07 July 2024: Articles 
Crusted Scabies in a Pediatric Liver Transplant Recipient on Immunosuppression
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Unexpected drug reaction, Rare disease, Clinical situation which can not be reproduced for ethical reasons
Laura Shih Hui GohDOI: 10.12659/AJCR.943128
Am J Case Rep 2024; 25:e943128






Abstract
BACKGROUND: Crusted scabies is a severe skin infection resulting from hyper-infestation with the obligate parasite Sarcoptes scabiei var. hominis. In contrast to classic scabies, crusted scabies may involve as many as hundreds to millions of mites. Importantly, this condition is associated with a mortality rate of 60% in 5 years, and is more likely to develop in immunosuppressed hosts, presumably due to an impaired T-cell response against the mite.
CASE REPORT: We present a case of crusted scabies in a 13-year-old girl during her early post-liver transplant period receiving immunosuppression successfully treated with topical 5% permethrin. She had pruritic erythematous papules, confirmed as scabies through skin scraping. The challenge of misdiagnosis during the initial presentation is noteworthy, given atypical manifestations and more common differentials. To our knowledge, only 2 cases of crusted scabies in pediatric solid-organ transplant recipients have been reported. Despite the absence of guidelines for pediatric solid-organ transplant recipients, urgent treatment is required due to the high associated mortality rates. In our case, early treatment proved successful without any secondary bacterial infections or clinical evidence of relapse during a 6-month follow-up.
CONCLUSIONS: We report a case of scabies in a pediatric liver transplant recipient that was successfully treated. It is crucial to consider the diagnosis of scabies given the associated morbidity and the risk of secondary bacterial infections among other more common differentials. Notably, the response to standard anti-scabies treatment may lead to resolution without relapse in pediatric solid-organ transplant recipients.
Keywords: Pediatrics, scabies, Liver Transplantation, Humans, Female, Adolescent, Permethrin, Immunocompromised Host, Immunosuppressive Agents, Insecticides, Immunosuppression Therapy
Introduction
Crusted (Norwegian) scabies is a severe type of skin infection caused by hyper-infestation with the obligate parasite
Case Report
We report a case of crusted scabies in a 13-year-old girl during her early post-liver transplant period, which was successfully treated with topical 5% permethrin. She had inflammatory bowel disease (IBD) with ulcerative pancolitis controlled with steroids, disease-modifying anti-rheumatic drugs, and biologics at age 2 years. She developed primary sclerosing cholangitis (PSC) at age 3 years. Despite treatment with tacrolimus and mycophenolic acid, this progressed to chronic liver disease complicated by portal hypertension, necessitating liver transplantation (LT) at 13 years of age. Histology of the explanted liver confirmed the diagnosis of PSC. She recovered well and was discharged 1 month after living-donor LT on immunosuppressant medications. Due to pancytopenia, both vedolizumab and mycophenolic acid were discontinued, with the regimen subsequently changed to tacrolimus 5 mg/day (trough levels 6–7.7 ng/ml) and prednisolone 5 mg/ day. Two weeks later, she developed widespread pruritic rashes.
The initial rashes appeared on both hands and improved with application of Fusidic acid cream. However, over the following month she developed intermittent pruritic rashes on her trunk, legs, arms, and left cheek. Physical examination revealed scaly, erythematous papules on both her upper and lower limbs, with scaling and plaques noted on the webs of her fingers and toes (Figure 1) and trunk (Figure 2). Although further examination of her family members revealed similar skin lesions, her social history did not indicate any contact with others having similar lesions, nor any exposure to household pets. Given the patient’s high level of immunosuppression, we considered her at increased risk for scabies infestation, leading to a clinical diagnosis of scabies based on the characteristic rash presentation. Subsequently, dermatology colleagues performed skin scrapings, which confirmed our initial diagnosis. The decision to forgo microscopy was based on strong clinical judgment that the diagnosis was clinically obvious.
Subsequently, the patient and her family were treated based on a clinical diagnosis of crusted scabies with 2 courses of 5% permethrin lotion for 3 days each at an interval of 3 weeks. They were advised to launder all linen at 60°C. The lesions started clearing after the second course of permethrin and completely resolved within 1 month. Household contacts were given prophylactic application of 5% permethrin lotion. There was no recurrence of scabies in the child or her parents over a 6-month follow-up.
