06 November 2024: Articles 
Priapism Following Coronary Angiography: A Case Report and Clinical Insights for Diagnosis and Management
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Unexpected drug reaction, Clinical situation which can not be reproduced for ethical reasons, Rare coexistence of disease or pathology
Tuersunjiang Naman1E, Najina Wugeti1B, Juan Sun1F, Refukaiti Abuduhalike1B, Nida Aslam1F, Ailiman Mahemuti2A*DOI: 10.12659/AJCR.943609
Am J Case Rep 2024; 25:e943609






Abstract
BACKGROUND: Priapism is a persistent penile erection that lasts longer than 4 hours. The most common causes of priapism are ischemia and the effects of drugs, including PDE-5 inhibitors, such as sildenafil and anticoagulants. Here, we describe the presentation and management of a 50-year-old man with priapism following coronary artery angiography for the investigation of ischemic heart disease (IHD).
CASE REPORT: A 50-year-old man was admitted to the Department of Cardiovascular Disease with the chief concern of intermittent precordial pain and discomfort for 1 year. After performing regular medical tests in the hospital, we confirmed that there was a need to identify the cause of the chest pain. Thus, after obtaining informed consent, we performed coronary angiography and diagnosed the patient with coronary artery disease based on the results of coronary angiography. However, half an hour after coronary angiography, he developed priapism. By performing ultrasound of the penis, we found that there was a thrombus in the penile vein. By combining blood aspiration from the corpus cavernosum of the penis with injection of hydroxylamine into the corpus cavernosum, we achieved a good treatment effect.
CONCLUSIONS: Priapism is becoming more common in middle-aged men. It should be treated as a medical emergency according to current management guidelines, and the underlying cause should be identified to prevent recurrence.
Keywords: Coronary Angiography, Penile Erection, Priapism, Humans, Male, Middle Aged, Penis, Myocardial Ischemia
Introduction
Cardiovascular disease (CVD) is the most common cause of death in European Society of Cardiology (ESC) member countries. The total number of CVD deaths across all ESC member countries far exceeds the number of cancer deaths. One hundred thirteen million individuals across ESC member countries continue to live with CVD. There is no decline in CVD mortality in many countries; thus, CVD is the most common cause of death [1], and coronary artery disease (CAD) accounts for a large portion of CVD-related deaths. Coronary angiography (CAG) is the criterion standard for evaluating the coronary artery lumen due to its high spatial and temporal resolution [2] and thus is widely used to diagnose CAD worldwide.
As CAG is an invasive procedure, there are specific patient-dependent and procedure-related complications of CAG [3]. The most common complications of CAG are cardiogenic death, myocardial infarction, arterial embolism, ventricular fibrillation, vascular injury, serious cardiac arrhythmias, local hemorrhage, hematoma, heart failure, and anaphylaxis [4]. However, no study has reported priapism after CAG as a complication of CAG.
Priapism is a full or partial erection that continues more than 4 hours beyond sexual stimulation and orgasm or is unrelated to sexual stimulation [5].
Although priapism is comparatively rare, with an incidence of 1.5 per 100 000 person-years [6], we encountered an unusual case of priapism after coronary angiography.
The purpose of this case report is to share with clinicians new insights into how priapism can occur after coronary angiography, to analyze the possible reason for this phenomenon, and to share the treatment process and outcomes.
Case Report
A 50-year-old man was admitted to the Department of Cardiovascular Disease with the chief concern of intermittent precordial pain and discomfort for 1 year.
The medical history revealed that he was diagnosed with hypertension 4 years prior and was prescribed an antihypertensive drug: allisartan isoproxil 240 mg/day. Moreover, he was diagnosed with obstructive sleep apnea syndrome (OSAS) 5 years previously and was put on a ventilator. He was married and had 1 child. He shared a harmonious marital relationship with his spouse.
This patient did not have sickle cell disease, leukemia, polycythemia, or alcoholism, had no history of drug abuse, and had not taken PDE-5 inhibitors such as sildenafil, Viagra, or anticoagulants.
