09 November 2022: Articles 
Cantharidin-Podophyllin-Salicylic Acid Formulation as a First-Line Treatment for Plantar Warts? A Case Report with Multiple Plantar Warts of Human Papillomavirus Biotype 27 and Previous Failed Treatments
Unusual clinical course, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Unexpected drug reaction
David Navarro-PérezDOI: 10.12659/AJCR.937867
Am J Case Rep 2022; 23:e937867






Abstract
BACKGROUND: Plantar warts are benign skin tumors caused by the human papillomavirus (HPV). There are multiple treatments, but none ensure absolute success. Successful treatment depends on several factors, such as the location, number of lesions, HPV biotype, and the patient’s health condition. This report presents a 53-year-old woman who had multiple recalcitrant plantar warts with HPV biotype 27 that were treated using a cantharidin-podophyllin-salicylic acid (CPS) formulation after 2 failed treatments.
CASE REPORT: A 53-year-old woman was seen on October 25, 2021. She had 6 plantar warts due to HPV biotype 27, which was confirmed by polymerase chain reaction using a sample of hyperkeratosis scales obtained from the wart after debridement. Five cryotherapy sessions were applied, without clinical improvement. Two sessions of nitric-acid–zinc complex were then applied, from which the patient reported severe pain, without clinical improvement. Finally, 3 sessions of CPS formulation were applied, and the HPV remitted in all warts.
CONCLUSIONS: Conservative treatments, such as cryotherapy, have not been effective in a case of multiple recalcitrant plantar warts. The combined action of the 3 compounds of CPS formulation was key in the resolution of this case. Plantar wart treatment should be easy to apply, effective, fast, and efficient. In cases of recalcitrant or numerous warts, treatment should be more aggressive from the beginning if the patient’s lifestyle allows it. It would be interesting to conduct randomized clinical trials to find out which patients could be indicated for the CPS formulation as a first line of treatment.
Keywords: Cantharidin, conservative treatment, HPV L1 Protein, Human Papillomavirus, Warts, Female, Humans, Middle Aged, Papillomaviridae, Podophyllin, Alphapapillomavirus, Papillomavirus Infections, Salicylic Acid, Treatment Outcome
Background
Plantar warts are benign tumors caused by the human papillomavirus (HPV), which infects the cells of the epidermis [1,2]. HPV is an infiltrative and highly contagious virus, and due to the pressures produced on the sole of the foot, it tends to become embedded and penetrate the epidermis, surrounding itself with a hyperkeratotic coat [1,2]. This compresses underlying tissues, including nerve endings, which causes pain [1,2].
There are about 230 genotypes of HPV, of which genotypes 1, 2, 4, 10, 27, 57, and 63 are the most common on the soles of the feet [3,4]. The prevalence is around 79% in all age ranges, and it is most common in adolescents (9 to 16 years old) [5]. It is transmitted by direct contact, and the risk factors are the use of showers, swimming pools, and common spaces; living with patients who have warts; and immunosuppression or autoimmune diseases [6]. The characteristic clinical signs are hyperkeratosis, hemorrhagic stippling, loss of continuity of dermatoglyphics, and pain upon pinching [7,8]. The diagnosis is essentially clinical, and confirmation by microbiological culture or polymerase chain reaction (PCR) is recommended [4].
There are many types of treatments, which have different effects, aims, and methods of administration, but none of them ensure absolute success [9,10]. Success depends on many factors, such as the location, number of lesions, and health condition of the patient [9,10]. Another problem with HPV is that there is no antigen presentation to the immune system, unlike with other viruses [8]. This means that there is no immune response or inflammatory process, and HPV generates anti-inflammatory processes by activating suppressor T cells [8]. Therefore, even with an intact immune system, treatment is difficult [8].
The HPV biotype also influences the natural course and treatment response [11]. De Planell-Mas et al [12] observed differences in the time to development of warts based on the HPV genotype. In that study, warts belonging to the mu genus were mainly detected in less than 1 year, and warts belonging to the alpha genus were mainly detected over a long period of time [12].
