28 June 2024: Articles 
The Rising Concern of Ethanol Intoxication from Easy Access to Hand Sanitizers: A Case Report
Unusual clinical course, Challenging differential diagnosis, Diagnostic / therapeutic accidents, Unusual setting of medical care, Adverse events of drug therapy, Clinical situation which can not be reproduced for ethical reasons
Mahmoud El-Hussein1ACDE*, Cima Hamieh2EF, Patrick Nasrallah3AE, Eric Revue1AEDOI: 10.12659/AJCR.943318
Am J Case Rep 2024; 25:e943318






Abstract
BACKGROUND: Ethanol intoxication is very common, and several forms of alcohol intoxication can lead to emergency department visits. Excessive alcohol users, when in withdrawal, might seek replacement alcoholic beverages; one of the common sources of ethanol is hand sanitizer, which contains 45-95% alcohol. It becomes even more challenging to deal with alcohol use disorder patients when they seek these replacement products inside hospital premises, and medical clinics and hospitals have increased their use of ethanol-based hand sanitizer since the start of the COVID-19 pandemic.
CASE REPORT: We report the case of a 26-year-old man with alcohol dependence presenting with a fictitious illness leading to hospital admission and consumption of ethanol-based hand sanitizer in the emergency department (ED). The patient initially presented reporting severe abdominal pain that persisted despite medications. The initial laboratory tests and imaging were non-significant. The patient was later caught stealing hand sanitizer bottles, consuming them within 4-6 h. The COVID-19 pandemic has increased alcohol intoxication, especially in EDs. Hand sanitizers, including ethanol, are toxic and hazardous when misused, mostly by adolescents and young adults. Treatments include glucose determination, dextrose infusion, and thiamine perfusion. Strategies to reduce ethanol intoxication include eliminating hand sanitizers, using wall-fixed sanitizers, and using sanitizer wipes.
CONCLUSIONS: Patients with alcohol use disorder are known to develop alcohol-seeking behaviors. This report has highlighted that healthcare professionals should be aware that the increased availability of ethanol-based hand sanitizers, some of which contain toxic antiviral chemical agents, may be targeted by individuals with alcohol dependency.
Keywords: Alcoholism, Hand Disinfection, Factitious Disorders, Emergency Medical Services, Humans, Male, adult, Hand Sanitizers, Alcoholic Intoxication, COVID-19, Ethanol, Emergency Service, Hospital, SARS-CoV-2
Introduction
The Diagnostic and Statistical Manual of Mental Disorders (DSM) V delineates 4 stages of alcoholism: early stage involves occasional binge drinking, while end-stage alcoholism consists of severe health problems, disability, and dependance [1].
Alcohol use disorder as defined by Nehring et al is a medical condition that can be diagnosed when an individual’s drinking causes distress and harm, and the pleasurable effects of drinking may in turn elicit alcohol-seeking behaviors [2,3].
Brain region such as the hypothalamus and nucleus accumbens and hormones such as betta endorphins and other stress hormones can play a role in alcohol-seeking behaviors. Research in animal models concluded that previous exposure to alcohol and stress can lead to alcohol-seeking behavior by activating specific areas in the brain [4]. Therefore, when alcoholic beverages are not accessible, alcohol users in the late and end stages of addiction shift to any available alternative, such as paint, perfumes, hairsprays, gasoline, sanitizers, and cooking extracts, as these can contain large amounts of alcohol [5].
Hand sanitizers are mostly ethanol, but also can contain isopropanol, methanol, and acetone [5].
World health Organization and Centers for Disease control guidelines for hand hygiene require alcohol-based hand sanitizers to be available in all healthcare facilities [5,6]. Furthermore, the use of hand liquid antiseptics has increased drastically after the emergence of the corona virus pandemic, and hand cleaners are used in medical settings and in homes [7]. Nearly every house, shop, and restaurant in the world has had these products freely available for the public [7]. This widespread availability has led to a drastic increase in intentional ingestion of ethanol-based hand sanitizers [7]. Symptoms of ethanol ingestion intoxication include hypoglycemia, dis-equilibrium, seizures, confusion, coma, respiratory arrest, and death [8]. Several published articles have addressed the issue of hand sanitizers being widely available with easy access in EDs [5,6]. Patients therefore can easily ingest, steal, and hide these hand sanitizers without being noticed by medical staff. Emergency physicians and staff should pay very close attention to patients with addiction to alcohol, especially in departments where many disposable ethanol-based hand sanitizer bottles are available.
