01 August 2024: Articles 
A 52-Year-Old Man with Aneurysmal Subarachnoid Hemorrhage Associated with Delayed-Onset Vitreous Hemorrhage (Terson’s Syndrome) Successfully Treated with Balloon-Assisted Coiling and Delayed Vitrectomy
Challenging differential diagnosis, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis)
Thanos Vassilopoulos1ABCDEF, Christos Tsitsipanis12ABCDEF, Anastasios Stavrakakis3ACDE, Konstantinos Ntotsikas2ABCDEF*, Nikolaos MoustakisDOI: 10.12659/AJCR.943567
Am J Case Rep 2024; 25:e943567






Abstract
BACKGROUND: Terson’s syndrome (TS) is a medical condition characterized by intraocular bleeding that can lead to visual impairment and is associated to subarachnoid hemorrhage (SAH). The pathophysiology and natural history are not well established in the current literature. This report describes successful treatment of a 52-year-old man with aneurysmal SAH who developed late-onset TS using balloon-assisted coiling and vitrectomy to raise awareness of this important complication of aneurysmal SAH.
CASE REPORT: A 52-year-old smoker with no known past medical history presented to the emergency department with a sudden, severe headache that worsened with photophobia and phonophobia. The patient had a diffuse SAH and underwent an embolization procedure. After 48 hours of close Intensive Care Unit monitoring, the patient’s vital signs were stable, and the GCS score was consistently 15/15. However, after 3 weeks in the hospital, the patient experienced blurred vision and a right upper quadrantanopia. Further examination revealed TS and the patient underwent a vitrectomy in 1 eye. The surgery was successful and the eye recovered to 20/20 with no complications. However, the other eye showed slow absorption of the hemorrhage, and a vitrectomy was scheduled for that eye as well.
CONCLUSIONS: TS is a complication of aneurysmal SAH that can lead to vision loss and increased morbidity. It often goes undiagnosed, and ophthalmologists are not regularly consulted. Late manifestation of the condition is exemplified by the present case. Early detection and intervention are crucial for better patient outcomes.
Keywords: Subarachnoid Hemorrhage, Vitreous Hemorrhage, Visual Acuity, Aneurysm, Intracranial Berry, 1, Eye Hemorrhage, Retinal Hemorrhage, Humans, Male, Middle Aged, Vitrectomy, Syndrome, Embolization, Therapeutic
Introduction
RETINAL VENOUS CONGESTION THEORY:
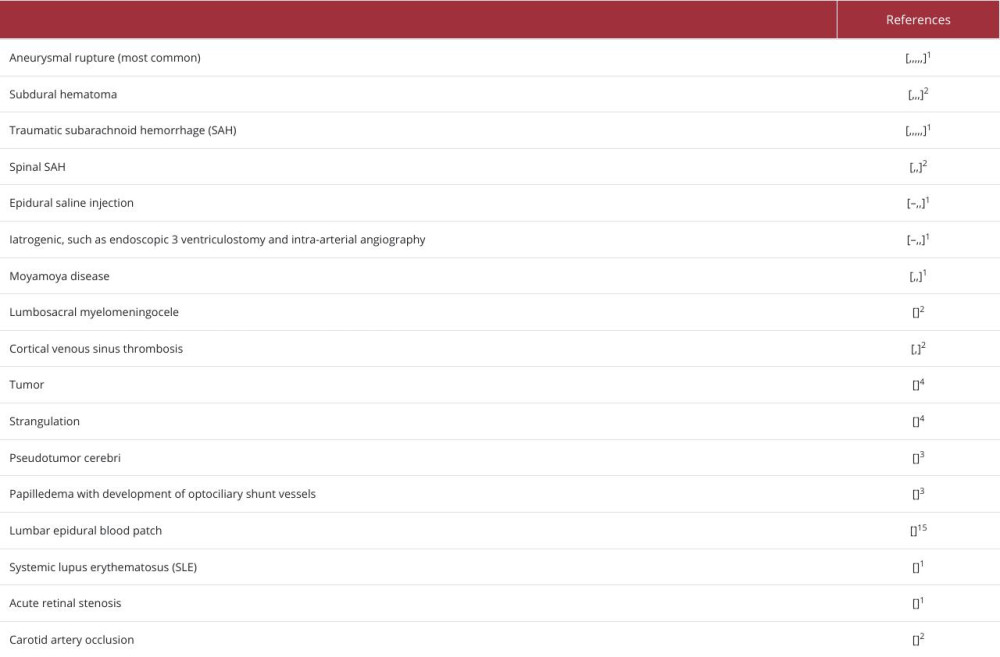
According to the prevailing theory in the literature, the sudden increase in ICP following SAH interrupts the drainage of cerebrospinal fluid (CSF) along the optic nerve sheath, owing to the hydrostatic gradient [1–3,6,7,15,18,36]. As a result, the elevated pressure transmitted through the sheath can cause acute intraocular venous hypertension and, by extension, rupture of retinal vessels [1–3,6,7,15,18,36]. This phenomenon indicates that the ocular bleeding in TS does not have a subarachnoid origin [1–3,6,7,15,18,36]. However, although this is the dominant theory, some points can question this proposed mechanism. An acute elevation of ICP causing rupture of retinal vessels should develop TS immediately; instead, it is shown that TS occurrence can vary from minutes to days or weeks after the rise of ICP [36]. In addition, not all the pathologies that induce elevation of ICP cause such a frequency of intraocular hemorrhages [37], and no known mechanism has been proposed for how ICP can cause the rupture of those specific vessels [36,38]. Therefore, we also present the other proposed mechanisms.
