26 June 2024: Articles ")
Recurrent Hypoglycemia After Total Gastrectomy: A Case Report and Literature Analysis
Challenging differential diagnosis, Rare disease
Yue Zhang1CD, Haiyan Chen1AF, Zhe Wang2ABEF*DOI: 10.12659/AJCR.943144
Am J Case Rep 2024; 25:e943144






Abstract
BACKGROUND: Hypoglycemia is a common complication following total gastrectomy, primarily caused by dumping syndrome and severe malnutrition, with late dumping syndrome being particularly significant. However, for recurrent fasting hypoglycemia, the possibility of insulinoma should be considered. Hypoglycemia caused by insulinoma can lead to severe consequences, including seizures and even death. Thus, it is crucial to differentially diagnose hypoglycemia occurring after total gastrectomy.
CASE REPORT: In this report, we present the case of a 36-year-old Chinese woman who underwent total gastrectomy for gastric cancer and subsequently received chemotherapy. Four months after surgery, she began experiencing recurrent seizures, and multiple tests confirmed hypoglycemia. A series of laboratory and imaging examinations ultimately led to a diagnosis of insulinoma. After surgical resection of the tumor, the patient’s hypoglycemic symptoms resolved, and pathology results confirmed an insulinoma.
CONCLUSIONS: This case report highlights the rapid weight loss and severe hypoglycemia observed in a patient only 4 months after total gastrectomy for gastric cancer. Although dumping syndrome was initially suspected based on the clinical course, the final diagnosis turned out to be insulinoma. The case underscores the importance of comprehensive evaluation and appropriate diagnostic investigations for patients experiencing hypoglycemia after total gastrectomy. Furthermore, the case suggests that the increased levels of enteroglucagon following changes in the gastrointestinal tract resulting from total gastrectomy may promote the development of insulinomas. This case report also contributes to the existing literature regarding atypical presentations of insulinomas and their association with gastric resection.
Keywords: Gastrectomy, Hypoglycemia, Insulinoma, Humans, Female, adult, Stomach Neoplasms, Recurrence, Pancreatic Neoplasms, Postoperative Complications, Dumping Syndrome
Introduction
Hypoglycemia following total gastrectomy can stem from various factors, such as dumping syndrome, especially late dumping syndrome, malnutrition, and impaired liver function. In many instances, these causes can be addressed by improving dietary habits and providing symptomatic treatment. However, when recurrent hypoglycemic symptoms persist, particularly in the fasting state, it is important to consider the possibility of insulinoma. In this case report, we describe a patient who underwent total gastrectomy for gastric indolent cell carcinoma. Four months after the surgery, the patient began experiencing seizures without apparent triggers, eventually leading to a diagnosis of insulinoma after continuous glucose monitoring and pancreatic magnetic resonance imaging (MRI). Subsequent surgical resection resulted in an improvement of the hypoglycemic symptoms and the specimen confirmed the diagnosis of insulinoma. This case underscores the importance of considering insulinoma as a potential cause of hypoglycemia following total gastrectomy, particularly when recurrent episodes occur.
Case Report
The patient was a 36-year-old woman who underwent laparoscopic-assisted radical total gastrectomy (Billroth II + Braun anastomosis) 4 months ago. The pathological diagnosis revealed poorly differentiated adenocarcinoma, with a portion being signet ring cell carcinoma (Figure 1). Following surgery, the patient underwent 4 cycles of chemotherapy. The chemotherapy regimen for the cancer included intravenous infusion of oxaliplatin (200 mg on the first day) and oral administration of tegafur/gimeracil/oteracil (S-1) (60 mg, twice daily). Each treatment cycle was administered every 3 weeks. There were no instances of hypoglycemia observed before, during, or immediately after the surgery. However, approximately 4 months later, the patient was admitted to the Neurology Department with nocturnal fever and experienced intermittent tonic seizures of the right limb accompanied by slurred speech. During the patient’s hospitalization, her fasting blood glucose level was 1.47 mmol/L. These seizures were initially attributed to malnutrition following gastric surgery or hypoglycemia resulting from late dumping syndrome. After discharge, she continued to display symptoms such as irritability, slurred speech, and recurrent seizures. She did not monitor her blood glucose level at home. When she experienced seizures, fingertip blood glucose was measured at an external emergency department, yielding a result of 1.4 mmol/L. Due to the unclear diagnosis of the underlying cause of hypoglycemia, she was transferred to the Endocrinology Department at our hospital for further evaluation and management.