Discussion
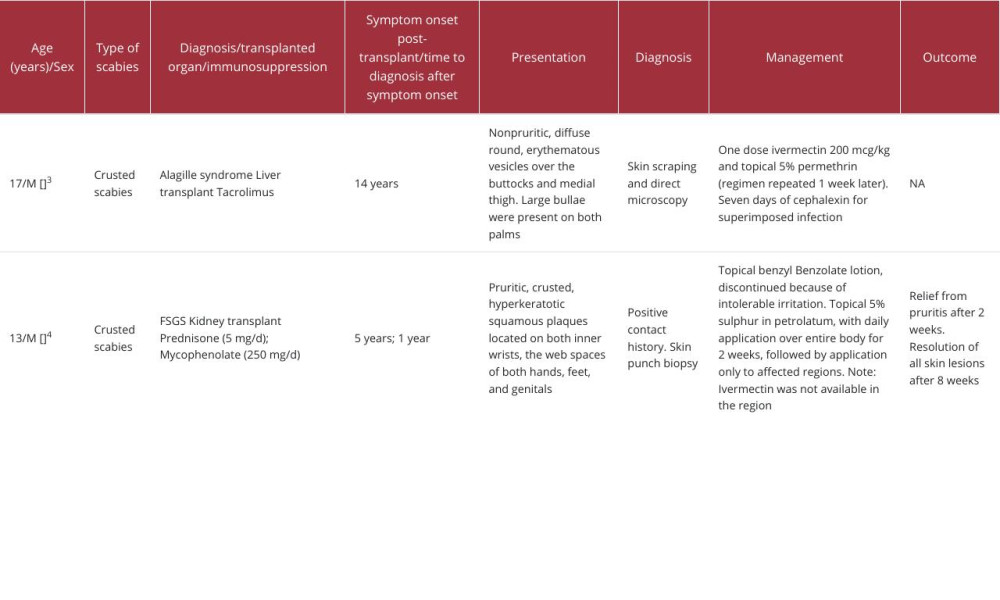
Crusted scabies is known to be associated with immunosuppressed states such as acquired immunodeficiency syndrome, leprosy, lymphoma, and transplant recipients on immunosuppression, because of disruption of acquired T-cell-mediated immunity against the scabies mite, which is central to limiting the infestation [2]. A search of PubMed and Google Scholar databases using the search terms “scabies” and “transplant” and “immunocompromised/suppressed” and “pediatric” identified 2 case reports of scabies after solid-organ transplant in the age group under 18 years (Table 1) [3,4].
Misdiagnosis at initial presentation was reported in a renal transplant recipient who was treated for psoriasis with topical antihistamines and topical steroids for 1 year, without improvement [4]. Reasons for misdiagnosis include atypical presentation with symptoms similar to common conditions such as dermatitis and eczema [4]. Although scabies is rarely reported in pediatric solid-organ transplant recipients, a lack of symptomatic relief of itching when present or poor response to treatment with antihistamines or topical steroids together with typical distribution of the skin rash should raise the suspicion. Secondary infection with
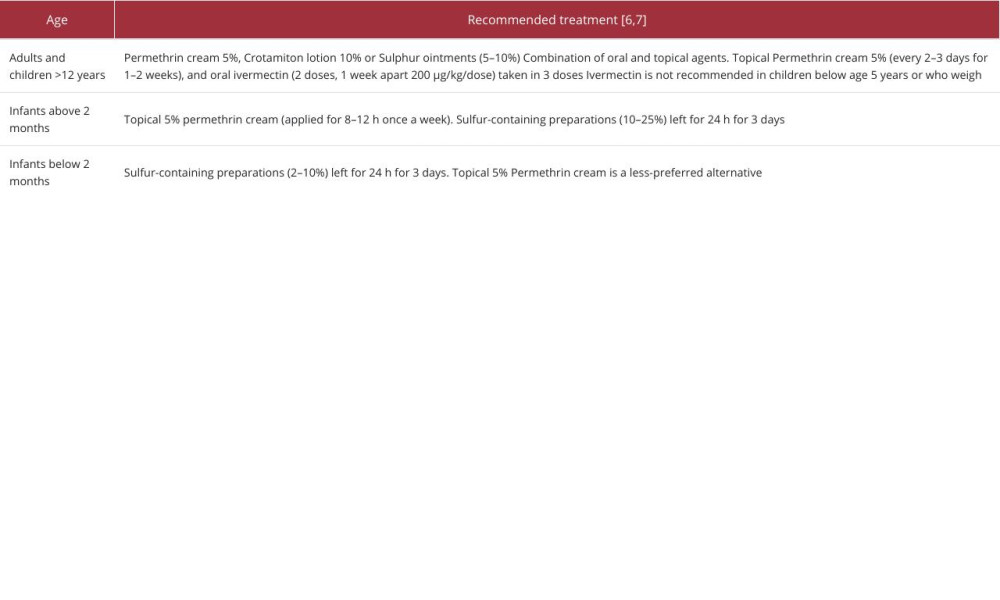
To our knowledge, this is only the second report of scabies in a pediatric LT recipient. Whether the paucity of literature of scabies in pediatric solid-organ transplants implies any real immunologic privilege or just a lack of reporting is uncertain. For example, as Roberts et al could not reach a specific immunologic diagnosis despite data showing immunological reactivity in their series of 78 patients, such as elevated IgE levels, eosinophilia, elevated interleukin-4 and a predominantly T-cell response in the skin infiltrates [1]. Crusted scabies has been previously reported following a prolonged period of immunosuppression (Table 1). However, the occurrence of crusted scabies in the early post-transplant period in our case may not be surprising given that she had been on long-term immunosuppression for her IBD and PSC prior to her LT. In general, guidelines for the management of scabies in children are limited as compared to adults (Table 2).
