21 July 2024: Articles 
Diagnosis and Treatment of a 64-Year-Old Man with Chyle Leak Following Laparoscopic Cholecystectomy: A Case Report
Unusual clinical course, Challenging differential diagnosis, Unusual setting of medical care, Educational Purpose (only if useful for a systematic review or synthesis)
Mohammed Salim Zaatari1ABD*, Mohamad Zaki El Haress1ABCDEFG, Mohamad Ibrahim Siblini1ACD, Mohamad Ali Yassine1CE, Kamar Mohamad Said Hafez1EFDOI: 10.12659/AJCR.943429
Am J Case Rep 2024; 25:e943429






Abstract
BACKGROUND: Chyle leakage with chylous ascites is a rare complication of abdominal surgery, and few cases have been reported following cholecystectomy. This report is of a 64-year-old man with chyle leak following laparoscopic cholecystectomy and describes the diagnosis and approach to treatment. Immediate diagnosis, although challenging, remains imperative. Frequently, patients manifest nonspecific symptoms, such as abdominal discomfort or nausea. They can also exhibit milky discharge from drains and wounds. Abdominal fluid analysis is fundamental for diagnosis. The existence of elevated triglyceride levels in peritoneal fluid is indicative of chyle leakage.
CASE REPORT: We present a case report of a 64-year-old man with chyle leakage after laparoscopic cholecystectomy for acute cholecystitis, on postoperative day 2. A milky-white fluid was drained, and diagnosis was confirmed with elevated triglycerides upon fluid analysis. Chyle leakage decreased gradually until complete resolution at postoperative day 7, after dietary modifications and the closed-suction silicone drain was removed. The patient was symptom-free at a 2-month follow-up.
CONCLUSIONS: Although chyle leakage is a rare postoperative complication of laparoscopic cholecystectomy, early diagnosis and rapid multidisciplinary management are required. It is vital to consider this diagnosis even if the course of laparoscopic cholecystectomy was uncomplicated and with no anatomical variation. Thus, a closed-suction silicone drain and close monitoring of output is essential for early diagnosis. The dietary modification constitutes a cornerstone in the management of chyle leakage, and a surgical approach should be preserved for patients for whom the conservative approach fails or who have large volumes of chyle.
Keywords: Cholecystectomy, Laparoscopic, Cholecystitis, Acute, Chyle, Gallstones, Humans, Male, Middle Aged, Chylous Ascites, Postoperative Complications, Drainage
Introduction
Laparoscopic cholecystectomy is a globally performed procedure and is the criterion standard for removing the gallbladder. Each year, around 750 000 laparoscopic cholecystectomies are performed in the United States [1]. Although its elective execution results in low mortality (0.08–0.14% [2]) and morbidity (1.6–5.3% [2]), complications such as bile duct injuries can still arise [3].
Chyle leakage is an extremely uncommon complication of laparoscopic cholecystectomy, and only 7 cases have been reported in the literature [3–9]. Chylous ascites is an uncommon clinical condition, defined as a peritoneal deposition of chyle. The incidence is about 1 in 20 000 admissions over 20 years. Chylous ascites is usually caused by trauma or rupture of lymphatics. Treatment consists of a low-fat diet, medication (orlisat, somatostatin), non-surgical invasive intervention, and surgery. Mortality can reach 40% to 70%, making early diagnosis essential [10]. We will be describing the eighth case reported case of chyle leakage after laparoscopic cholecystectomy. Although it is extremely rare, chyle leakage carries significant complications, encompassing malnutrition, delayed wound healing, immunosuppression, and electrolyte imbalances [11].
Immediate diagnosis, although challenging, remains imperative. Frequently, patients manifest nonspecific symptoms, such as abdominal discomfort, nausea, or distension. They can also exhibit milky discharges from drains or wounds. Abdominal fluid analysis is fundamental for diagnosis. The existence of elevated triglyceride levels in the peritoneal fluid is indicative of a chyle leak.