She had no prior history of chronic illnesses such as hypertension or diabetes mellitus, and denied any history of smoking or alcohol consumption. Furthermore, there were no significant abnormalities reported in the patient’s family medical history.
Physical examination revealed her height was 160 cm, weight was 41.5 kg (BMI=16.2 kg/m2). The patient appeared emaciated, with blood pressure 100/63 mmHg (1 mmHg=0.133 kPa), and no cardiopulmonary abnormalities were noted. On examination, the abdomen was soft, with a visible scar measuring approximately 10 cm in length located in the middle of the abdomen. Reduced muscle strength was observed in the extremities, but no other abnormalities were detected.
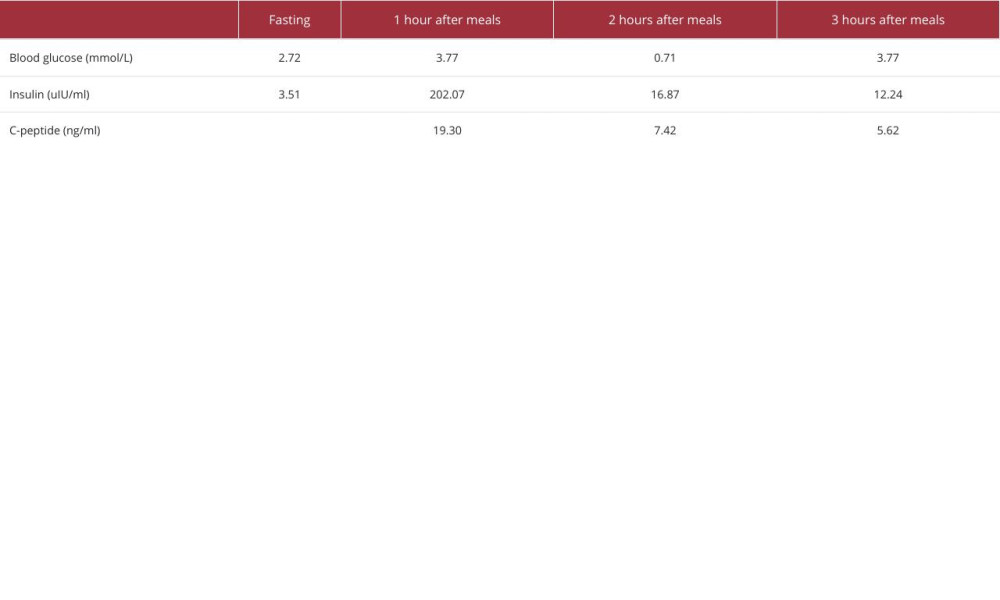
Laboratory examinations were performed. The insulin release test (Table 1) consistently showed low blood glucose levels, prompting simultaneous measurement of insulin and C-peptide levels when blood glucose was <3.0 mmol/L. The insulin release index (INS/GLU) was >0.4. Fasting insulin and C-peptide levels were elevated, while glycated hemoglobin was 4.7% (normal range: <5.7%). In terms of liver function, ALT was 125 U/L (normal range: 7–40 U/L), AST was 191 U/L (normal range: 13–45 U/L), and ALB was 30.3 g/L (normal range: 40–55 g/L). Thyroid function was within the normal range, with TSH 2.0759 μIU/mL (normal range: 0.35–4.94 μIU/mL), FT4 was 11.45 pmol/L (normal range: 9.01–19.05 pmol/L), and FT3 was 4.94 pmol/L (normal range: 2.43–6.01 pmol/L). Cortisol level was 301 nmol/L (normal range: 133–537 nmol/L). IGF-1 was 107 ng/ml (normal range: 60–350 ng/ml), and the diabetes antibody series was negative.
