11 January 2023: Articles 
Venous Stent Placement for Malignant Vena Cava Syndrome in a Patient with Liposarcoma
Unusual setting of medical care, Rare disease
Shunya Shiohira1ABCDEF, Toshihiko Sugiura2ABCDEF, Hideki Ikeda2BCDE, Shunichiro Iwasawa3ABCDE, Yuto Akimoto2BCD, Hajime Kasai2ABCDEF*, Kohei Shikano2BCD, Aoi Hino2BCDE, Atsushi SaigaDOI: 10.12659/AJCR.938311
Am J Case Rep 2023; 24:e938311






Abstract
BACKGROUND: Reports of venous stenting for inferior vena cava (IVC) syndrome (IVCS) due to sarcoma are limited, and the treatment’s efficacy and safety are not clear.
CASE REPORT: A 36-year-old woman with myxoid liposarcoma was admitted to the Department of Respiratory Medicine for treatment of bilateral lower-leg edema and to be evaluated for acute liver dysfunction. She was 13 years old when she was diagnosed with myxoid liposarcoma. Over the next 18 years, she had 4 tumor resections and 1 round of radiation therapy. She had been on chemotherapy for 4 years and then pazopanib at the age of 35. The edema did not improve after admission despite treatment with diuretics. Computed tomography revealed a huge liposarcoma occupying the right thoracic cavity and a compressed IVC, which caused the edema. Although doxorubicin was administered as fifth-line treatment, there was no response. Since there was no additional chemotherapy regimen, her prognosis was considered to be less than 6 months. She could not be discharged to her home since she was unable to walk due to the edema; therefore, IVC stenting was performed to improve her dysmotility. After IVC stenting, the lower-leg edema improved without any adverse events, enabling her to walk and eventually return home.
CONCLUSIONS: In patients with IVCS caused by rare malignancies such as myxoid liposarcoma, an IVC stent can be safely implanted and can help to alleviate symptoms. IVC stenting can improve symptoms and allow for home care, resulting in improved quality of life.
Keywords: Edema, Liposarcoma, Stents, Vena Cava, Inferior, Female, Adult, Humans, Adolescent, Liposarcoma, Myxoid, Quality of Life, Vascular Diseases, Treatment Outcome
Background
Vena cava syndrome is a complication of progressive malignant cancer. Enlarged tumors compress the vena cava, interrupting venous return and causing several symptoms [1]. Vena cava syndrome is classified into superior vena cava (SVC) syndrome (SVCS) and inferior vena cava (IVC) syndrome (IVCS). SVCS is caused by the obstruction of the SVC and is usually secondary to malignancy such as lung cancers or mediastinal tumors [1,2]. IVCS is mainly caused by metastatic liver tumors [1], and primary tumors are rare [3]. Stenting is indicated for symptomatic IVC stenosis that is refractory to treatment of the underlying disease [4]. This may be more useful for symptomatic relief and earlier symptomatic improvement than radiation therapy or anticancer drugs. Liposarcomas are rare, malignant tumors of adipocytic differentiation [5]. The treatment options include surgery, chemotherapy, and radiation therapy, and the disease can recur in some cases. The reports of venous stenting for vena cava syndrome due to sarcoma are limited, and its efficacy and safety are not clear.
We present a case of malignant vena cava syndrome in a liposarcoma patient who received venous stent placement.
Case Report
A 36-year-old woman with myxoid liposarcoma was admitted to our department for treatment of prominent lower-leg edema and to be evaluated for acute liver dysfunction. At the age of 13, she underwent an excision of a large tumor that had completely occupied the right thoracic cavity, and she was diagnosed with myxoid liposarcoma. She underwent 1 round of radiation therapy and 4 tumor resections over the course of 18 years. The tumor grew markedly again when she was 31 years old, and was determined to be inoperable. At 31 years old, she was administered doxorubicin as first-line treatment, eribulin as second-line treatment at 33 years old, and trabectedin as third-line treatment at 35 years old. However, the tumor grew gradually over time. She was administered pazopanib as fourth-line treatment at 35 years old. She continued pazopanib for 5 months before being admitted to our department.