Treatments should be inexpensive, simple, and painless, they should have no adverse effects, and they should offer immunity against the virus and resolution of all or most warts [9,10,13]. In other words, they should not affect the patient’s lifestyle, which should return to normal as soon as possible [9,10,13]. The fastest treatments are also the most aggressive, while the slowest are usually conservative, such as cryotherapy [9,10,13]. Usually, the initial treatments are the most conservative, and based on scientific evidence, the protocol involves 70% salicylic acid, nitric-acid–zinc complex (Verrutop®), cryotherapy (liquid nitrogen), cantharidin-podophyllin-salicylic acid (CPS) formulation, and surgical treatment [14,15].
Chemical treatment with salicylic acid ointment has been compared to cryotherapy in a randomized controlled clinical trial conducted with 229 patients [16]. However, the study observed low cure rates in both groups: 13.6% in the group treated with salicylic acid and 14.3% in the group treated using cryotherapy with liquid nitrogen [16]. A recent systematic review [15] showed that treatments have different cure rates (Table 1), and CPS formulation had the highest cure rate (97.82%) [15].
A narrative review by Lipke et al [17] suggests that there are much higher success rates with less widely tested approaches and combination therapies. A 2011 clinical trial showed 100% efficacy of CPS formulation compared to cryotherapy (41.7%) [18]. Case series published by Nguyen et al [19] and Lopez-Lopez et al [20] showed cure rates of 62.7% and 100%, respectively. In addition, Nguyen et al [19] reported a higher cure rate in children (86.5%).
This report presents a 53-year-old woman with multiple HPV biotype 27 plantar warts. All lesions were treated conservatively with cryotherapy and acids, but without success. Eventually, CPS formulation was applied, and there was complete healing. Therefore, the aim of this article is to generate discussion and promote future research on the treatment of recalcitrant warts by means of clinical trials.
Case Report
On September 16, 2021, a 53-year-old female patient came to the University Podiatric Clinic of the Complutense University of Madrid. HPV had been diagnosed on the ball of the hallux of her right foot, which had developed over several years. At her referral hospital, she had been treated with 10 sessions of cryotherapy from late 2019 to early 2020, but total remission was not achieved. She reported that multiple plantar warts had appeared on both feet since the summer of 2021 (Figure 1).
The patient reported no allergies or relevant medical history. She had no history of surgeries and was not taking any medication regularly. She had no risk factors and did not smoke or drink alcohol. After the clinical examination, we took a sample for culture and PCR to confirm the presence of HPV and to determine the biotype (Figure 2).
The diagnosis and biotype were confirmed using PCR from a hyperkeratosis scale sample that was obtained from the wart after debridement [4]. The sample was processed within 24 h after collection. The genomic DNA was extracted from the hyperkeratosis scales using an NZY Tissue gDNA Isolation kit (NZYTech), according to the manufacturer’s instructions, after 5 h of sample pre-lysis at 56°C [4]. DNA concentration was quantified after extraction at 260 nm using a Nanodrop 2000 spectrophotometer [4]. Nested PCR was performed using previously described primers and conditions. Sequences were analyzed using Sequencing Analysis software v.5.1 (Applied Biosystems), and the HPV sequence alignment was determined through comparison with known sequences in the GenBank database using BLASTn software [4].
On October 25, we were able to confirm the diagnosis. The final diagnosis comprised plantar warts caused by HPV biotype 27 on the ball of the hallux of the right foot with small satellite lesions around it, as well as on the ball of the second toe under the first metatarsal head and the heel of the same foot. The left foot had warts on the first metatarsal head and 2 on the heel. In total, the patient had 6 plantar warts.
The patient was offered the possibility of participating in a randomized clinical trial (RCT) (ClinicalTrials.gov Identifier: NCT04654091) that was currently taking place in our center to compare a nitric-acid–zinc complex and cryotherapy. The patient decided to participate in the study, and treatment was started with the application of liquid nitrogen cryotherapy using CryoPen b® (HO Equipments, Ghislenghien, Belgium). Cryopen® is an instrument that is used for the direct application of liquid N2O, which reaches temperatures of −89ºC. Once the hyperkeratotic tissue has been debrided [14], the device is used to evaporate the gas, projecting it onto the area to be treated. It should be applied at a distance of 0.5 to 4 mm from the wart at an angle of 45º until a whitish halo of 2 mm is observed around the wart.