Imaging examinations were performed. Computed tomography (CT) demonstrated post-total gastrectomy alterations, including various changes associated with removal of the stomach. Additionally, several small lymph nodes were observed in the vicinity of the stomach.
Based on these examinations, there was a high suspicion of insulinoma or islet cell hyperplasia. Subsequently, the patient underwent dynamic MRI of the pancreas, which supported the diagnosis of insulinoma (Figure 2). Therefore, she was referred to the Hepatobiliary Surgery Department for insulinoma surgery (Figure 3). The postoperative pathology results (Figure 4) confirmed the presence of a neuroendocrine tumor, specifically a pancreatic body tail neuroendocrine tumor, classified as NET G1. On the first day after surgery, the venous blood glucose level was 5.3 mmol/L, indicating normal glucose levels. The patient was followed up postoperatively and did not experience any hypoglycemia or further seizure symptoms.
The patient had a documented history of gastric surgery and underwent 4 cycles of postoperative chemotherapy before onset of the disease. At that time, there were no hypoglycemic symptoms or supporting test evidence. The patient’s preoperative anthropometric measurements indicated a height of 160 cm and a weight of 61.5 kg (BMI=24.0 kg/m2). Subsequently, within a span of 4 months, she had a substantial weight reduction from 61.5 kg to 41.5 kg (BMI=16.2 kg/m2), signifying an alarming decline in nutritional status. This was further confirmed by the subjective global assessment (SGA) score, which took into consideration the significant weight loss, inadequate dietary intake, previous history of gastric cancer, and extreme frailty during hospitalization. The patient had no history of using hypoglycemic medication, and after comprehensive blood biochemistry, hormone, and islet cell antibody tests, as well as chest and abdominal CT scans, the causes of hypoglycemia were first considered to be late dumping syndrome and malnutrition. Nevertheless, during 2 hospitalizations in the Neurology Department, she had frequent and worsening episodes of unexplained hypoglycemia that could not be explained by late dumping syndrome and malnutrition. We utilized continuous glucose monitoring (CGM) to monitor blood glucose levels and observed that fasting blood glucose exhibited fluctuations ranging from 1.8 to 6.4 mmol/L, while postprandial blood glucose ranged between 2.8 and 5 mmol/L, occasionally peaking at 10 mmol/L. The administration of continuous glucose infusion effectively maintained her fasting blood glucose within the range of 4–7 mmol/L. Oral glucose tolerance testing (OGTT) in Endocrinology Department revealed persistently low blood glucose levels and abnormally elevated insulin secretion, with an insulin release index much greater than 0.4. Maintaining the patient’s blood glucose within the range of 3–4.5 mmol/L required continuous intravenous administration of 5% glucose, consistent with Whipple’s triad, and an enhanced thin-layer pancreatic MRI scan revealed an occupancy in the mid-pancreatic body, leading to the diagnosis of insulinoma. She ultimately underwent surgery for insulinoma. The abdominal cavity exhibited extensive adhesion surrounding the pancreas, posing challenges in separating the small intestine, colon, spleen, and pancreas. Consequently, the definitive surgical procedure encompassed distal pancreatectomy, splenectomy, and intestinal adhesiolysis. Following surgical resection, the patient experienced relief from hypoglycemic symptoms.