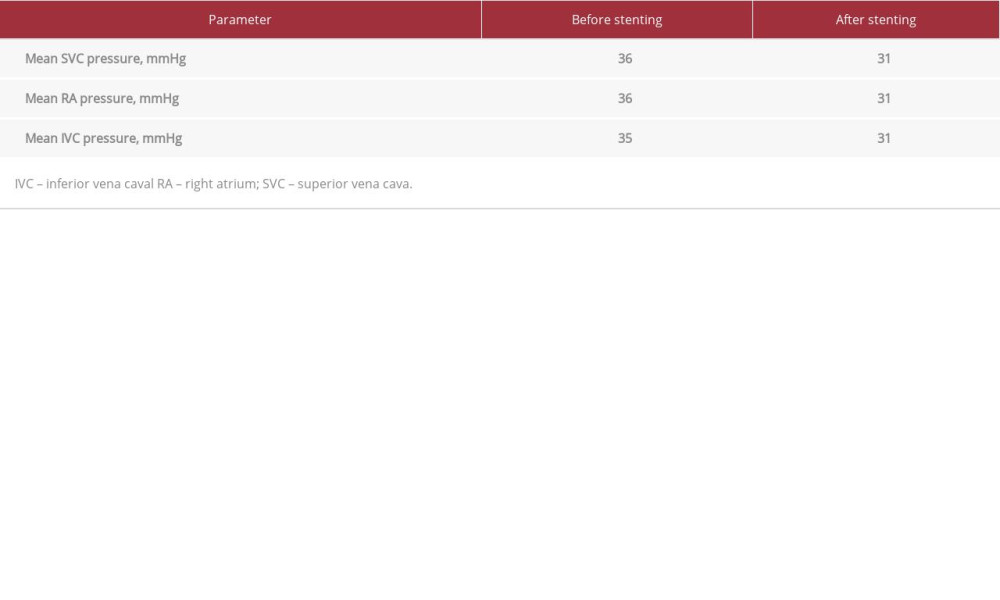
At the time of admission, her weight was 48.7 kg and her height was 158 cm. Her vital signs were as follows: Glasgow Coma Scale, 15 (E4V5M6); blood pressure, 116/81 mmHg; pulse rate, 59 beats/min; pulse oximetry, 99% with nasal cannula oxygenation at 2 L/min; respiratory rate, 12/min; and body temperature, 36.5°C. Physical examination revealed decreased respiratory sounds in the right thoracic region and prominent lower-leg edema (Figure 1A). Blood examination revealed an aspartate aminotransferase level of 1100 U/L, an alanine aminotransferase level of 438 U/L, and total bilirubin level of 7.2 mg/dL. Pazopanib was discontinued because it was suspected of causing liver dysfunction. Glycyrrhizin acid was administered after the admission. After 12 days of glycyrrhizin administration, liver dysfunction gradually improved. The liver function almost normalized, except for lactate dehydrogenase and alkaline phosphatase levels, about 2 months after admission. Furosemide and tolvaptan were administered to improve the edema, but it did not improve. Computed tomography (CT) revealed a huge liposarcoma occupying the right thorax and surrounding the IVC (Figure 2). Furthermore, the tumor had compressed the IVC, causing the edema (Figure 2A'). Although doxorubicin was administered as fifth-line treatment on hospitalization days 48 and 72, there was no response (Figure 3). Since there were no additional anticancer drug choices, her prognosis was considered to be less than 6 months. However, as she was unable to walk due to the edema, she could not be discharged to her home. Since the liposarcoma was a highly locally advanced tumor, local treatment such as radiotherapy and IVC stenting was discussed. Since the liposarcoma was considered to have poor sensitivity to radiotherapy, it was not considered to be sufficiently effective. However, since liposarcoma is a relatively soft tumor, stenting was considered to improve blood flow to the IVC. IVC stenting was performed to improve the edema-induced dysmotility. With informed consent from the patient, a 14F sheath (Cook-Z Stent Vena Caval and Venous Design Radiopaque Band Introducer Set; William Cook, Bjaeverskov, Denmark) was inserted into the right common femoral vein and a 5F sheath (Super Sheath; Medikit, Tokyo, Japan) was inserted into the right basilic vein, due to her right internal carotid artery stenosis. IVC venography revealed IVC stenosis due to the tumor (Figure 4A, 4B). A 0.035-inch guidewire (Radiforcus Guide Wire; Terumo, Tokyo, Japan) was passed through the stenosis. The guidewire was captured by a 12–20-mm snare (EnSnare; Merit Medical, South Jordan, UT, USA) in the SVC and was pulled out via a 5F sheath in the right basilic vein; “pull-through” was achieved. Then, a stent delivery system was inserted beyond the site. A self-expandable metallic bare stent, 20 mm in diameter and 8 cm in length (Spiral Relief Stent; Cosmotec, Tokyo, Japan), was placed across the stenotic site. Angioplasty using a balloon catheter (20 mm×4 cm; Maxi LD, Cordis, CA, USA) was performed over the region of greatest stenosis. The stenosis was dilated with a balloon catheter while viewing the vessel morphology with sheath angiography (Figure 4C, 4D). Venography was then performed to confirm the improvement of blood flow in the IVC. Pressures in the IVC, RA, and SVC decreased mildly after stenting. However, there were no pressure gradients in the IVC