Two 15-s applications are done per session with an interval of 30 s between each one, as recommended by the manufacturers. The lesion is then covered with a non-adherent dressing, and the patient is instructed to keep it on for 24 h. The application of liquid povidone-iodine once a day is recommended until the next check-up after 1 week, when a decision is made about whether to reapply the product, according to the development of the lesion. The maximum number of sessions of product application is 5, based on previous studies [13].
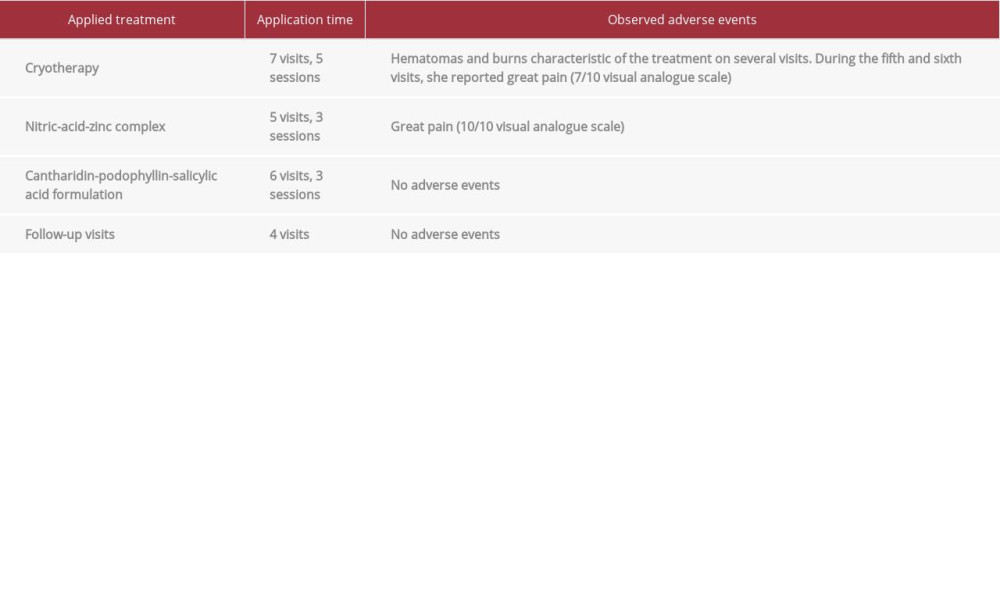
The treatment consisted of the application of cryotherapy on a weekly basis, alternating 1 foot per week. In each session, two 15-s applications were done on each plantar wart. During the 7 cryotherapy visits, there was no great improvement in signs and symptoms on 5 occasions, and several plantar warts disappeared and returned on subsequent visits. In several visits, the patient presented hematomas and burns that are characteristic of the treatment, and during the fifth and sixth visits, she reported great pain (7/10 visual analogue scale).
Having completed 5 cryotherapy sessions of the RCT without showing clear improvement, we decided to change the treatment. The protocol involved 70% salicylic acid, nitric-acid–zinc complex (Verrutop®), cryotherapy (liquid nitrogen), CPS formulation, and surgical treatment [15]. The nitric-acid-zinc complex was applied on the same day to both of the first metatarsal heads, the ball of the hallux, and the heel of the right foot. The nitric-acid–zinc complex (Verrutop®) is an aqueous solution of organic acids (lactic, oxalic, and acetic acid), nitric acid, zinc, and copper salts. The effect occurs through mummification of the wart tissue, leading to its detachment once healthy skin is formed, and it also reduces the amount of HPV DNA.
After scalpel debridement of the keratinized surface of the wart, the product was applied using small touches with a capillary containing it. The lesion was then covered with a nonadherent dressing, and the patient was instructed to clean the area each day with 70% alcohol to reactivate the product until check-up in the following week. At that time, a decision was made about whether to reapply the product according to the development of the lesion.
