28 August 2024: Articles 
Malignant Pericardial Effusion from Cervical Squamous Cell Carcinoma: A Case Study
Challenging differential diagnosis, Educational Purpose (only if useful for a systematic review or synthesis), Rare coexistence of disease or pathology
Sunder Sham1AEF*, Saroja Devi Geetha2EF, Alae Kawam3AB, Ahmed Bendari1E, Reham Al-Refai1E, F.N.U. Anjali4E, Manju Harshan1A, Kasturi Das2AEDOI: 10.12659/AJCR.943013
Am J Case Rep 2024; 25:e943013






Abstract
BACKGROUND: Cervical cancer ranks fourth globally among women’s cancers. Squamous cell carcinoma constitutes 70% of cervical cancer cases, often metastasizing to lungs and paraaortic nodes. Uncommon sites include the brain, skin, spleen, and muscle, while pericardial fluid metastasis is highly rare. We report a case of squamous cell carcinoma of the uterine cervix that was metastatic to the pericardium and was detected on cytologic evaluation of pericardial fluid.
CASE REPORT: A 42-year-old woman who was previously treated for stage III squamous cell carcinoma of the cervix presented with symptoms of cough, fever, and shortness of breath for 8 days, and chest pain for 3 days. Clinical workup revealed pericardial effusion, with spread to the lungs and mediastinal and hilar lymph nodes. Cytological analysis of the fluid showed malignant cells, consistent with metastatic squamous cell carcinoma. Immunohistochemistry demonstrated cells positive for p63 and p40, while negative for GATA-3, D2-40, calretinin, and WT1. These findings in conjunction with patient’s known history of cervical squamous cell carcinoma was consistent with a cytologic diagnosis of metastatic squamous cell carcinoma to pericardial fluid.
CONCLUSIONS: History and clinical correlation plays a vital role in determining the primary site causing malignant pericardial effusions. While the occurrence of cervical cancer metastasizing to the pericardium is uncommon, it should be considered, particularly in cases involving high-grade, invasive tumors, recurrences, or distant metastases. This possibility should be included in the list of potential diagnoses when encountering pericardial effusions with squamous cells in female patients.
Keywords: Neoplasm Metastasis, Neoplasms, Squamous Cell, Pericardial Effusion, Uterine Cervical Neoplasms, Humans, Female, Carcinoma, Squamous Cell, adult, Heart Neoplasms
Introduction
Pericardial effusion results from diverse factors, including idiopathic cases, malignancy, uremia, iatrogenic factors, post-acute myocardial infarction situations, and infections. Malignancy contributes 13% of all cases [1]. Malignant pericardial involvement has been reported in 1% to 20% of cancer autopsies, with lung, breast, esophagus, melanoma, lymphoma, and leukemia as common sites of origin [2].
Cervical cancer is the fourth most common malignant tumor in women globally, with an annual mortality rate of approximately 311 000 deaths [3]. The disease metastasizes into surrounding tissues or distant organs by either direct filtration and/or by lymphatic and hematogenous pathways [4]. Cardiac metastasis from cervical cancer is extremely rare, with an estimated incidence of 1.23%, based on autopsy findings [5]. The diagnosis is typically made on post-mortem examination; only few cases of antemortem diagnosis of malignant pericardial effusion secondary to cervical carcinoma have been reported so far [6,7]. This could be due to low index of suspicion, asymptomatic involvement, and lack of advanced diagnostic techniques. The prognostic outlook subsequent to cardiac metastasis is unfavorable, and the most extended reported survival period following diagnosis is 13 months [8].
Here, we present a unique case of cervical carcinoma that metastasized to the pericardium, resulting in malignant pericar-dial effusion. The narrative delves into the pathological observations and cytomorphologic findings, with a focus on the use of immunohistochemistry (IHC) to distinguish from other close entities presenting with pericardial metastasis.