TRANS-LAMINA CRIBROSA THEORY:
Studies supporting this theory suggest that intracranial blood enters the vitreous cavity through the lamina cribrosa of the sclera, although there is no direct connection between the subarachnoid space of the optic nerve and the vitreous space [1,4,15,18,35,36].
PERIVASCULAR LEAK THEORY:
A possible mechanism may be entry of the blood from a SAH into the intraocular compartment via perivascular (Virchow-Robin) spaces [1]. However, this theory is debatable due to the limited number of studies supporting this pathophysiologic mechanism [1].
PERIPAPILLARY LEAK THEORY:
Another proposed mechanism, supported by a specific case report, is the destruction of peripapillary tissue due to the SAH-induced elevation of the ICP [1].
PRIMARY VITREOUS THEORY:
Another questionable proposed mechanism is the entrance of blood to the intraocular space via specific vessels, such as sub-retinal and vessels proximal to the optic nerve, but also via the sub-internal limiting membrane (sub-ILM) [1].
GLYMPHATIC REFLUX:
This theory states that the glymphatic pathway is an extravascular anatomical connection between the subarachnoid space and retina, although glymphatic channels have not been shown to exist yet [4,7,37]. However, aquaporin-4 (AQP4) is suggested to play an essential role in lymphatic efflux, and thus is considered a milestone of the glymphatic system studied for its contribution to the pathophysiologic pathway of many neurological diseases, such as Alzheimer’s, post-traumatic neurode-generation, normal pressure hydrocephalus, Parkinson’s disease, cerebral stroke, and vascular dementia [39–42].
Various studies have analyzed histopathological specimens from patients with TS, revealing the presence of erythrocytes and leukocytes in different intraocular spaces [30,43]. Other studies have also noted the presence of glial cells and basement membrane material accompanying hemorrhages in the spaces above [30,43].
The first step in assessment of TS is to recognize the specific patient profile that has a high index of suspicion in favor of TS, as mentioned above [1,6]. Then, there are different methods and techniques that contribute to the diagnosis of TS [3]. The criterion standard examination to identify TS is fundoscopy with indirect ophthalmoscope for most cases or direct ophthalmoscope for emergency cases only [1,2,4,6,10,12,14,15,20,21,29,35,44]. For the fundoscopy to be more sensitive in detecting the intraocular hemorrhage, the technique must be performed after the patient has received mydriasis-inducing medication [1,4,5,12]. Ophthalmologic examination for all patients with SAH is essential to identify TS, as its presence is a crucial factor for the patient’s general condition [2,5,6,10,14,15,21,28,34]. Ocular sonography, and in particular, the B-mode of ocular ultrasonography, appears to be a valuable diagnostic tool for confirming the diagnosis of TS [2,4,5,7,10,15,29]. Numerous studies demonstrated the valuable role of visual acuity monitoring and intraocular hemorrhage evolution assessment through the use of retinal imaging technology [2,5,10,15]. Furthermore, the early detection of potential syndrome complications, such as retinal detachment, can be facilitated by its utilization [2,4,7,10,15].