Nonetheless, with a reported mortality of 60% over 5 years in patients with crusted scabies, we preferred to implement urgent treatment given the lack of guidelines in pediatric solid-organ transplant recipients [5]. Such high mortality rates are often linked to sepsis or secondary infections, particularly in patients with comorbidities that lead to immunosuppression, such as post-transplant patients or those undergoing immunosuppressive therapy. Early diagnosis and treatment with 1 dose of ivermectin 200 mcg/kg and topical 5% permethrin were shown to be effective in achieving a quick and relapse-free response in a pediatric liver recipient with bullous scabies. In a pediatric renal transplant recipient in a region where ivermectin treatment is not available, the use of 5% sulphur petroleum was reported to be successful, without any relapse. In our case, treatment with 2 courses of topical 5% permethrin for 3 consecutive days 3 weeks apart was successful, without any clinical evidence of relapse over a 6-month follow-up [6,7]. Given concurrent issues of post-LT cholestasis due to a biliary anastomotic stricture, ivermectin was avoided [8]. In general, guidelines for the management of scabies in children remain limited compared to adults. Antibiotics were not administered, as there was no evidence of secondary bacterial infection. Given that scabies is transmitted by prolonged skin-to-skin contact, in addition to laundry and hygiene advice, we recommend prophylaxis for close contacts, including healthcare providers that have had prolonged direct skin contact with the patient. Work and school activities may be resumed the next day after prophylaxis treatment. Physical spaces occupied should be thoroughly cleaned.
Conclusions
In conclusion, we report another case of scabies in a pediatric liver transplant recipient. The diagnosis of scabies should be considered when presented with the typical rash, when there is a lack of response to treatment for dermatitis, and when
References:
1.. Roberts LJ, Huffam SE, Walton SF, Currie BJ, Crusted scabies: Clinical and immunological findings in seventy-eight patients and a review of the literature: J Infect, 2005; 50; 375-81
2.. Bimbi C, Brzezinski P, Sokolowska-Wojdylo M, Crusted (Norwegian) scabies as a strong marker of adult T-cell leukaemia/lymphoma in HTLV-1 infection: Clin Case Rep, 2019; 7; 474-76
3.. Salame N, Holland V, Non-pruritic bullous scabies in an immunosuppressed paediatric patient: Pediatr Dermatol, 2019; 36; 552-53
4.. Ede C, Gunduz O, Modi D, Crusted scabies in a pediatric renal transplant recipient on immunosuppressants: Transpl Infect Dis, 2020; 22; e13193
5.. Currie B, Huffam S, O’Brien D, Walton S, Ivermectin for scabies: Lancet, 1997; 350; 1551
6.. Thompson R, Westbury S, Slape D, Paediatrics: How to manage scabies: Drugs Context, 2023; 10; 2020-12 -3
7.. : Scabies – Resources for health professionals, 2019, CDC Available from: https://www.cdc.gov/parasites/scabies/health_professionals/meds.html
8.. Oscanoa TJ, Amado J, Romero-Ortuno R, Carvajal A, Hepatic disorders associated with the use of Ivermectin for SARS-CoV-2 infection in adults: A pharmacovigilance study in VigiBase: Gastroenterol Hepatol Bed Bench, 2022; 15; 426-29
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133