Case Report
A 42-year-old woman with history of stage III squamous cell carcinoma of the cervix and chemotherapy and radiation therapy presented with symptoms of cough, fever, and shortness of breath for 8 days, and chest pain for 3 days. The patient underwent a transthoracic echocardiogram, which revealed the presence of lesions in the lung, mediastinal and hilar lymph-adenopathy, and pericardial effusion. Pericardiocentesis was performed, and fluid samples were sent for cytopathologic evaluation. Cytopathology from pericardial fluid showed numerous pleomorphic cells present both as syncytial groups and isolated cells, with hyperchromatic nuclei and scant dense cytoplasm in a background of macrophages (Figures 1–3). Cell block demonstrated sheets of cells with hyperchromatic, enlarged nuclei, irregular nuclear contours, high nuclear to cytoplasmic ratio, and scant cytoplasm (Figure 4). On IHC, the malignant cells expressed p63, p40 (Figure 5), and were negative for GATA-3, D2-40, calretinin, and WT1. These morphologic and IHC features in conjunction with the history of squamous cell carcinoma of the cervix were compatible with metastatic cervical squamous cell carcinoma.
Discussion
Approximately 70% of cervical cancers are of squamous cell lesions [9] and are associated with human papillomavirus (HPV) [10]. Individuals harboring co-infections with other sexually transmitted organisms face an elevated risk of developing invasive cervical carcinoma. This risk is further heightened by recurrent cervicitis, oral contraceptive usage, tobacco consumption, and a compromised immune system [11]. In most cases, absence of these additional risk factors usually results in low-grade HPV infection, which usually self-resolves [10].
Although screening for cervical carcinoma has greatly reduced morbidity and mortality, this carcinoma is known to metastasize or recur. The recurrence rate of cervical carcinoma in women with no lymph node involvement following surgical intervention or radiotherapy is 10% to 20%. However, the recurrence rate stands at 70% in women who have had nodal metastasis. Metastasis of cervical carcinoma can occur via the lymphatic route or the hematogenous route, with the hematogenous route occurring more commonly in advanced stages, through the paracervical veins and the venous plexuses. The sites that are most commonly affected by distant metastasis are the lungs, which comprise 21% of distant metastatic sites, the para-aortic nodes, comprising 11%, the abdominal cavity, 8% and finally the supraclavicular nodes, which make up 7% of distant metastasis [4]. Unusual sites of metastasis include the breast, skin, soft tissue, umbilicus, and oral cavity [12]. In most cases, metastases occurs within 2 years of diagnosis [4]. The median survival time for metastatic cervical carcinoma is approximately 8 to 13 months. The 5-year survival rate is 16.5%. Furthermore, individuals exhibiting multi-site metastasis typically experience a markedly diminished survival rate than do patients with metastasis limited to a single site. [13].
Cardiac metastasis of cervical carcinoma is a very rare occurrence, with a reported incidence rate of approximately 1.23%. Due to the rarity of the condition, most cases are often discovered during autopsies. Very rarely, antemortem diagnosis of cardiac metastases is made. Prognosis is usually poor, with the longest reported survival being 13 months [5]. The primary locus of metastasis to the heart from cervical carcinoma predominantly involves the pericardium, accounting for 64% of all cardiac metastases, followed by the myocardium and endocardium. Intraventricular metastases have also been reported. Almost all intraventricular metastases occur in the right chamber [5].
Patients typically present with symptoms of pleuritic pain, cough, dyspnea, fatigue, and syncope. The mean age of diagnosis of pericardial effusion in the context of cervical carcinoma is 52 years. Diagnosis is made mostly in patients who have had prior identification of the primary tumor [14].