One week later, the patient came to the clinic with severe pain (9/10 visual analogue scale) in the days following the application. The nitric-acid–zinc complex was reapplied to all of the plantar warts, and the patient was in great pain for that week. We thought that the patient’s pain was generated by the high sensitivity of the skin due to the time over which the patient had been treated. Therefore, we decided not to apply treatment for 2 weeks to allow the skin area to regenerate. After 2 weeks, the nitric-acid-zinc complex was applied for a third time, which caused the patient much pain (10/10 visual analogue scale). Thus, we decided to cancel the session.
This was the second turning point in the treatment of the patient’s plantar warts. Some doubts began to appear because we had been treating the patient for 12 weeks, 5 months had passed since the first consultation, and we had not made much progress. Therefore, at visit 13, we decided to start with the application of 1% cantharidin, 30% salicylic acid, and 5% podophyllin (CPS formulation) on the first metatarsal head of the left foot after debridement.
CPS should be prescribed as a formulation that is applied by swabbing the entire surface of the plantar wart and covered with an impermeable occlusive dressing for the tissue to macerate to increase the therapeutic effect. The treatment was maintained for 72 h, followed by liquid povidone-iodine treatment until the next visit, when all affected tissue not adhering to the remaining skin was debrided. The application can be repeated 1 or 2 more times to obtain good results (Figure 3A, 3B) [18,21]. The key to treatment using this formulation is that it combines the action of 3 compounds. The keratolytic and caustic action of salicylic acid acts against hyperkeratosis and surrounding skin, the vesicant action of cantharidin acts against the wart, and the podophyllin inhibits cell mitosis and interrupts the process of cell division, preventing the advance and development of HPV [18,21].
Owing to the pain, the blisters caused by this treatment, and the presence of warts in different locations on the soles of both feet of the patient, we decided to treat them one by one at different visits to avoid affecting the patient’s walking. At the next visit, we observed the tissue, which showed the characteristic papillae of plantar warts, and treated them using liquid povidone-iodine. At visit 15, we applied the treatment to the 2 plantar warts on the heel of the left foot. At visit 16, not only did we see improvement in the treated plantar warts, but also the warts on the right foot began to improve in both signs and symptoms without having applied any treatment to them (Figure 3C–3F). At subsequent visits, only the ball of the right hallux was treated, as the remaining warts had improved without treatment during that period.
On March 29, we concluded the treatment for plantar warts, but fearing the possibility of a recurrence, we decided to set up a series of follow-up visits. A week later, we observed that both feet were in good condition and recommended the application of hydrating cream to the hyperkeratotic areas. We also made another appointment a month later, at which time both feet were in perfect condition (Figure 4). After 22 visits distributed over 8 months, we discharged the patient and scheduled a visit after 3 months for a check-up (Table 2).
Discussion
Eight sessions of conservative treatments of cryotherapy or nitric-acid–zinc complex for 12 weeks were ineffective for a 53-year-old woman with multiple recalcitrant HPV biotype 27 plantar warts with several months of development. However, 3 applications of the CPS formulation at different sites achieved resolution of all plantar warts. In this clinical case, the treatment consisted of 3 phases. In the first phase, the patient was treated with cryotherapy, which showed slow but positive development, bordering on stagnation, but without worsening. This is also what happened 2 years prior when the patient was treated with cryotherapy for 10 sessions.
In the second phase, the patient was treated with the nitric-acid-zinc complex and had much pain (9/10 visual analogue scale), without any results to compensate for the pain. At this point, we had to decide how to approach the treatment, as the next step would be to use the CPS formulation; however, we were uncertain due the fact that the patient had 5 active plantar warts. Eventually, we decided to treat 1 plantar wart per visit so as not to cause severe injuries or impede the patient’s walking. As a result, positive development was observed not only in the treated lesions, but also in those that were not treated. Based on the data, we questioned whether all plantar warts should be treated from the beginning with more aggressive treatments, such as the CPS formulation.