Yip et al wrote an article published in the weekly report of the Center for Disease Control and Prevention on August 14th, 2020, presenting cases of methanol poisoning due to ingestion of hand sanitizers by patients, which caused fatalities or disability such as vision loss [9].
The aim of the present report is to raise awareness of acute ethanol intoxications in EDs and to present clinical aspects of these intoxicated patients. Ethanol intoxication is very common, can be life-threatening, and can lead to many complications.
This report is of a 26-year-old man with alcohol dependence presenting with a feigned illness leading to hospital admission and consumption of ethanol-based hand sanitizer.
Case Report
A 26-year-old male patient presented to the ED reporting severe abdominal pain. He was hemodynamically stable, afebrile, with normal blood pressure and saturation, acted irritated, and was sometimes verbally aggressive.
His physical exam was insignificant except for poor general hygiene, tachycardia, and diffuse abdominal tenderness; the abdomen was soft.
Intravenous (IV) medications were prescribed, including Perfalgan, Pantoprazole, and Phloroglucinol for symptomatic relieve, but no improvement was observed, as the patient remained agitated.
IV morphine was titrated to calm the patient, who still complained of severe, non-resolving abdominal pain. Several abdominal reexaminations were done by the residents and the attending physician, with no change in the abdominal exam, which remained soft throughout the patient’s stay. The surgery team was consulted for this reported severe abdominal pain, and they agreed to wait for the laboratory results and to perform an abdominal computed tomography (CT) scan afterwards to rule out perforation, volvulus, or, less probably, mesenteric ischemia.
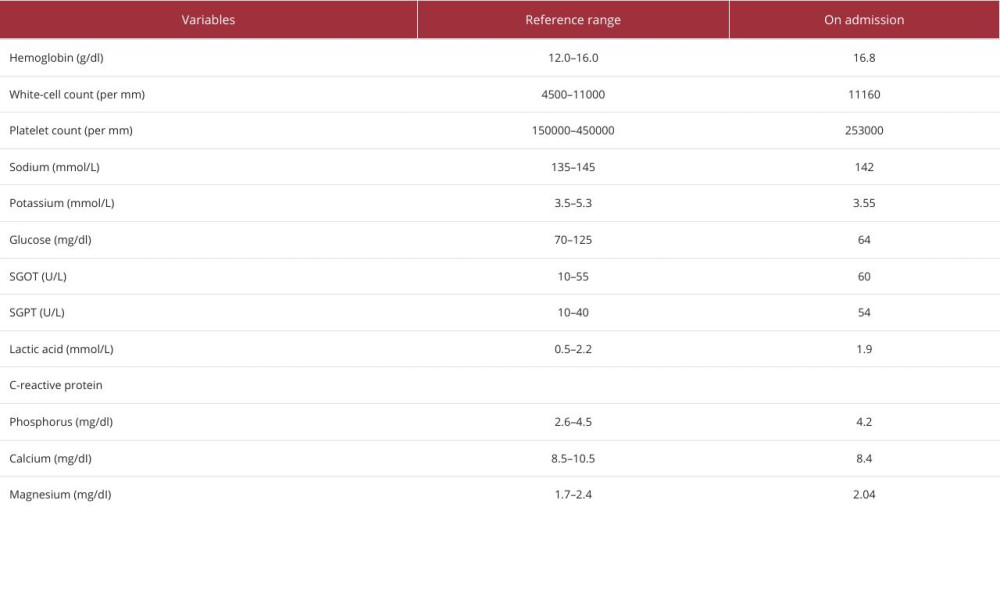
An electrocardiogram showed sinus tachycardia with no ischemic signs. A rapid urinary bundle was ordered to rule out kidney stones, and this also was negative. The laboratory findings showed normal complete blood count without an increase of leukocytes, normal electrolytes, normal creatinine levels, negative CRP, normal lipase, and slightly elevated liver enzymes (Table 1).