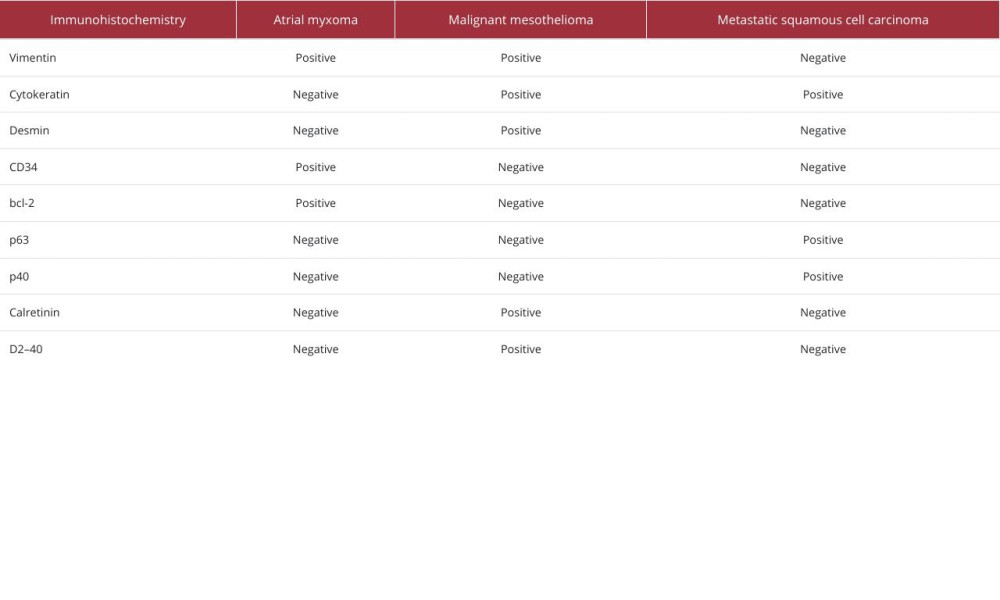
Cytological evaluation of the pericardial fluid is effective to assess for the presence of malignant cells. Indeed, cytological evaluation of pericardial fluid is a much better diagnostic tool for metastatic pericardial lesions than pericardial biopsies. Cytological evaluation has a false negativity rate of 14.7%, whereas the use of pericardial biopsy has a reported false negativity rate of 40% [15]. The differential diagnosis of cardiac metastases are thrombi, cardiac vegetations, and primary cardiac tumors, such as atrial myxoma, primary pericardial malignant mesothelioma [15,16]. Many times, it can be challenging to achieve a definitive diagnosis based solely on cyto-morphologic findings. In such context, application of IHC stains has demonstrated utility. Atrial myxomas are the most common primary tumors of the heart and typically present as a single, gelatinous, well-circumscribed mass [17]. Cytologic analysis of pericardial fluid reveals tumor cells that are spindle-shaped or polygonal, often with abundant cytoplasm and hyperchromatic nuclei [17]. In cases of malignant mesothelioma, the malignant cells usually form large clusters with a knobby, scalloped contour, referred to as mulberry clusters. The individual cells forming the clusters demonstrate cytomegaly, with a normal nuclear-cytoplasmic ratio. The nucleus is round and centrally located, with a prominent nucleolus. Binucleated and multinucleated cells are common [18]. Table 1 describes the IHC findings of atrial myxoma, malignant mesothelioma, and metastatic squamous cell carcinoma [19–22].
The cytologic evaluation of pericardial fluid in our study demonstrated pleomorphic cells with hyperchromatic, enlarged nuclei, which was concerning for malignancy. Although the patient had a history of cervical carcinoma, it was not in our top differentials, as cervical carcinoma metastasizing to the pericardium is extremely uncommon. We used a broad panel of IHC but found out that the tumor cells were only positive for p63 and p40, thereby pointing toward a diagnosis of meta-static cervical squamous cell carcinoma.
Conclusions
Although cervical cancer metastasizing to the pericardium is rare, it should be considered in patients with cervical cancer presenting with pericardial effusion, especially in patients with no other cause of pericardial effusion or a history of other malignancy. The prognosis of metastatic cervical carcinoma to the pericardium is generally poor, with a median survival time of only a few months. This case highlights the importance of considering the possibility of metastatic disease in the differential diagnosis of pericardial effusions and the value of IHC in the confirmatory diagnosis of metastatic tumors.