There is currently no agreement on the most effective treatment approach for chyle leaks. However, commencing with conservative treatment and subsequently choosing surgical intervention for more complex cases is the standard approach. Conservative management focuses on diminishing intestinal lymph flow and replenishing protein, electrolyte, and fluid lost. However, its effectiveness has been variable, from 77% to 100% success in previous studies [12]. The surgical strategy involves draining the leaked chyle and subsequently ligating the responsible lymphatic vessel [13].
Furthermore, cholecystectomy can lead to other complications, such as bile duct injury which is still a major unpleasant complication, occurring in approximately 0.2% to 1.3% of cases [14]. Also, bleeding is rare but among the most serious complications [15]. This report is of a 64-year-old man with a chyle leak following laparoscopic cholecystectomy, and describes the diagnosis and approach to treatment.
Case Report
A 64-year-old non-alcoholic, non-smoking male patient with no past medical and surgical history, including a negative history of pancreatitis or its risk factors, presented to the surgery clinic with right upper quadrant pain of a 2-week duration. He had been taking ciprofloxacin 500 mg twice daily (without a physician’s prescription) and paracetamol every 6 h, with no clinical improvement.
Blood workup revealed a normal white blood cell count, neutrophil count, and bilirubin level. Ultrasonography revealed a thickened gallbladder wall, measuring 5.5 mm, partially contracted measuring 6×2.5 cm, that was almost full of hyper-echoic sludge and a stone reaching 2 cm, suggestive of chronic cholecystitis. Magnetic resonance cholangiopancreatography was not performed.
The patient underwent laparoscopic cholecystectomy the next day. The gallbladder was retracted over the liver, allowing for the dissection of the hepatocystic triangle to isolate the cystic artery in addition to the cystic duct and confirming the location (Figure 1). Once this view was adequately achieved, we isolated the cystic duct and cystic artery, in which the anatomy was completely normal, with no anatomical variation. Both were carefully clipped and transected (Figure 2), which made it less likely that a lymphatic duct could transverse the cystic artery that might be dissected, causing chyle leakage. Following ligation, the gallbladder was removed from the abdomen in a specimen pouch. The gallbladder bed was washed using warm normal saline, and hemostasis was achieved (Figure 3). A closed-suction silicone drain was placed in the sub-hepatic fossa, as per the surgeon’s preference for post-acute cholecystitis. The course of the surgery was smooth, with no complications, such as visible chyle duct injury, leakage, or bleeding.
Postoperatively, the patient was transferred to the ward, a clear fluid diet was started, to be advanced as tolerated, and prophylactic antibiotics (cefuroxime) were initiated.
On postoperative day 1, the drain output was 100 mL of serosanguinous fluid, with minimal right upper quadrant pain. On postoperative day 2, when an unrestricted regular diet was introduced, which included fat, the drain output became milky-white, and 180 mL were drained (Figure 4).
A chyle leak was suspected; thus, a fluid sample was sent for analysis, revealing an elevated triglyceride concentration of 460 mg/dL (reference range 40–170 mg/dL), consistent with a chyle leak.
Upon diagnosis, a conservative approach was provided with diet modification (fat-free and high-fiber diet), along with albumin and electrolyte replacement. Total parenteral nutrition (TPN) was not started, due to the patient’s refusal.
The drain effluent was 200 mL/day during postoperative days 3 and 4, decreasing progressively and changing in color through postoperative days 5 and 6 (Figure 5). Complete resolution of drain output was noted at postoperative day 7, with confirmation by ultrasound scanning. After 48 h of zero drain output, the silicone-closed suction drain was removed.
The patient was asymptomatic through the 2-month follow-up period. Intraoperative pathology revealed chronic calculus cholecystitis, with no dysplasia seen.