Computed tomography (CT) and optical coherence tomography (OCT) are other tools that can contribute to diagnosing TS and provide information about its severity [2,6,14,20,26,35,45]. Despite having the disadvantage of radiation exposure, these techniques can confirm the diagnosis made by fundoscopic examination, detect possible complications, or rule out the presence of TS in patients with no visual symptoms and a negative CT scan [2,6,7,10,14,15,20,25,26,28,29,45]. Several techniques, some in the general context and others in more specific cases, can be an extra tool for assessment of TS: computed tomography angiography (CTA), magnetic resonance imaging (MRI), fluorescein angiography, and visual evoked potentials (VEPs) [1,14,44].
The therapeutic approach for TS can be classified as either non-surgical or surgical [3,11,18,46]. Some studies suggest conservative management, while others advocate early surgical intervention to prevent intraocular hemorrhage complications [1–3,5,6,15,18,20,23,24,32,33,46]. The conservative approach typically involves closely monitoring the hemorrhage and allowing it to resolve spontaneously [1,5,7,29]. It is commonly recommended that patients rest in bed with head elevated, have adequate fluid intake, and abstain from taking anticoagulant medications or nonsteroidal anti-inflammatory drugs [1,4,5,7,15,32]. The recommended surgical approach for aggressive treatment is pars plana vitrectomy [2,3,5,6,8,29,30,32–34,46]. This is typically advised when hemorrhages persist for more than 3–6 months, and after 4–8 weeks for bilateral cases to avoid complications [1–3,5,8,10–12,23,24,29,33,46]. Indications for early choice of the surgical approach include sub-macular hemorrhage, binocular damage with severe visual loss, and pediatric patients at high risk of amblyopia [2,5,7,32,34]. Complications of pars plana vitrectomy are retinal detachment, endophthalmitis, retinal damage, entry site breaks, cataract formation, dissociated optic nerve fiber, maculopathy, and epiretinal membrane formation [1,44]. In some instances where standard treatment has not been effective, surgical interventions such as neodymium-doped yttrium aluminum garnet (Nd: YAG) laser posterior hyaloidotomy and intravitreal injection therapies may be considered [1,23].
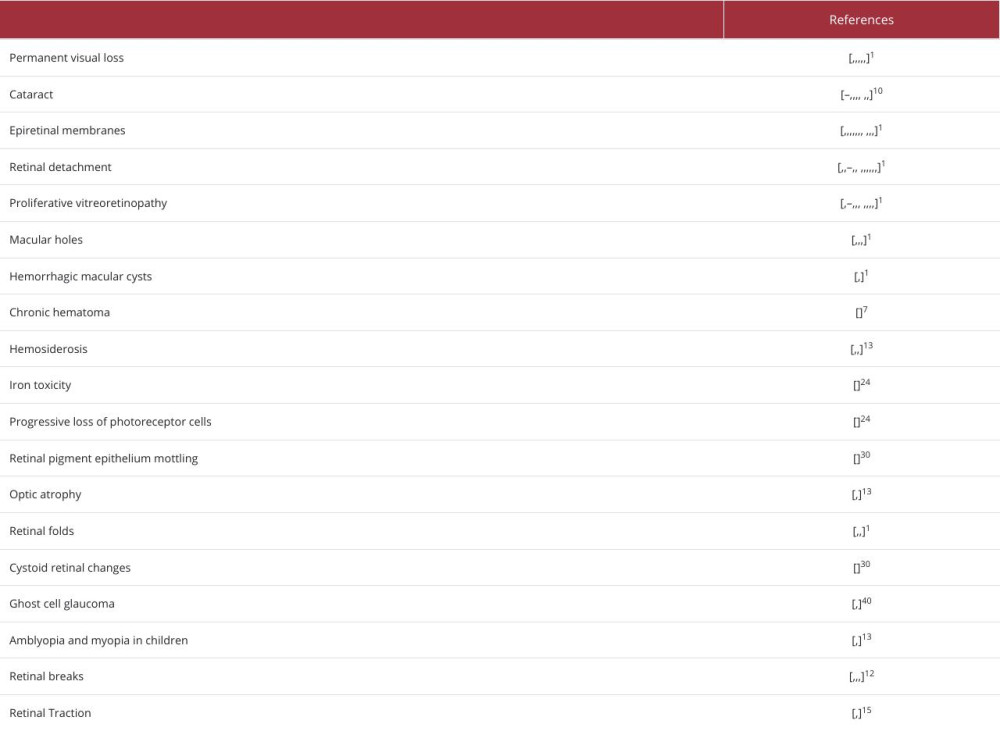
Complications, as shown in Table 2, can result from TS due to late administration of therapy, the possible aggressive nature of the syndrome, and the poor general condition in some patients [1,4,5,7,10–15,18,20,23,24,29,30,34,43,44,47]. Several studies have demonstrated that the mortality rate is significantly higher in patients with SAH who also have TS, ranging from 6.3% to 90% [1,2,4,6,19,22,29,33,34,46]. Moreover, there appears to be a correlation between poor prognostic features of patients with SAH upon admission – such as a low GCS score, high Hunt and Hess grade, high WFNS score, and high Fischer grades – and the likelihood of developing an intraocular complication [1,2,6,15,21,33,34,46,47].