The patient was immediately sent to Radiology, where an abdominal computed tomography (CT) scan was normal, with only signs of fatty liver.
After all this activity to help the patient, another patient sharing same the room approached the nurse to inform her that the patient in question was stealing hand sanitizer bottles, hiding them in his bag, and drinking them during his stay.
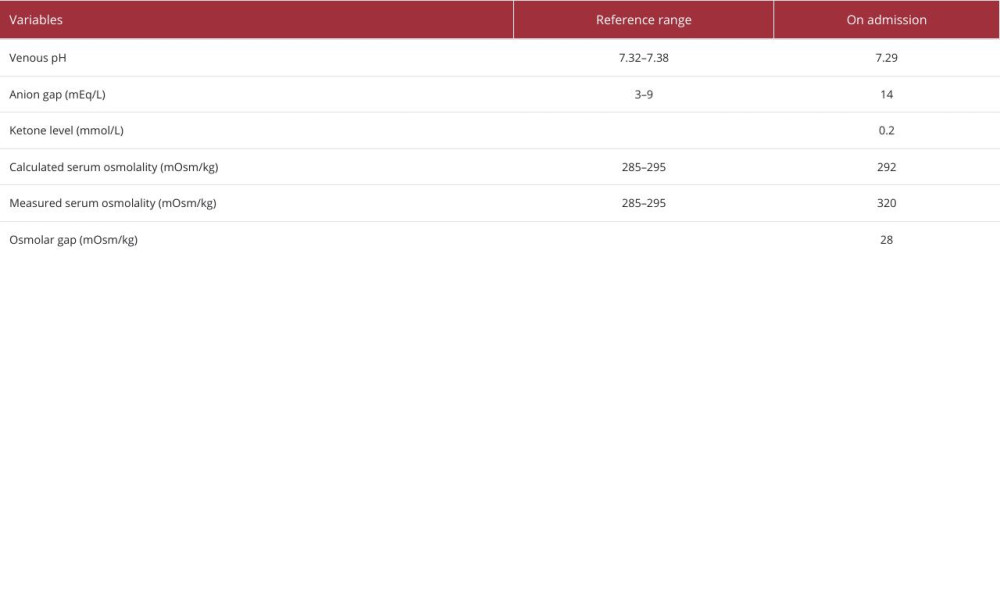
Blood testing revealed a 0.2% ethanol serum level, a urine toxicology screen that the patient had approved was positive for tetrahydrocannabinol (THC), and further laboratory testing was done (Table 2). The patient was informed of these new results by the emergency physician and addictologists. He confessed to faking illness and drinking from stolen hand sanitizer bottles, as he was having withdrawal symptoms. Seven 475-ml bottles of hand sanitizer stolen from our ED were found in his bag, of which about a bottle and a half had been consumed during a 4–6 h period. The bottles contained 1.45% glycerol, 0.13% hydrogen peroxide, and 80% ethanol.
The patient received hydration and thiamine infusion along with vitamins B3 and B6. Benzodiazepine was added to help calm him, as he was still agitated. He was hospitalized in the medical ward for 24-h clinical observation and was later discharged home with scheduled addictology follow-up.
Discussion
Vigilance is very important in the ED when taking care of patients with signs of alcohol poisoning or withdrawal, and can be lifesaving, but it can be very challenging when dealing with a patient presenting fictitious illness and alcohol-seeking behavior. In this case the patient presented with feigned abdominal pain to gain access to alcohol-containing hand sanitizer.
Hand sanitizers are in no doubt essential tools to fight infection, protecting both the user and others. During the COVID-19 pandemic, the World Health Organization recommended that hand sanitizers be made up from ethanol, isopropyl alcohols, and/or hydrogen peroxides in several combinations, all of which are toxic and hazardous for the environment and humans when misused [10]. Similar cases reported in the literature proved the increased occurrence of this behavior and the drastic outcomes for patients [9]. Therefore, when assessing patients who have swallowed an alcohol-based hand sanitizer in the past or who exhibit symptoms consistent with alcohol poisoning, clinicians should be highly suspicious of the condition and, if necessary, seek medical management advice from the local poison center.