before and after stenting (Table 1). Furthermore, an enhanced CT and three-dimensional images by the enhanced CT showed that the stent was placed in the IVC between the liver and the heart, sandwiched between the tumors (Figures 5, 6). The lower-leg edema improved (Figures 1B, 6) after IVC stenting, and she was able to walk again within a few days. The liver function, which had improved other than mild elevation of serum lactate dehydrogenase and alkaline phosphatase levels before the stenting, did not show deterioration after the stenting. She was then discharged from the hospital on day 144 of her stay. She spent approximately 1 month at home without any complications from the IVC stenting; unfortunately, she died of respiratory failure due to increased sputum.
Discussion
The present case demonstrates 2 notable clinical findings. First, IVC stenting can be safely introduced even for IVCS due to rare malignancies such as liposarcoma. Second, IVC stenting can provide marked improvement in leg edema caused by IVCS, and can be useful in improving quality of life (QOL), even in patients with liposarcoma.
IVC stenting can help with a variety of symptoms caused by IVCS due to rare malignancies such as liposarcoma and can be safely implanted. Although the complication rate of stent placement for vena cava obstruction is relatively low, vena cava rupture, venous perforation, stent migration, and embolism [6] are all potential risks. The number of patients eligible for IVC stenting is limited, and a safe implantation method has not been established. Increased serum bilirubin can increase risk of clinical failures and recurrences of IVC stenting for IVCS [7]. Furthermore, IVC stenting with a safety margin, not only at the stenosis site, can be useful to prevent restenosis [3]. In the present case, a guide wire was extended to the right upper arm from the right femoral vein to prevent migration of the stent into the right heart during implantation. After the stent was placed in the stenotic area, it was dilated with a balloon catheter while viewing the vessel morphology with sheath angiography. As a result, there were no complications during the procedure or during the first month after implantation.
IVCS is often caused by intrahepatic compression due to liver metastases or hepatic metastases, but can also be caused by extrahepatic compression by various tumors. However, the difference of effect between intrahepatic stenting for IVCS due to hepatic tumors/metastasis lesions and extrahepatic stenting for IVCS due to extrahepatic/retroperitoneal tumors has not discussed. Although there were several original articles on IVC stenting for IVCS, there was no detailed information on how tumors compress and/or narrow the IVC, and no mention of differences in response to treatment based on the underlying disease and site of stenosis [3,7–12]. Although there have been case reports of IVSC caused by extrahepatic compression due to lymph node metastasis of colon cancer and retroperitoneal Kaposi’s sarcoma, the compression of IVC occurred in areas peripheral to the liver [1,13]. Our case involved intrahepatic and extrahepatic compression of the IVC from the liver to the right heart by liposarcoma. There are no reports detailing IVCS due to extrahepatic compression from the liver to the right heart as in our case. Further case accumulation is needed to evaluate the efficacy of IVC stenting between intrahepatic and extrahepatic IVCS.