Regarding the prognosis of TS syndrome alone, different studies suggest that the visual prognosis is favorable due to the frequent resolution of intraocular hemorrhage, either spontaneously or iatrogenic [6,7,19,30,45,48].
To the best of our knowledge, there are no known cases of late-onset TS following an aneurysmal SAH (aSAH). Here, we present a case of a 52-year-old man who developed TS 21 days after an aSAH. He was successfully treated with balloon-assisted coiling of an intracerebral aneurysm and delayed vitrectomy for intraocular hemorrhage. We present this case for academic and educational purposes. The submission of this case to the literature is of immense significance in highlighting the potential occurrence of a severe form of aSAH in a delayed manner. We aim to raise awareness about this significant complication among medical professionals and the general public.
Case Report
A 52-year-old male smoker with no known past medical history presented to the emergency department with a sudden, severe headache that worsened with photophobia and phonophobia. The initial physical examination revealed hypothermia (35°C) and hypertension, with a heart rate of 65 beats per minute. He was alert, awake, and oriented, spontaneously opening his eyes and following commands. No limb paresis, ataxia, or sensory loss were observed. The presence of nuchal rigidity was notable and underscored the severity of the associated pain. The results of the head CT indicated that the patient had diffuse SAH, located mainly in the interhemispheric fissure, basal cisterns, the frontotemporal subarachnoid space, and the convexity of the parietal lobe bilaterally, with a concomitant phlogistic hemorrhagic lesion in the right inferior and middle frontal gyrus (Figures 1–3). The patient was classified as Grade 3 on the Fischer scale (the original form of the Fisher scale) and Grade 2 on the Hunt and Hess scale. Following his initial examination, he underwent digital subtraction angiography (DSA), which revealed a saccular aneurysm in the ACoA (Figure 4). Following the diagnosis, he underwent an embolization procedure to address the aneurysm (Figure 4). The procedure entailed using multiple micro-coils in conjunction with a balloon to temporarily obstruct the neck of the aneurysm, commonly referred to as balloon-assisted coiling.
Following the embolization procedure, the patient had an episode of seizures and was subsequently started on anti-epileptic medication (Levetiracetam 500 mg IV bid). He was then closely monitored in the Intensive Care Unit (ICU) for 48 h. Throughout his stay in the ICU, he consistently maintained a GCS of 15/15, was afebrile and had stable vital signs, and was free from any further seizures. He was administered oral nimodipine to manage his condition, while irbesartan was required to regulate his blood pressure. He also received systemic tramadol and paracetamol for pain management. He had no increased inflammation serum biomarkers.