After hospitalization, relevant examinations were conducted, and no abnormalities on electrocardiogram examination, laboratory tests, or imaging examination were noted. The main laboratory test results are presented in Table 1.
According to his chief concern of intermittent precordial pain and discomfort, the patient was highly suspected of having coronary artery disease. Therefore, to confirm this, coronary angiography (CAG) was performed using 4000 U heparin to avoid the complication of thrombosis and 60 mL of contrast agent. CAG revealed the following: right dominant coronary artery, LM: no abnormal conditions, LAD: 60% localized stenosis in the proximal segment of the anterior descending branch (forward blood flow (TIMI) 3 level) (Figure 1A), and LCX: 50% localized stenosis in the middle segment of the circumflex branch (forward blood flow (TIMI) 3 level) (Figure 1B). In the RCA, 50% localized stenosis was visible in the proximal segment of the right coronary artery (forward blood flow (TIMI) 3 level) (Figure 1C).
According to the CAG results, “coronary artery disease” was diagnosed (degree of stenosis >50%); however, it was not severe (<75%) enough to require intervention by implanting a stent; hence, the treatment was continued using drugs as previously described.
Twenty hours after coronary angiography, the patient reported having dysuria and penile erection with pain. On examination, priapism was suspected (Figure 2A). Actually, the patient was in this state of health for half an hour after CAG; however, he did not inform the clinician owing to shyness. When the symptoms did not abate and were accompanied by worsening of pain, the patient informed the doctor 20 h later. Initially, it was suspected to be caused by allergies to contrast agents; therefore, a 5-mg venous injection of dexamethasone was administered. Subsequently, penile examination by ultrasound indicated slow venous blood flow in the penile vein (Figure 2B).
The D-dimer level was markedly elevated at 1208 ng/mL (reference: <280 ng/mL) (Table 2). After dexamethasone injection, there was no alleviation of symptoms. Based on the patient’s symptoms and the ultrasound and D-dimer results, a thrombus in the penile vein was diagnosed, and an andrologist was invited for further diagnosis and prompt treatment. Based on the patient’s history of past illness, symptoms, and auxiliary examination results, we (a cardiologist and an andrologist) diagnosed the patient as having low-flow priapism (ischemic), penile vein thrombosis, coronary artery disease, essential hypertension (level 3), and obstructive sleep apnea syndrome.
We believe that the priapism resulted from penile vein thrombosis leading to penile vascular blood flow obstruction, which caused abnormal filling of the penile vessels with blood, resulting in priapism. Methodical aspiration and irrigation are the first-line therapies according to the AUA guidelines [7]; thus, we initially performed treatment by combining aspiration and irrigation.
We performed the treatment cooperatively with an andrologist by blood aspiration from the corpus cavernosum of the penis and drug injection to the corpus cavernosum. Approximately 120 mL of blood was withdrawn. Approximately 2 mg of hydroxylamine diluted in 20 mL of saline solution was injected at a speed of 2 mL/5 min into the corpus cavernosum of the penis. There were no obvious effects after treatment, and the penile erection hardness decreased by 1 degree (from 4 to 3).
When initial management fails, second-line therapy for priapism is a distal shunting procedure [7]. Another andrologist was consulted, and he confirmed the diagnosis of this disease and suggested that there was a need to perform a penile vein shunt to prevent severe complications such as erectile dysfunction and even penile necrosis. Therefore, we explained to the patient the complications of this disease and suggested performing a penile vein shunt; however, the patient and family members rejected this. Thus, after consulting with specialists, we continually repeated the treatment on the basis of the guidance, using blood aspiration and the injection of hydroxylamine 3 times (time/day), after which the hardness decreased to level 2.
During treatment, we used drugs for coronary artery disease, hypertension, and analgesics because the patient experienced severe pain in the penis. All drugs and methods used are presented in Table 3.
With the use of the above medications, the indicators of liver function gradually abnormally increased (Table 4). At 12 days after admission to the hospital, we suspected that abnormalities in the indicators of liver function resulted from the use of atorvastatin calcium tablets and painkiller drugs. After consulting a doctor from the Department of Liver Disease, we replaced the atorvastatin calcium tablets (20 mg po qn) with rosuvastatin calcium tablets (5 mg po qn) and used compound glycyrrhetinic acid gan tablets (75 mg po tid) to protect the liver; by these treatments, the indicators of liver function decreased gradually and normalized by hospital day 33 (Table 4).