Discussion
Hypoglycemia is a common complication following esophageal, gastric, and bariatric surgery. These procedures disrupt the normal anatomy and innervation of the stomach, leading to rapid transit of undigested food into the small intestine. This phenomenon is also known as dumping syndrome. Dumping syndrome can manifest as early or late symptoms. Late dumping syndrome, occurring mainly 1–3 h after a meal, is characterized by hypoglycemic symptoms such as hunger, palpitations, and sweating [1]. This is thought to be caused by high-sugar foods in the intestinal lumen promoting the secretion of GLP-1 in the small intestine, subsequently stimulating insulin secretion [2].
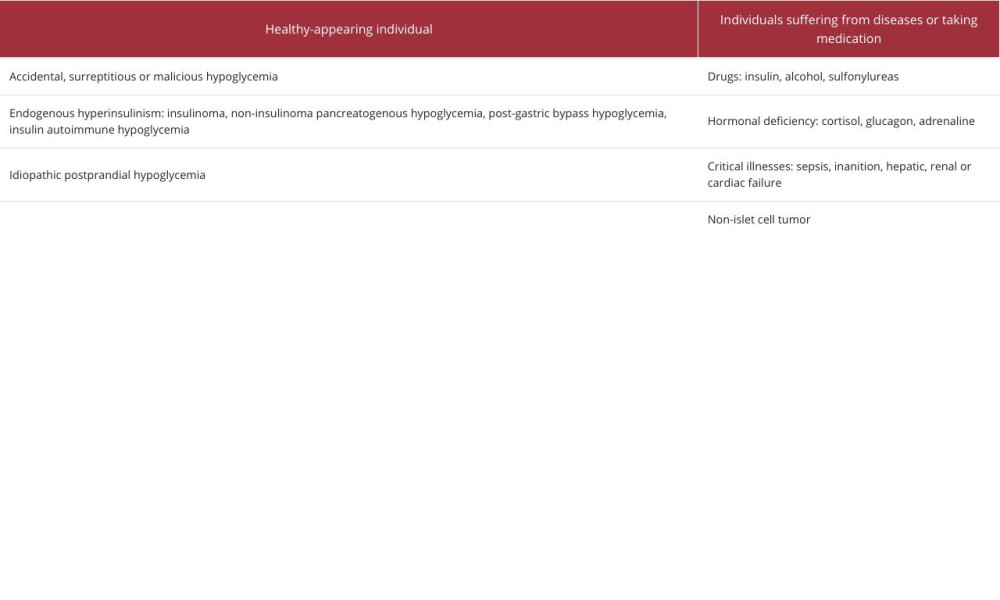
The prevalence of dumping syndrome varies depending on the surgical procedure. Vagotomy with pyloroplasty carries a 20% risk, while Roux-en-Y gastric bypass (RYGB) or sleeve gastrectomy have a 40% risk, and esophagectomy has a 50% risk [1]. While post-bariatric surgery hypoglycemia is a common complication, several studies indicate that many of the hypoglycemic and even severe events are asymptomatic. In a survey examining the prevalence of post-bariatric surgery hypoglycemia (PBH), the authors found a prevalence of 75% for PBH, with many patients being asymptomatic [3,4]. Hypoglycemia episodes following gastric bypass surgery can present in various ways, making diagnosis challenging. Symptoms may include palpitations, sweating, hunger, and neurological manifestations such as seizures and impaired consciousness, which can be mistaken for epilepsy if not properly evaluated [5]. Malnutrition following total gastrectomy can also contribute to hypoglycemia. Therefore, it is essential to assess the timing of symptom onset and hypoglycemia, considering blood glucose concentrations at the time of symptoms or conducting ambulatory glucose monitoring. The diagnosis of hypoglycemia relies on Whipple’s triad – symptoms of hypoglycemia, low plasma glucose level during episodes, and symptom relief upon plasma glucose level normalization through glucose administration [3]. Once hypoglycemia is confirmed, further diagnostic investigations are necessary to determine the underlying cause (Table 2) [6].