Upon discharge from the ICU, he was transferred to the Department of Neurosurgery, where he received medical care and had a favorable course of hospitalization. His headache gradually subsided. During his stay in the Department of Neurosurgery, he was diagnosed with a
Discussion
The present case report has certain limitations. We did not take any images of fundoscopy or ocular ultrasound, nor did we take any photos from the operating theater where the vitrectomy was performed. However, we have made every effort to present the case as accurately and comprehensively as possible based on the available data. Please note that the second operation on the other eye is still pending; hence, we cannot provide the final outcome after all procedures. We understand the significance of this information in helping readers comprehend the case we are presenting. However, the principal aim of this study was to apprise medical practitioners of a commonly misdiagnosed condition that can significantly impact a patient’s functional outcome following an episode of aSAH. Moreover, it is imperative to note that this complication surfaced at a later stage, thereby constituting a defining feature of this case and a noteworthy addition to the existing literature.
At the time of the aneurysm rupture, our patient was 52 years old. Ko and Knox conducted pathologic examinations on the eyes of patients who developed TS after vasculogenic intracranial hemorrhage, and the mean age of the patients was 56.1 years; however, as the specimens were acquired from deceased patients, the results may only pertain to severe cases [43]. In several prospective and retrospective case series studies, mean ages ranged from 49.2 to 56.1 years old [2,10,13,47]. In addition, most case reports refer to patients of this age [15,19,49]. Karadzic et al reported a patient with vitreous hemorrhage following SAH who was treated conservatively but developed ghost cell glaucoma [32]. Sung et al found a lower proportion of vitreous hemorrhage compared to pre-retinal and intraretinal hemorrhage [47]. Moraru et al reported a 42-year-old patient who developed TS after experiencing an intracranial aneurysm rupture and vitreous hemorrhage who also required surgery in both eyes, with a favorable outcome [30]. In the case report by Hassan et al, TS was clinically detected on day 20 of hospitalization, but the patient had a low level of consciousness [6]. Therefore, we cannot be certain of the exact timing of onset. In their prospective study, Czorlich et al found 2 patients with delayed-onset TS on postictal day 14, and both patients had an otherwise uneventful clinical course [2].
It is postulated that vitreous hemorrhage may lead to deleterious effects on the internal limiting membrane, thereby causing impairment of visual function in the affected ocular organs [43]. TS is associated with patients who have higher severity of hemorrhage [1,2,13,20,28]. Joswig et al and Stienen et al reported that the location of the ruptured aneurysm and the severity of consequent hemorrhage were linked to the development of TS in their prospective studies [20,28]. Moreover, aneurysms located in the anterior circulation and those associated with higher Hunt and Hess scores and Fisher scores and lower GCS were associated with the occurrence of TS [20,28]. Interestingly, Czorlich et al found no correlation between TS and the location of the aneurysm [2]. In the same study, TS occurrence was not statistically significant despite being associated with aneurysm diameter [2]. However, with increasing Hunt and Hess score and Fisher score, and a lower GCS, the incidence of TS increased significantly [2]. In addition, Gottsche et al showed that increased severity of aSAH, as indicated by the Fisher scale score, WFNS grading system, and GCS, was significantly associated with a higher incidence of TS [29]. Gottsche et al found seizures were a significant predictor of TS, independent of other factors [29]. In their retrospective case series study, Lee et al identified the diameter of the aneurysm dome as a statistically significant risk factor for the development of TS [14].
Skevas et al performed vitrectomy on 60% of patients with TS and achieved excellent outcomes; the period of time between the first diagnosis and the operation was 3–5 months, and the sample size was small [13]. Gottsche et al also found favorable outcomes after surgery for TS in their prospective study [29]. Gordinho et al described the case of a 45-year-old patient with TS who underwent urgent eye surgery to treat vitreous hemorrhage [22]; the procedure had a favorable outcome for only 1 eye [22].