García-Oreja et al (2021) [15] conducted a systematic review and observed that first-line treatments for plantar warts, such as salicylic acid or cryotherapy, have low cure rates (13.6% and 45.61%, respectively). Previous clinical trials, such as that by Cockayne et al [16], also found very low cure rates with salicylic acid (13.6%) or cryotherapy (14.3%). Other more aggressive treatments included in the conservative group were more effective, such as CPS formulation (97.82%), laser treatment (79.36%), and intralesional bleomycin (83.37%), among others [15]. Other studies, such as that by Kaçar et al [18], showed 100% efficacy of CPS formulation compared to cryotherapy (41.7%). In a case series, Nguyen et al [19] and Lopez-Lopez et al [20] showed cure rates of 62.7% and 100%, respectively.
Given the high efficacy of the CPS formulation, it would be tempting to treat all plantar warts with this formula, but this is not appropriate as it can cause great pain, blisters, and large injuries [15]. Patients who work all day in a standing position, athletes, and people who are very sensitive to pain would not be candidates for this treatment [15]. The main contraindications of CPS formulation are allergies to the components of the product, elderly patients, and immunosuppressed patients [22]. Due to the risk of ulceration, it is not indicated for patients with diabetes or for those with peripheral vascular disease [22]. Finally, it is also not indicated in lactating women and children less than 5 years of age owing to the absence of safety data [22].
On the other hand, we must bear in mind that treatments should affect the patient’s lifestyle as little as possible [20,23,24]. For this patient, we carried out 22 consultations with different treatments, which was equivalent to approximately 8 months of discomfort from plantar warts, pain from the treatments, worsening of the patient’s mood as she saw that they were not improving, time spent going to the doctor, and a general decrease in quality of life.
As for how to apply the CPS formulation, it would be interesting to quantify the dose that is applied according to certain criteria, as we have observed that this formulation generates larger lesions in some patients than in others. Finally, we must be careful with the treatment that we choose, and it is necessary to follow an action protocol, but we must also be as efficient as possible. Thus, we may have to carry out more aggressive treatments from the beginning.
Conclusions
More conservative treatments, such as cryotherapy and nitric-acid-zinc complex, have not been effective in a case of multiple recalcitrant plantar warts of several months of development. The combined action of the 3 compounds of the CPS formulation was key in the resolution of this case because it was not necessary to treat all the plantar warts for their resolution due to the activation of the immune system against the papilloma-virus. Plantar wart treatment should be easy to apply, effective, fast, and efficient, with the aim of returning the patient to normal activity as soon as possible. In the case of recalcitrant or numerous warts, we should be more aggressive from the beginning of treatment if the patient’s lifestyle allows it in cases of multiple plantar warts, previously unsuccessful treatment, recurrence, or a long history of disease. It would be interesting to carry out RCTs to find out which patients could be indicated for the CPS formulation as a first line of treatment. Nevertheless, it is important to maintain long-term follow-up to avoid recurrence.
Figures
![Cure rates of the main treatments for plantar warts [15].](https://jours.isi-science.com/imageXml.php?i=t1-amjcaserep-23-e937867.jpg&idArt=937867&w=1000)
References:
1.. Fernández Domínguez H, Mosquera Fernández A, Monteagudo Sánchez B, Revisión bibliográfica de los tratamientos de la verruga plantar: Rev Esp Podol, 2014; 25(4); 138-41 [in Spanish]
2.. Zalacaín A, Ogalla J, García-Patos V: Atlas y sinopsis de enfermedades cutáneas del pie, 2008, Madrid, EdikaMed S.L [in Spanish]
3.. Wolff K J, Suurmond D: Fitzpatrick’s, color atlas & synopsis of clinical dermatology, 2005, Philadelphia, McGraw-Hill