Figures
References:
1.. Sagristà-Sauleda J, Mercé J, Permanyer-Miralda G, Soler-Soler J, Clinical clues to the causes of large pericardial effusions: Am J Med, 2000; 109(2); 95-101
2.. Babu RS, Lanjewar A, Jadhav U, A case series of malignant pericardial effusion: J Family Med Prim Care, 2022; 11(10); 6581-85
3.. Sung H, Ferlay J, Siegel RL, Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries: Cancer J Clin, 2021; 71(3); 209-49
4.. Bhandari V, Kausar M, Naik A, Batra M, Unusual metastasis from carcinoma cervix: J Obstet Gynaecol India, 2016; 66(5); 358-62
5.. Sasidharan A, Hande V, Mahantshetty U, Shrivastava SK, Cardiac metastasis in cervical cancer: BJR Case Rep, 2016; 2(2); 20150300
6.. Rieke JW, Kapp DS, Successful management of malignant pericardial effusion in metastatic squamous cell carcinoma of the uterine cervix: Gynecol Oncol, 1988; 31(2); 338-51
7.. Nelson BE, Rose PG, Malignant pericardial effusion from squamous cell cancer of the cervix: J Surg Oncol, 1993; 52(3); 203-6
8.. Byun SW, Park ST, Ki EY, Intracardiac metastasis from known cervical cancer: A case report and literature review: World J Surg Oncol, 2013; 11; 107
9.. Hu K, Wang W, Liu X, Comparison of treatment outcomes between squamous cell carcinoma and adenocarcinoma of cervix after definitive radiotherapy or concurrent chemoradiotherapy: Radiat Oncol, 2018; 13(1); 249
10.. Cohen PA, Jhingran A, Oaknin A, Denny L, Cervical cancer: Lancet, 2019; 393(10167); 169-82
11.. Ghosh I, Mandal R, Kundu P, Biswas J, Association of genital infections other than human papillomavirus with pre-invasive and invasive cervical neoplasia: J Clin Diagn Res, 2016; 10(2); XE01-XE06
12.. Yu X, Wang Z, Zhang Z, Postoperation of cervical cancer with intestine metastasis: A case report and literature review: World J Surg Oncol, 2016; 14(1); 2
13.. Zhou S, Peng F, Patterns of metastases in cervical cancer: A population-based study: Int J Clin Exp Pathol, 2020; 13(7); 1615-23
14.. Rodríguez-Rosales YE, Salazar-Mejía CE, Soto-Martínez BA, Cardiac tamponade as an initial manifestation of cervical cancer: Case Rep Oncol Med, 2019; 2019; 7524797
15.. Burazor I, Aviel-Ronen S, Imazio M, Metastatic cardiac tumors: From clinical presentation through diagnosis to treatment: BMC Cancer, 2018; 18(1); 202
16.. Lee MJ, Kim DH, Kwan J, A case of malignant pericardial mesothelioma with constrictive pericarditis physiology misdiagnosed as pericardial metastatic cancer: Korean Circ J, 2011; 41(6); 338-41
17.. Anvari MS, Boroumand MA, Karimi A, Histopathologic and clinical characterization of atrial myxoma: A review of 19 cases: Lab Med, 2009; 40(10); 596-99
18.. Lagrotteria DD, Tsang B, Elavathil LJ, Tomlinson CW, A case of primary malignant pericardial mesothelioma: Can J Cardiol, 2005; 21(2); 185-87
19.. Gong W, Ye X, Shi K, Zhao Q, Primary malignant pericardial mesothelioma – a rare cause of superior vena cava thrombosis and constrictive pericarditis: J Thorac Dis, 2014; 6(12); E272-75
20.. Hernández-Bringas O, Ortiz-Hidalgo C, [Histopathological and immunohisto-chemical features of cardiac myxomas.]: Arch Cardiol Mex, 2013; 83(3); 199-208 [in Spanish]
21.. Wang JG, Li YJ, Liu H, Clinicopathologic analysis of cardiac myxomas: Seven years’ experience with 61 patients: J Thorac Dis, 2012; 4(3); 272-83
22.. Pereira TC, Share SM, Magalhães AV, Silverman JF, Can we tell the site of origin of metastatic squamous cell carcinoma? An immunohistochemical tissue microarray study of 194 cases: Appl Immunohistochem Mol Morphol, 2011; 19(1); 10-14
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133