Our patient had a good clinical outcome, despite the need for intraocular hemorrhage surgery; however, the literature suggests that TS patients have high mortality rates [20,28,47].
Regarding the pathophysiology of intraocular hemorrhage, it can be inferred that the emergence of TS in the patient 21 days after the initial event of aneurysm rupture is not in line with the theory of intracranial hypertension. Prior ophthalmological examinations were not conducted, which makes it difficult to determine the exact time when the hemorrhage began. Moreover, the CT scans of the patient did not appear to indicate any evidence of intraocular hemorrhage. The literature contains several cases in which TS was the sole manifestation of subarachnoid hemorrhage [16,19,33,50]. Underdiagnosis is a common issue with TS, and it is rare for ophthalmologists to be consulted for this condition [10,13]. Healthcare professionals who have treated TS reported the importance of vigilance in identifying and diagnosing this condition [6,11,16,19,30,32,33,50].
The literature on the incidence, prevalence, and mortality rates of TS suggests that there is a dearth of information regarding its epidemiology. Future descriptive statistical analyses of this syndrome may be crucial in gaining a comprehensive understanding of its epidemiology and pathophysiology. Such studies can play a significant role in unraveling the complexities associated with TS and aiding clinicians in devising appropriate management and treatment strategies. To detect retinal detachment, it is important for physicians to be aware of the presence of TS [2]. Early surgical intervention may be necessary to prevent severe complications and permanent loss of vision [2]. Understanding the pathophysiologic pathway plays a crucial role in detecting the syndrome, given the diverse definitions in the literature. It is imperative to establish a consensus on the definition of the syndrome to facilitate accurate diagnosis and effective treatment.
Conclusions
TS is frequently overlooked, resulting in delayed diagnosis and management, and ophthalmologists are not regularly consulted in such cases. It is important to raise awareness of this issue, as early detection and intervention can greatly improve overall health outcomes.
Aneurysmal subarachnoid hemorrhage is a medical condition that carries a high risk of mortality and morbidity. Therefore, early detection of its complications is essential. One such complication is TS, which is associated with vision loss and increased morbidity. It may also manifest late, as illustrated by the case presented here; it is essential to identify the patient population that is at risk for developing TS and related complications. To this end, further prospective studies are warranted to help clinicians provide timely and appropriate treatment for patients at risk.
Figures
References:
1.. Aboulhosn R, Raju B, Jumah F, Terson’s syndrome, the current concepts and management strategies: A review of literature.: Clin Neurol Neurosurg., 2021; 210; 107008
2.. Czorlich P, Skevas C, Knospe V, Terson syndrome in subarachnoid hemorrhage, intracerebral hemorrhage, and traumatic brain injury: Neurosurg Rev, 2015; 38(1); 129-36
3.. Lima-Fontes M, Leuzinger-Dias M, Rodrigues R, Terson syndrome – clinical presentation, management, and visual outcomes in a tertiary centre: Clin Ophthalmol, 2023; 17; 351-59
4.. Maslias E, Vijiala S, Epiney JB, Terson syndrome: Not to be missed in patients with disorders of consciousness.: Brain Sci., 2023; 13(6); 879