Discussion
Chyle leakage can be associated with high mortality; however, swift diagnosis and therapy can minimize complications. After a patient undergoes laparoscopic cholecystectomy, chyle leakage is an exceptionally rare occurrence, with only a handful of cases reported worldwide [6]. These leaks generally have a self-limiting nature and involve small volumes. However, when high-volume leaks do occur, they can lead to significant morbidity. Patients facing such leaks are at risk of sepsis and infections due to the lymph fluid’s rich lymphocyte composition. This fluid, once lost, collects in the abdominal cavity, potentially causing peritoneal irritation and giving rise to symptoms, such as abdominal pain, distention, fever, and other acute abdomen indicators [13]. Additionally, deficiencies in vitamins, protein, and calories can arise, accompanied by disruptions in electrolyte balance [7]. Presently, the underlying pathophysiology behind post-laparoscopic cholecystectomy chyle leakage remains unclear and lacks specific diagnostic criteria. Recent literature suggests that such leaks can arise after iatrogenic injury to a lymphatic vessel. The output and color of the fluid draining from the abdomen typically provide the most informative signs of lymphatic leakage [3]. Diagnosis of a chyle leak presents challenges. In many cases, patients exhibit nonspecific symptoms, such as nausea, abdominal discomfort, distention, or a milky discharge from drains and wounds. Analyzing the abdominal fluid can aid in confirming the diagnosis. The presence of a high triglyceride count exceeding 110 mg/dL (1.2 mmol/L) in the peritoneal cavity fluid is indicative of chyle leakage, reflecting a chylous ascites. The fluid is usually sterile, odorless, alkali, and abundant in lymphocytes, however, deficient in amylase as well as bilirubin [6]. The approach to managing chyle leaks after laparoscopic cholecystectomy can be categorized into 2 groups: non-surgical (conservative) and surgical. Commencing with non-surgical management is generally recommended, while surgical intervention is considered for more severe cases or after the failure of conservative treatment. Conservative management strategy focuses on diminishing the flow of lymph within the intestines and compensating for any losses of fluid, protein, or electrolytes. The usual lymph circulation rate through the thoracic duct is around 1 mL/kg/h, but this can surge to 200 mL/kg/h after the consumption of a fat-rich meal. Employing temporary TPN emerges as the most effective and fast means of reducing intestinal lymph flow, allowing for the recovery of impaired lymphatic circulation. Research has demonstrated that TPN by itself can effectively resolve cases, in a range of 77% to 100%. It is useful to retain the advantages of enteral feeding by introducing a diet low in fat yet rich in protein, supplemented with medium-chain triglycerides. Paracentesis proves beneficial for chylous ascites causing symptoms when no drainage tube is present. However, it is advisable to refrain from frequent paracentesis, owing to the potential risk of infections, heightened nutritional losses, and the chance of lengthening the leakage. If dietary adjustments alone fail to effectively diminish chylous ascites, pharmaceutical substances might be introduced to the treatment plan. The reported effectiveness varies. Compounds such as pancreatic lipase inhibitors (eg, orlistat) and synthetic somatostatin analogs (eg, octreotide) might assist in reducing triglyceride absorption and the flow of enteric chyle. Some investigations have shown notable improvements in outcome within a few days of subcutaneous administration or continuous infusion, while others have shown failure. The incorporation of octreotide alongside TPN or a diet rich in medium-chain triglycerides has demonstrated a significant acceleration in the healing of leaks, especially in hepatopancreatic biliary surgeries and nephrectomies. Commencing somatostatin therapy at a dosage of 100 µg 3 times daily is recommended. Moreover, there is a recommendation for antibiotic prophylaxis to avert the development of concurrent infections. Surgery serves as an additional fundamental aspect of management, particularly due to the occasional ineffectiveness of conservative methods. Essential clinical considerations for each scenario encompass the patient’s current health condition, the gravity of the chyle leak (particularly if it exceeds 500 mL per day), and the original surgical procedure. The objectives of surgical intervention encompass draining the leaked chyle and subsequently ligating the responsible lymphatic vessel. When performed by experienced practitioners, a laparoscopic approach can be both secure and viable, yielding successful outcomes when the leak is identifiable during the reoperation. Additionally, fibrin glue can be employed as a supplementary measure [13].