Thus, we used rosuvastatin calcium tablets (5 mg po qn) continually and stopped using the glycyrrhetinic acid gan tablets.
After 40 days, the hardness of the penis decreased to a normal level, and the penis was not erect (Figure 3A). Ultrasound examination indicated there was very little blood flow in the veins (Figure 3B). The D-dimer levels decreased gradually (Table 2).
Discussion
Priapism is common in middle-aged people, especially after coronary angiography. Priapism is most frequently caused by sickle cell disease, leukemia, drugs (notably exogenous testosterone and psychiatric medications), increased megakaryocytes in bone marrow, JAK2V617F mutation, and thrombosis in the penile vasculature. Penile trauma and sacral parasympathetic activity can also cause spontaneous penile erections [8]. There are 2 pathophysiologic variants of priapism that are essential for distinguishing it in the emergency setting: ischemic (low-flow) and nonischemic (high-flow) priapism. Ischemic priapism is the most common subtype and accounts for more than 95% of all reported priapism episodes [9]. Epidemiologic reports suggest that the incidence rate of priapism is 0.5–1 case per 100 000 person-years [10].
Ischemic priapism is defined by rigid corpora, minimal or no cavernous nonischemic inflow, and complete occlusion of venous outflow. The result of this hematologic stasis is a progressively acidotic environment within the corpora secondary to hypoxia and hypercarbia. The progressive acidity within the closed compartment activates corporal nociceptors; hence, pain is a key factor in differentiating ischemic priapism from nonischemic priapism [11].
Nonischemic priapism, also called high-flow priapism, is much less common than ischemic priapism. This condition is the result of unregulated cavernous nonischemic inflow following the formation of an arteriolar-sinusoidal fistula [12]. In contrast to ischemic priapism, there is appropriate flow of well-oxygenated blood through the system, which maintains normal pH and oxygenation of the cavernous environment [12]. The etiology of nonischemic priapism most often involves blunt perineal trauma [12].
Thrombosis in the penile vein is the main cause of priapism, and it can cause priapism by obstructing penile venous blood flow. D-dimer is a valuable marker for the diagnosis of thrombi. D-dimer is a soluble fibrin degradation product resulting from the breakdown of thrombi by the fibrinolytic system [13]. Many studies have indicated that D-dimer is a valuable marker of fibrinolysis activation. As a result, D-dimer has been widely used for diagnosis of venous thromboembolism (VTE) [14]. Among patients with VTE, D-dimer levels vary with clot burden, timing of measurement, and initiation of treatment [15].
A combined analysis of the characteristics of this patient revealed that the ultrasound test of the penis indicated slow venous blood flow and the blood level of D-dimer was high; thus, a thrombus in the penile vein was confirmed.
We further sought to determine the cause of a thrombus in the penile vein after CAG. During CAG, the angiography catheter, guidewire, and contrast medium contacted the blood and vascular wall. Solomon and colleagues [16] have shown that platelet deposition can vary 12-fold depending on the catheter material and whether heparin bonding is used.
One study reported that [17] the clotting system is activated by various intravascular catheters. When foreign objects such as catheters enter the bloodstream, they activate the clotting and anticoagulation systems. Numerous studies [14] have indicated that D-dimer is as a valuable marker for activation of coagulation and fibrinolysis systems. In this case report, we explored the correlation between coronary angiography and priapism. First, CAG was performed by entering a guide catheter, guidewire, and contrast agent into the body and activating the coagulation system. Second, the patient had a history of hypertension and OSAS. Both are risk factors for a hypercoagulable state; thus, the probability of thrombosis in body vessels is greater when CAG is performed. During CAG, we regularly use heparin (4000 IU) to prevent thrombosis in body vessels. Most likely because of individual differences, this patient was resistant to heparin. Thus, heparin (4000 IU), injected at the beginning of the operation, does not have an anticoagulation effect; thus, there is an overly formed thromboembolism. The fibrinolytic system overly dissolves the thrombus and results in elevated blood D-dimer levels.