5.. Sharma R, Shrestha J, Terson’s syndrome.: Nepal J Ophthalmol, 1970; 1(1); 77-79
6.. Hassan A, Lanzino G, Wijdicks EFM, Terson’s syndrome: Neurocrit Care, 2011; 15(3); 554-58
7.. Issiaka M, Mchachi A, Rachid R, Terson syndrome: Two case reports.: Int J Surg Case Rep., 2022; 90; 106700
8.. McCarron MO, A systematic review of Terson’s syndrome: Frequency and prognosis after subarachnoid haemorrhage.: J Neurol Neurosurg Psychiatry, 2004; 75(3); 491-93
9.. Baker ML, Hand PJ, Tange D, Terson’s syndrome in spontaneous spinal subarachnoid haemorrhage: J Clin Neurosci, 2008; 15(3); 313-16
10.. Bäuerle J, Gross NJ, Egger K, Terson’s syndrome: Diagnostic comparison of ocular sonography and CT: J Neuroimaging, 2016; 26(2); 247-52
11.. Reale C, Brigandì A, Gorgoglione N, Terson’s syndrome: Pract Neurol, 2020; 20(2); 163-64
12.. Czorlich P, Burkhardt T, Knospe V, Ocular ultrasound as an easy applicable tool for detection of Terson’s syndrome after aneurysmal subarachnoid hemorrhage.: PLoS One, 2014; 9(12); e114907
13.. Skevas C, Czorlich P, Knospe V, Terson’s syndrome – rate and surgical approach in patients with subarachnoid hemorrhage.: Ophthalmology, 2014; 121(8); 1628-33
14.. Lee GI, Choi KS, Han MH, Practical incidence and risk factors of Terson’s syndrome: A retrospective analysis in 322 consecutive patients with aneurysmal subarachnoid hemorrhage: J Cerebrovasc Endovasc Neurosurg, 2015; 17(3); 203
15.. Ren Y, Wu Y, Guo G, Terson syndrome secondary to subarachnoid hemorrhage: a case report: World Neurosurg, 2019; 124; 25-28
16.. Murthy S, Salas D, Hirekataur S, Ram R, Terson’s syndrome presenting as an ophthalmic emergency: Acta Ophthalmol Scand, 2002; 80(6); 665-66
17.. Dörner L, Alfke K, Barth H, Mehdorn HM, A subarachnoid haemorrhage primarily presenting as Terson’s syndrome: Cent Eur Neurosurg, 2009; 70(02); 89-90
18.. Paquette F, Darsaut TE, Sebag M, Weill A, Terson’s syndrome: Can J Neurol Sci J Can Sci Neurol, 2010; 37(6); 861-62
19.. Moynihan G, Robinson K, Terson’s syndrome: Subarachnoid haemorrhage presenting as sudden visual loss: Emerg Med Australas, 2012; 24(4); 454-56
20.. Stienen MN, Lücke S, Gautschi OP, Harders A, Terson haemorrhage in patients suffering aneurysmal subarachnoid haemorrhage: A prospective analysis of 60 consecutive patients: Clin Neurol Neurosurg, 2012; 114(6); 535-38
21.. Wu LN, He T, Xing YQ, Shen Y, Incidence of Terson’s syndrome in patients with SAH in a Chinese hospital: Curr Eye Res, 2013; 38(1); 97-101
22.. Leonardo Gordinho A, Rosado S, Blind spot: Blindness as initial presentation of subarachnoid haemorrhage.: BMJ Case Rep. , 2018; 2018 bcr2017222745
23.. Burgos-Blasco B, Moreno-Morillo FJ, Hernández-Ruiz S, Terson syndrome: Vitrectomy vs Nd: YAG hyaloidotomy: J Fr Ophtalmol, 2019; 42(6); e263-e66
24.. Citirik M, Tekin K, Teke MY, Terson syndrome with persistent vitreous hemorrhage following traumatic brain injury.: Saudi J Ophthalmol, 2019; 33(4); 392-97
25.. Stewart MW, Hasan SA, Collins C, Can baseline computed tomography scans be used to identify patients at high risk of vision loss due to Terson syndrome?: Am J Ophthalmol, 2020; 211; 217-28
26.. Koskela E, Pekkola J, Kivisaari R, Comparison of CT and clinical findings of Terson’s syndrome in 121 patients: A 1-year prospective study: Clinical article: J Neurosurg, 2014; 120(5); 1172-78
27.. Obuchowska I, Turek G, Mariak Z, Mariak Z, Early intraocular complications of subarachnoid haemorrhage after aneurysm rupture: Neuro-Ophthalmol, 2014; 38(4); 199-204