4.. García-Oreja S, Álvaro-Afonso FJ, Sevillano-Fernández D, A non-invasive method for diagnosing plantar warts caused by human papillomavirus (HPV): J Med Virol, 2021; 94(6); 2897-901
5.. Sterling JC, Handfield-Jones S, Hudson PM, Guidelines for the management of cutaneous warts: Br J Dermatol, 2001; 144(1); 4-11
6.. Ciconte A, Campbell J, Tabrizi S, Warts are not merely blemishes on the skin: A study on the morbidity associated with having viral cutaneous warts: Australas J Dermatol, 2003; 44(3); 169-73
7.. Aubin F, Pretet JL, Mougin C, Riethmuller D, Infection a papillomavirus humains: Ann Dermatol Vénerol: Elsevier, 2007; 134; 94-99
8.. Hashmi F, Bristow I, Treating plantar warts: Utilising natural immunity to induce wart regression: Dermatological Nursing, 2014; 13(1); 42-45
9.. Kumari P, Yadav D, Vijay A, Falknor’s needling method as a potential immunotherapy in palmo-plantar warts: Indian J Dermatol Venereol Leprol, 2019; 85; 129
10.. Alcalá Sanz J, Aranda Bolívar Y, Ahumada Bilbao J, Cantaridina. Revisión bibliográfica como tratamiento de las verrugas plantares: Rev Esp Podol, 2011; 22(3); 107-11 [in Spanish]
11.. Bruggink SC, Gussekloo J, de Koning MN, HPV type in plantar warts influences natural course and treatment response: Secondary analysis of a randomized controlled trial: J Clin Virol, 2013; 57(3); 227-32
12.. De Planell-Mas E, Martínez-Garriga B, Zalacain AJ, Human papilloma-viruses genotyping in plantar warts: J Med Virol, 2017; 89(5); 902-7
13.. García-Oreja S, Álvaro-Afonso FJ, Tardáguila-García A, Efficacy of cryo-therapy for plantar warts: A systematic review and meta-analysis: Dermatol Ther, 2022; 36(5); e15480
14.. Becerro de Bengoa Vallejo R, Losa Iglesias ME, Gómez-Martín B, Sánchez Gómez R SCA, Application of cantharidin and podophyllotoxin for the treatment of plantar warts: J Am Pod Med Assoc, 2008; 98(6); 445-50
15.. García-Oreja S, Álvaro-Afonso FJ, García-Álvarez Y, Topical treatment for plantar warts: A systematic review: Dermatol Ther, 2021; 34(1); e14621 Erratum in: Dermatol Ther. 2021;34(2):e14941
16.. Cockayne S, Hewitt C, Hicks K, Cryotherapy versus salicylic acid for the treatment of plantar warts (verrucae): A randomised controlled trial: Br Med J, 2011; 342; d3271
17.. Lipke MM, An armamentarium of wart treatments: Clin Med Res, 2006; 4(4); 273-93
18.. Kaçar N, Taşlı L, Korkmaz S, Cantharidin-podophylotoxin-salicylic acid versus cryotherapy in the treatment of plantar warts: A randomized prospective study: J Eur Acad Dermatol Venereol, 2012; 26(7); 889-93
19.. Nguyen AL, Quint KD, Bouwes Bavinck JN, Real-life treatment of cutaneous warts with cantharidin podophyllin salicylic acid solution: Dermatol Ther, 2019; 32(6); e13143
20.. López D, Vilar Fernández JM, Losa Iglesias ME, Safety and effectiveness of cantharidin-podophylotoxin-salicylic acid in the treatment of recalcitrant plantar warts: Dermatol Ther, 2016; 29(4); 269-73
21.. López-López D, Agrasar-Cruz C, Bautista-Casasnovas A, Álvarez-Castro CJ, Application of cantharidin, podophyllotoxin, and salicylic acid in recalcitrant plantar warts. A preliminary study: Gac Med Mex, 2015; 151(1); 14-19
22.. Gómez-Ortiz S, Gomez-Facundo S: Guía farmacológica podología 2016, 2016, Barcelona, Nexus Médica [in Spanish]
23.. Torbeck R, Pan M, DeMoll E, Levitt J, Cantharidin: A comprehensive review of the clinical literature: Dermatol Online J, 2014; 20(6); 13030 /qt45r512w0
24.. Vakharia PP, Chopra R, Silverberg NB, Silverberg JI, Efficacy and safety of topical cantharidin treatment for molluscum contagiosum and warts: A systematic review: Am J Clin Dermatol, 2018; 19(6); 791-803
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953110
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952798
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952736
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953993
Most Viewed Current Articles
07 Dec 2021 : Case report
22,757,193
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,264
175,264
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,171
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,170
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133