In a Phase III trial evaluating the efficacy of stenting for vena cava syndrome, 18 patients with SVCS and 14 patients with IVCS were randomly assigned to a stenting group or a control group [12]. The primary endpoint of the study was improvement in symptom scores based on interviews, which revealed significant improvement before and after implantation in overall cases, including IVC and SVC stenosis cases. The secondary endpoint was a QOL evaluation, which compared the improvement in 2 QOL scores, the EQ-5D and SF-8, before and after stenting. There was no significant improvement in QOL scores in overall cases; however, SF-8 showed a significant improvement only in IVCS cases. Furthermore, it should be noted that the overall population had a very limited prognosis, with a median survival of 67 days, and the study found that vena cava stenting did not improve survival in patients with SVCS and IVCS. As the safety of long-term implantation has not yet been established, only patients with no other treatment options for causative disease and limited prognosis should be considered. IVCS is caused by hepatic or retroperitoneal tumors, and can also be caused by a variety of tumors due to hepatic metastasis and/or extension around the IVC. Only 1 case of liposarcoma was included in a previous study [12], while no details were given as to the course and whether the IVC stent was effective for the IVCS. In our case, there were no additional anticancer drug choices, and her prognosis was considered to be less than 6 months. Moreover, due to significant edema, she was unable to walk and could not be discharged home.
Symptom palliation with IVC stenting enables home care and contributes to improvement in QOL. Therefore, IVC stenting should be considered in IVCS patients with limited prognosis.
Conclusions
IVC stents can be safely implanted in patients with IVCS caused by rare malignancies such as giant myxoid liposarcoma and can improve symptoms. Improvement in symptoms with IVC stenting can allow for home care, thereby contributing to an improved QOL, even with rare tumors.
Figures
References:
1.. Morita S, Sugawara S, Suda T, Stent placement for malignant inferior vena cava syndrome in a patient with recurrent colon cancer: Intern Med, 2020; 59; 2885-90
2.. Azizi AH, Shafi I, Shah N, Superior vena cava syndrome: JACC Cardiovasc Interv, 2020; 13; 2896-910
3.. Kuetting D, Thomas D, Wilhelm K, Endovascular management of malignant inferior vena cava syndromes: Cardiovasc Intervent Radiol, 2017; 40; 1873-81
4.. Klein-Weigel PF, Elitok S, Ruttloff A, Inferior vena cava-syndrome: Vasa, 2021; 50; 250-64
5.. Bower TC, Nagorney DM, Cherry KJ, Replacement of the inferior vena cava for malignancy: An update: J Vasc Surg, 2000; 31; 270-81
6.. , Stent placement for vena caval obstruction, 2004 Available from: https://www.nice.org.uk/guidance/ipg79.7
7.. Brountzos EN, Binkert CA, Panagiotou IE, Clinical outcome after intrahepatic venous stent placement for malignant inferior vena cava syndrome: Cardiovasc Intervent Radiol, 2004; 27; 129-36
8.. Augustin AM, Lucius LJ, Thurner A, Kickuth R, Malignant obstruction of the inferior vena cava: Clinical experience with the self-expanding Sinus-XL stent system: Abdom Radiol (NY), 2022; 47; 3604-14
9.. Devcic Z, Techasith T, Banerjee A, Technical and anatomic factors influencing the success of inferior vena caval stent placement for malignant obstruction: J Vasc Interv Radiol, 2016; 27; 1350-60.e1
10.. Oudkerk M, Heystraten FM, Stoter G, Stenting in malignant vena caval obstruction: Cancer, 1993; 71; 142-46
11.. Sebastian T, Dopheide JF, Engelberger RP, Outcomes of endovascular reconstruction of the inferior vena cava with self-expanding nitinol stents: J Vasc Surg Venous Lymphat Disord, 2018; 6; 312-20
12.. Takeuchi Y, Arai Y, Sone M, Evaluation of stent placement for vena cava syndrome: Phase II trial and phase III randomized controlled trial: Support Care Cancer, 2019; 27; 1081-88
13.. Gasparis AP, Kokkosis A, Labropoulos N, Venous outflow obstruction with retroperitoneal Kaposi’s sarcoma and treatment with inferior vena cava stenting: Vasc Endovascular Surg, 2009; 43; 295-300
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133