In our case, our index of suspicion of chyle leak was high after seeing the milky drain output, and our immediate response was to measure the triglyceride level, which confirmed our diagnosis, and after reviewing the literature, we were comfortable to start with the conservative management, especially since the drain output did not give large amounts.
With conservative management, the drain output in terms of volume and quality improved over the first 48 h after initiation, gradually decreasing and reaching zero after 7 days. The drain was removed after ultrasound confirmation. The improvement in our patient and the resolution of the chyle leak after dietary modifications only without the use of TPN and octreotide goes parallel with what is described in the literature, that dietary modification can be enough in certain patients to achieve complete resolution [5–8].
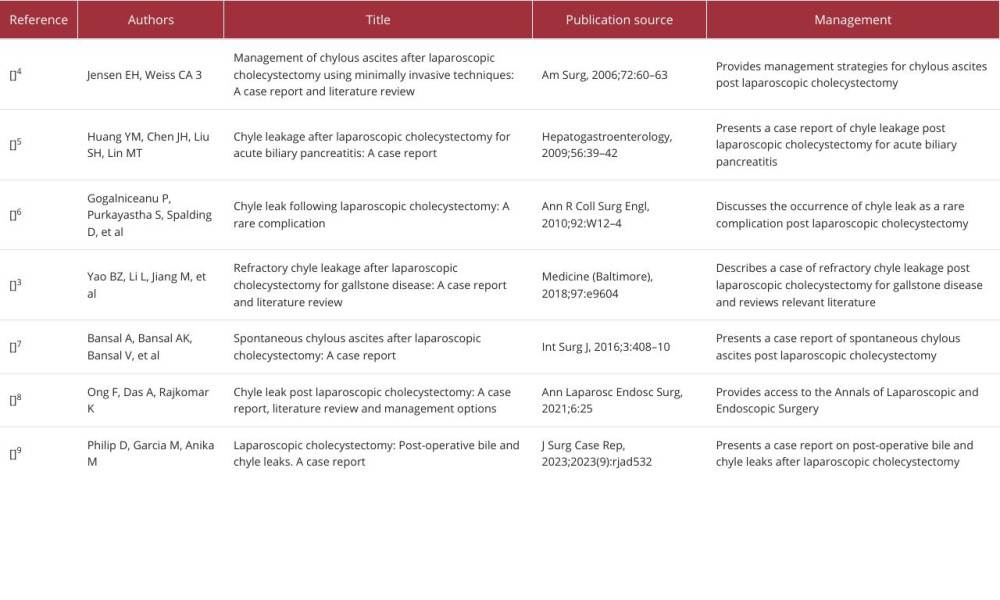
In the 7 reported cases of postoperative chyle leak, 3 cases responded to conservative, non-surgical management, and they all included a fat-free diet, similar to our practice [5,6,8] However, the remaining 4 cases required invasive intervention [3,4,7,9]. One case required laparoscopic exploration with identification of the site of the leak; this was controlled with suture ligation and fibrin glue, with immediate resolution of the leak [4]. Another case of chyle leak required open exploration, in which oversewing of the leak was done with prolene 3-0 and fibrin glue, and resolution of drain output after 7 months [3]. The third case required laparoscopy with aspiration of 1.4 L of chyle, with no identifiable leak site detected. A drain was inserted, although the patient showed intolerance to both Sandostatin and TPN. He was kept nil per os until day 5, when a fat-free diet was introduced. By day 4, the drain output reached 400 mL/day, eventually ceasing by day 15 [7]. The patient was discharged home on day 19. In the final case, an initial attempt at endoscopic retrograde cholangiopancreatography was unsuccessful, due to ampullary stenosis. Advanced endoscopic retrograde cholangiopancreatography with endoscopic ultrasound showed a normal biliary tree without bile leakage. A common bile duct sphincterotomy was performed, and a 10 French, 7-cm plastic stent was placed. Following this, the patient’s Jackson-Pratt drain output was reduced, and the patient reported less pain and improved diet tolerance. The patient was discharged on day 17 with instructions for Jackson-Pratt drain care, a low-fat diet, and prescription for octreotide. One month later, the patient showed complete resolution, and the percutaneous drain was removed [9]. Table 1 summarizes cases of chyle leak after laparoscopic cholecystectomy in the literature.