It has been reported that ethanol intoxication has peaked since the COVID-19 pandemic due to the wide availability of hand sanitizers [5]. Although alcohol is the most common form of abused ethanol substance in Western culture, other forms of ethanol intoxication are also common [7]. Demographically, adolescents and young adults are the most common intoxicated patients seen in EDs [7]. It was reported that 3.3 million deaths involved acute alcohol ingestion, which makes it the fourth leading preventable cause of death in the United States [7].
The intoxication can be acute or chronic; rapid ingestion of a large amount can be clinically harmful [6]. While the acute ingestion itself can be life-threatening, complications related to acute ingestion are common, such as traumatic injury (especially traumatic brain injuries), domestic violence, homicide, and violence [7–5].
The present patient had an extensive workup done prior to the diagnosis, including other differential diagnoses like sepsis, non-alcoholic toxicology ingestion, hypo- or hyperthyroidism, glucose disturbances, intracranial bleed, and hepatic encephalopathy, leaving alcohol intoxication last on the list [7].
The diagnosis was confirmed by a blood alcohol level test. The clinical symptoms are related to the blood alcohol concentration (BAC). The severity of the symptoms seems to increase gradually with the increase of BAC [6]. At less than BAC 0.05% (<50 mg/dL), symptoms can include decreased fine motor function and increased talkativeness. At BAC 0.050–1% (50–100 mg/dL), symptoms can include impaired judgment and coordination, which was the level observed in this case. At BAC 1–2% (100–200 mg/dL), symptoms can include gait instability, mood and behavior changes, and slurred speech. BAC over 2% can be life-threatening, with vomiting, hypothermia, and dysarthria. BAC of more than 4% (>400 mg/dL) can cause respiratory depression followed by coma and death [7].
Just like the physicians did for this patient, when caring for any patient with ethanol intoxication, a full blood test including metabolic panel, liver panel, and a venous blood gas should be obtained to detect metabolic abnormalities. Ethanol intoxication can cause lactic acidosis, hypokalemia, hypomagnesemia, hypocalcemia, hypophosphatemia, and hypoglycemia [7–11].
Measurement of anion gap and serum osmolar gap can be useful, as patients with suspected ingestion of toxic alcohol have a high anion gap with a high osmolar gap metabolic acidosis [5]. Co-ingestion with other alcohols (eg, ethylene glycol and methanol) should be suspected with a very high metabolic acidosis and an increased anion gap; for example, in the present patient, the anion gap was 14, indicating alcohol intoxication [7].
Cardiovascular effects such as tachycardia, volume depletion, peripheral vasodilation, hypotension, and hypothermia should also be evaluated [11], so an electrocardiogram should be obtained for detection of possible new-onset atrial fibrillation, which usually resolves once the intoxication is cleared [7].
The data in the literature agree with our case, showing how the symptoms of alcohol intoxication can be misleading and lead to misdiagnosis, and patients with alcohol abuse may mislead ED staff, wasting resources, time, and effort, to obtain alcohol-containing substances.
Treatment is usually supportive, including bedside glucose determination followed by dextrose infusion in case of hypoglycemia and perfusion with thiamine to prevent or treat Wernicke’s encephalopathy [5]. Agitated, uncooperative, and/or violent patients should be carefully managed as they can harm themselves and others. Decontamination using activated charcoal is not indicated unless there is co-ingestion of other drugs, as activated charcoal does not absorb ethanol [12].
De-escalation techniques and medications like benzodiazepine and first-generation anti-psychotics are commonly used [5]. The use of mechanical restraints should be avoided unless the patient is trying to escape or for prevention of physical trauma given the ethical concerns about their use [11]. A psychiatric evaluation is necessary once the patient is lucid and able to speak coherently, as suicidal thoughts can be stated during the intoxication period [7].
Metadoxine, pyridoxal L2 pyrrolidone – 5-carboxylate, although still not FDA-approved, has shown promising results in decreasing the BAC and improving the symptoms of acutely intoxicated individuals [8–11]. It accelerates the ethanol degradation rate, which reduces the metabolite in the ethanol elimination process [11].