Insulinoma is a rare functional endocrine tumor of the pancreas, with an incidence of 1–4 per 1 000 000. It represents approximately 1–2% of all pancreatic tumors and is characterized by excessive secretion of insulin, leading to development of hypoglycemia. Most insulinomas (90%) are benign, isolated (90%), and smaller than 2 cm (90%) in size. Furthermore, more than 90% of these tumors occur within the pancreas [7]. In patients presenting with spontaneous hypoglycemia, measuring plasma glucose, insulin, C-peptide, and insulinogen levels during the hypoglycemic episodes can help assess for the presence of abnormally elevated insulin. Asymptomatic patients often undergo a 72-h fasting test, which can induce the onset of hypoglycemia and detect up to 99% of insulinomas [8].
Imaging plays a crucial role in localizing and diagnosing insulinomas. When insulinoma is strongly suspected, pancreatic MRI is considered the imaging test of choice for this condition and can provide confirmation of the diagnosis [9]. Insulinomas generally develop slowly. A case was reported of a 61-year-old man who underwent total gastrectomy and Roux-en-Y reconstruction for cancer and developed severe postprandial hypoglycemia with endogenous hyperinsulinemia 3 years later. Pathological analysis after distal pancreatectomy revealed that the pancreatic neuroendocrine microadenoma contained insulin-producing cells, and this case confirms that insulinoma develops very slowly [10]. In another case report, a woman experienced recurrent hypoglycemia for 2 months following total gastrectomy for a gastrointestinal stromal tumor that had been performed 1 year earlier. She was initially suspected to have late dumping syndrome, and further examination confirmed the presence of insulinoma [11]. Patients are diagnosed an average of 1.5 years after symptom onset, but some patients have symptoms for decades before being diagnosed [12]. It has never been reported that patients after total gastrectomy rapidly progress from normal glycemic status to severe and persistent hypoglycemia in as little as 4 months. Animal experiments proved that after Roux-en-Y gastric bypass treatment, the levels of related hormones and Ca2+ levels changed, mainly manifested as increased levels of HOMA-β, GLP-1, intracellular free Ca2+ concentration, and decreased levels of ghrelin, which promoted the differentiation of primitive cells to islet cells and improved the function of β-cells, and ultimately led to the enhancement of insulin secretion [13]. The insulinoma that appeared after radical gastric cancer surgery in women may also be related to the altered gastrointestinal hormonal changes and stimulation of islet cell proliferation after surgery, and these changes accelerated the process of islet cell tumor. Meanwhile, severe malnutrition and liver damage affecting liver glycogen reserve accelerated the occurrence and progression of hypoglycemia. The patient had undergone a comprehensive examination including abdominal CT before gastrectomy. No tumor was found in the pancreas, and no symptoms of hypoglycemia appeared before or 4 months after surgery. However, the possibility of extremely small islet cell tumor could not be ruled out, which was difficult to detect on CT and showed rapid proliferation after surgery.
Upon analysis of the reasons for the previous misdiagnosis, several factors were identified:The patient exhibited normal blood glucose levels 4 months prior, as well as the absence of hypoglycemic symptoms after total gastric resection surgery and chemotherapy. Therefore, the hypoglycemia that subsequently appeared would typically be attributed to the surgical procedure, such as dumping syndrome [14].Significant weight loss of 20 kg after surgery indicated severe malnutrition, which is contrary to the weight gain often observed in patients with islet cell tumors due to excessive food intake [15].The rapid progression of hypoglycemic symptoms was inconsistent with the typical slow progression of the disease course of insulinoma [12,16].The primary symptom was recurrent seizures, leading to the initial diagnosis and treatment of a neurological disorder. These factors contributed to the initial misdiagnosis and delayed identification of the underlying cause of hypoglycemia [17].
While there are various factors that can cause hypoglycemia after gastric surgery, including malnutrition, it is crucial to consider the possibility of rare concurrent insulinoma in patients with persistent hypoglycemia, especially those experiencing recurrent hypoglycemia or seizures. The rapid progression of insulinoma after total gastrectomy was also unexpected. Prompt recognition and diagnosis of insulinoma can help prevent treatment delays and potential complications.