Conclusions
Chyle leakage is extremely rare; however, it constitutes a significant serious complication.
It is vital to consider this diagnosis even if the course of the laparoscopic cholecystectomy was uncomplicated and with no anatomical variation; thus, closed suction silicone drain and close monitoring of output is essential for early diagnosis. Dietary modification constitutes a cornerstone in the management of chyle leak, and a surgical approach should be preserved for patients for whom the conservative approach has failed or for those who have large volumes of chyle leak.
Figures
References:
1.. Vollmer CM, Callery MP, Biliary injury following laparoscopic cholecystectomy: Why still a problem?: Gastroenterology, 2007; 133(3); 1039-41
2.. Pucher PH, Brunt LM, Davies N, Outcome trends and safety measures after 30 years of laparoscopic cholecystectomy: A systematic review and pooled data analysis: Surg Endosc, 2018; 32; 2175-83
3.. Yao BZ, Li L, Jiang M, Refractory chyle leakage after laparoscopic cholecystectomy for gallstone disease: A case report and literature review: Medicine (Baltimore), 2018; 97; e9604
4.. Jensen EH, Weiss CA, Management of chylous ascites after laparoscopic cholecystectomy using minimally invasive techniques: A case report and literature review: Am Surg, 2006; 72; 60-63
5.. Huang YM, Chen JH, Liu SH, Lin MT, Chyle leakage after laparoscopic cholecystectomy for acute biliary pancreatitis: A case report: Hepatogastroenterology, 2009; 56; 39-42
6.. Gogalniceanu P, Purkayastha S, Spalding D, Chyle leak following laparoscopic cholecystectomy: A rare complication: Ann R Coll Surg Engl, 2010; 92; W12-14
7.. Bansal A, Bansal AK, Bansal V, Spontaneous chylous ascites after laparoscopic cholecystectomy: A case report: Int Surg J, 2016; 3; 408-10
8.. Ong F, Das A, Rajkomar K, Chyle leak post laparoscopic cholecystectomy: A case report, literature review and management options: Ann Laparosc Endosc Surg, 2021; 6; 25
9.. Philip D, Garcia M, Anika M, Laparoscopic cholecystectomy: Post-operative bile and chyle leaks. A case report: J Surg Case Rep, 2023; 2023(9); rjad532
10.. Dababneh Y, Mousa OY, Chylous ascites: StatPearls [Internet] Apr 24, 2023, Treasure Island (FL), StatPearls Publishing
11.. Delaney SW, Shi H, Shokrani A, Sinha UK, Management of chyle leak after head and neck surgery: Review of current treatment strategies: Int J Otolaryngol, 2017; 2017; 8362874
12.. Ong F, Das A, Rajkomar K, Chyle leak post laparoscopic cholecystectomy: A case report, literature review and management options: Ann Laparosc Endosc Surg, 2021; 6; 25
13.. Tulunay G, Ureyen I, Turan T, Chylous ascites: analysis of 24 patients: Gynecol Oncol, 2012; 127(1); 191-97
14.. Zidan MHE, Seif-Eldeen M, Ghazal AA, Refaie M, Post-cholecystectomy bileduct injuries: A retrospective cohort study: BMC Surg, 2024; 24(1); 8 [Erratum in: BMC Surg. 2024;24(1):48]
15.. Suuronen S, Kivivuori A, Tuimala J, Paajanen H, Bleeding complications in cholecystectomy: A register study of over 22,000 cholecystectomies in Finland: BMC Surg, 2015; 15; 97
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133