28.. Joswig H, Epprecht L, Valmaggia C, Terson syndrome in aneurysmal subarachnoid hemorrhage – its relation to intracranial pressure, admission factors, and clinical outcome: Acta Neurochir (Wien), 2016; 158(6); 1027-36
29.. Göttsche J, Knospe V, Sauvigny T, Terson syndrome in patients with aneurysmal subarachnoid hemorrhage: A 10-year single-center experience: Neurocrit Care, 2023; 39(1); 155-61
30.. Moraru A, Mihailovici R, Costin D, Brănişteanu D, Terson’s syndrome – case report: Romanian J Ophthalmol, 2017; 61(1); 44-48
31.. Ogawa T, Kitaoka T, Dake Y, Amemiya T, Terson syndrome: Ophthalmology, 2001; 108(9); 1654-56
32.. Karadzic J, Kovacevic I, Stefanovic I, Risimic D, Terson’s syndrome: A report of two cases: Srp Arh Celok Lek, 2015; 143(9–10); 595-98
33.. Choudhari K, Pherwani A, Gray W, Terson’s syndrome as the sole presentation of aneurysmal rupture: Br J Neurosurg, 2003; 17(4); 355-57
34.. Mazza JM, Tank P, LoPresti MA, Terson syndrome secondary to aneurysmal subarachnoid hemorrhage in a child: Illustrative case.: J Neurosurg Case Lessons., 2023; 5(25) CASE2390
35.. Czorlich P, Skevas C, Knospe V, Terson’s syndrome – pathophysiologic considerations of an underestimated concomitant disease in aneurysmal subarachnoid hemorrhage.: J Clin Neurosci, 2016; 33; 182-86
36.. Hayreh SS, Pathogenesis of Terson syndrome: Indian J Ophthalmol, 2022; 70(12); 4130-37
37.. Kumaria A, Gruener AM, Dow GR, An explanation for Terson syndrome at last: The glymphatic reflux theory: J Neurol, 2022; 269(3); 1264-71
38.. Kumaria A, Terson syndrome as a marker of severity in acute brain injuries: More than meets the eye: Neurol Engl Ed, 2022; 37(9); 827-28
39.. Peng S, Liu J, Liang C, Aquaporin-4 in glymphatic system, and its implication for central nervous system disorders: Neurobiol Dis, 2023; 179; 106035
40.. Gao Y, Liu K, Zhu J, Glymphatic system: An emerging therapeutic approach for neurological disorders.: Front Mol Neurosci., 2023; 16; 1138769
41.. Gao Y, Liu K, Zhu J, Glymphatic system: An emerging therapeutic approach for neurological disorders.: Front Mol Neurosci., 2023; 16; 1138769
42.. Ding Z, Fan X, Zhang Y, The glymphatic system: A new perspective on brain diseases.: Front Aging Neurosci., 2023; 15; 1179988
43.. Ko F, Knox DL, The ocular pathology of Terson’s syndrome.: Ophthalmology, 2010; 117(7); 1423-29.e2
44.. Middleton K, Esselman P, Lim PC, Terson syndrome: An underrecognized cause of reversible vision loss in patients with subarachnoid hemorrhage: Am J Phys Med Rehabil, 2012; 91(3); 271-74
45.. Iwase T, Tanaka N, Bilateral subretinal haemorrhage with Terson’s syndrome: Graefes Arch Clin Exp Ophthalmol, 2006; 244(4); 507-9
46.. Neß T, Janknecht P, Berghorn C, Frequency of ocular hemorrhages in patients with subarachnoidal hemorrhage: Graefes Arch Clin Exp Ophthalmol, 2005; 243(9); 859-62
47.. Sung W, Arnaldo B, Sergio C, Terson’s syndrome as a prognostic factor for mortality of spontaneous subarachnoid haemorrhage: Acta Ophthalmol (Copenh), 2011; 89(6); 544-47
48.. Gress DR, Wintermark M, Gean AD, A case of Terson syndrome and its mechanism of bleeding: J Neuroradiol, 2013; 40(4); 312-14
49.. Gauntt CD, Sherry RG, Kannan C, Terson syndrome with bilateral optic nerve sheath hemorrhage: J Neuroophthalmol, 2007; 27(3); 193-94
50.. Inoue T, Tsutsumi K, Shigeeda T, Terson’s syndrome as the initial symptom of subarachnoid hemorrhage caused by ruptured vertebral artery aneurysm: Case Report. Neurol Med Chir (Tokyo), 2006; 46(7); 344-47
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133