Conclusions
In summary, we report a case of a woman who experienced recurrent hypoglycemia following gastric cancer surgery and was ultimately diagnosed with insulinoma. This case underscores the significance of considering insulinoma as a potential cause of hypoglycemia following total gastrectomy, particularly when recurrent episodes occur. The case also contributes to the existing literature regarding atypical manifestations of insulinomas and their association with gastric resection surgery.
Figures
References:
1.. Scarpellini E, Arts J, Karamanolis G, International consensus on the diagnosis and management of dumping syndrome: Nat Rev Endocrinol, 2020; 16(8); 448-66
2.. van Beek AP, Emous M, Laville M, Tack J, Dumping syndrome after esophageal, gastric or bariatric surgery: Pathophysiology, diagnosis, and management: Obes Rev, 2017; 18(1); 68-85
3.. Michaels AD, Hunter Mehaffey J, Brenton French W, Hypoglycemia following bariatric surgery: Our 31-year experience: Obes Surg, 2017; 27(12); 3118-23
4.. Lazar LO, Sapojnikov S, Pines G, Symptomatic and asymptomatic hypoglycemia post three different bariatric procedures: A common and severe complication: Endocr Pract, 2019 [Online ahead of print]
5.. Salehi M, Vella A, McLaughlin T, Patti ME, Hypoglycemia after gastric bypass surgery: Current concepts and controversies: J Clin Endocrinol Metab, 2018; 103(8); 2815-26
6.. Cryer PE, Axelrod L, Grossman AB, Evaluation and management of adult hypoglycemic disorders: An endocrine society clinical practice guideline: J Clin Endocrinol Metab, 2009; 94(3); 709-28
7.. Okabayashi T, Shima Y, Sumiyoshi T, Diagnosis and management of insulinoma: World J Gastroenterol, 2013; 19(6); 829-37
8.. Mulla CM, Storino A, Yee EU, Insulinoma after bariatric surgery: Diagnostic dilemma and therapeutic approaches: Obes Surg, 2016; 26(4); 874-81
9.. Lobaton-Ginsberg M, Sotelo-González P, Ramirez-Renteria C, Insulinoma after sleeve gastrectomy: A case report: World J Clin Cases, 2022; 10(18); 6227-33
10.. Hayashida R, Tsuchiya K, Sekine T, A clinical case of insulinoma presenting with postprandial hypoglycemia in a patient with a history of gastric bypass surgery: Intern Med, 2022; 61(8); 1189-95
11.. Bilen A, Mercantepe F, Bilen H, Capoglu I, A case of insulinoma confused with dumping syndrome after total gastrectomy: Journal of Surgery and Medicine, 2022; 6(5); 594-96
12.. Giannis D, Moris D, Karachaliou GS, Insulinomas: from diagnosis to treatment: A review of the literature. J BUON, 2020; 25(3); 1302-14
13.. Yu HW, Zheng XY, Zhang ZM, Mechanism of Roux-en-Y gastric bypass treatment for type 2 diabetes in rats: J Gastrointest Surg, 2013; 17(6); 1073-83
14.. Papamargaritis D, Koukoulis G, Sioka E, Dumping symptoms and incidence of hypoglycaemia after provocation test at 6 and 12 months after laparoscopic sleeve gastrectomy: Obes Surg, 2012; 22(10); 1600-6
15.. Park HK, Ahima RS, Endocrine disorders associated with obesity: Best Pract Res Clin Obstet Gynaecol, 2023; 90; 102934
16.. Service FJ, McMahon MM, O’Brien PC, Ballard DJ, Functioning insulinoma – incidence, recurrence, and long-term survival of patients: A 60-year study: Mayo Clin Proc, 1991; 66(7); 711-19
17.. Yu Z, Wang Y, Sun Y, Case report: Insulinoma presenting as excessive daytime somnolence: Front Endocrinol (Lausanne), 2021; 12; 712392
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133