Mildly intoxicated patients can be discharged when they are no longer intoxicated and when it appears they will not cause harm to themselves or others. They should ideally be discharged into the care of a sober, competent individual [5].
It is a major challenge to ensure the safety of alcoholic patients inside the ED while maintaining a good hand hygiene policy. With the increased production and availability of hand sanitizer, there has been an increase in their abuse for intoxication cases, and physicians and staff should always be alert to prevent abuse. Eliminating hand sanitizers from the patient’s room, the use of wall-fixed hand sanitizers with period maintenance, and using sanitizer wipes are strategies that can be implemented to reduce ethanol intoxication inside healthcare facilities.
Although this is a major life-threatening problem, there has been a lack of proper action taken by hospitals to switch to hand sanitizer dispensers that are non-disposable, fastened to the wall, and are well monitored. It is therefore very crucial to limit the availability of these products, especially in psychiatric wards and EDs, to prevent similar incidents.
Recognizing and monitoring alcoholic patients can be very challenging for the medical staff, especially in crowded EDs. Medical staff should be very careful when dealing with substance users, as they tend be manipulative.
Conclusions
Ethanol intoxication after ingestion of hand sanitizers or similar products is very common and can be life-threatening. Patients with alcohol dependence are known to develop alcohol-seeking behaviors. This report has highlighted that healthcare professionals should be aware that the increased availability of ethanol-based hand sanitizers, some of which contain toxic antiviral chemical agents, may be targeted by individuals with alcohol dependency.
Excessive alcohol users sometimes seek hospital care presenting with false complaints to get to these products; so strict supervision is necessary. This problem can be solved by simple actions that will help prevent major complications.
References:
1.. Babor TF, The Classification of alcoholics: Typology theories from the 19th century to the present: Alcohol Health Res World, 1996; 20(1); 6-14
2.. Nehring SM, Chen RJ, Freeman AM, Alcohol use disorder. [Updated 2023 Aug 8]: StatPearls [Internet], 2024, Treasure Island (FL), StatPearls Publishing Available from: https://www.ncbi.nlm.nih.gov/books/NBK436003/
3.. Gianoulakis C, Alcohol-seeking behavior: the roles of the hypothalamic-pituitary-adrenal axis and the endogenous opioid system: Alcohol Health Res World, 1998; 22(3); 202-10
4.. Gianoulakis C, Alcohol-seeking behavior: Alcohol Health and Research World, 1998; 22(3); 202-10
5.. Pourmand A, Ghassemi M, Frasure SE, Hand sanitizer intoxication in the Emergency Department: Cureus, 2021; 13(9); e17906
6.. Stevens DL, Hix M, Intentional ingestion of hand sanitizer in an adult psychiatric unit: Mental Health Clinician, 2020; 10(2); 60-63
7.. LaHood AJ, Kok SJ, Ethanol toxicity: StatPearls June 21, 2023, Treasure Island (FL), StatPearls Publishing
8.. Liontos A, Samanidou V, Athanasiou L, Acute ethanol intoxication: An overlooked cause of high anion gap metabolic acidosis with a marked increase in serum osmolal gap: Cureus, 2023; 15(4); e37292
9.. Yip L, Bixler D, Brooks DE, Serious adverse health events, including death, associated with ingesting alcohol-based hand sanitizers containing methanol – Arizona and New Mexico, May–June 2020: MMWR Morb Mortal Wkly Rep, 2020; 69(32); 1070-73
10.. Mahmood A, Eqan M, Pervez S, COVID-19 and frequent use of hand sanitizers; Human health and environmental hazards by exposure pathways: Sci Total Environ, 2020; 742; 140561
11.. Birková A, Hubková B, Čižmárová B, Bolerázska B, Current view on the mechanisms of alcohol-mediated toxicity: Int J Mol Sci, 2021; 22(18); 9686
12.. Vonghia L, Leggio L, Ferrulli A, Acute alcohol intoxication: Eur J Intern Med, 2008; 19(8); 561-67
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133