As a result of excessive thromboembolism, there is a micro-thrombus in the bloodstream. It is likely embolized in the penile vein, causing obstruction of penile vein blood flow and resulting in priapism.
Heparin resistance (HR) is defined as the inability of an adequate heparin dose to increase activated clotting time (ACT) to an acceptable level [18]. The anticoagulant effect of heparin is produced by binding antithrombin (AT) to a specific pentasaccharide sequence on the heparin molecule, after which the thrombin inhibitory potency of AT can increase by over 2000-fold [19]. As a result, AT deficiency is regarded as the primary mechanism of HR [20]. In our case, the patient was informed of an urgent need to confirm whether he had HR and to guide him regarding precision therapy; however, the patient and family members did not agree to test the ACT after receiving an adequate dosage of heparin or drawing venous blood to test the concentration or activity of AT; therefore, we suspected that this patient might have had HR, which resulted from AT deficiency. This suspicion needs confirmation when clinicians encounter similar cases.
The symptoms of priapism and pain in the penis returned to normal; however, we did not test the erectile function of the penis, so the patient should be followed-up in the future to evaluate erectile function.
Conclusions
This report has highlighted that priapism is becoming more common in middle-aged men, and should be treated as a medical emergency according to current management guidelines, and that the underlying cause should be identified to prevent recurrence.
Figures
References:
1.. Timmis A, Vardas P, Townsend N, European Society of Cardiology: Cardiovascular disease statistics 2021: Eur Heart J, 2022; 43(8); 716-99
2.. Miller JM, Rochitte CE, Dewey M, Diagnostic performance of coronary angiography by 64-row CT: N Engl J Med, 2008; 359(22); 2324-36
3.. Tavakol M, Ashraf S, Brener SJ, Risks and complications of coronary angiography: A comprehensive review: Glob J Health Sci, 2011; 4(1); 65-93
4.. Cosby RS, Giddings JA, See JR, Complications of coronary arteriography: Am Heart J, 1975; 89(2); 259-60
5.. Nagathan DS, Pahwa HS, Kumar A, Goel A, Anticoagulant-induced priapism progressing to penile gangrene: A devastating complication!: BMJ Case Rep., 2012; 2012(1) bcr2012007073
6.. Eland IA, van der Lei J, Stricker BHC, Sturkenboom MJCM, Incidence of priapism in the general population.: Urology, 2001; 57(5); 970-72
7.. Ericson C, Baird B, Broderick GA, Management of priapism: Urol Clin North Am, 2021; 48(4); 565-76
8.. Jesus LEd, Teixeira L, Bertelli A, Recurring priapism may be a symptom of voiding dysfunction – case report and literature review: Int Braz J Urol, 2016; 42(2); 389-91
9.. Broderick GA, Kadioglu A, Bivalacqua TJ, Priapism: Pathogenesis, epidemiology, and management: J Sex Med, 2010; 7(1 Pt 2); 476-500
10.. Brahmer J, Lacchetti C, Schneider B, Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology clinical practice guideline, 2018; 36(17); 1714-68
11.. Muneer A, Ralph D, Guideline of guidelines: Priapism: BJU Int, 2017; 119(2); 204-8
12.. Ericson C, Baird B, Broderick GA, Management of priapism: 2021 update: Urol Clin North Am, 2021; 48(4); 565-76
13.. Eljilany I, Elzouki A-N, D-dimer, fibrinogen, and IL-6 in COVID-19 patients with suspected venous thromboembolism: A narrative review: Vascular Health Risk Manag, 2020; 16; 455-62
14.. Weitz JI, Fredenburgh JC, Eikelboom JW, A Test in context: D-dimer: J Am Coll Cardiol, 2017; 70(19); 2411-20
15.. Linkins LA, Takach Lapner S, Review of D-dimer testing: Good, bad, and ugly: Int J Lab Hematol, 2017; 39; 98-103
16.. Solomon DD, Arnold WL, Martin ND, Lentz DJ, An in vivo method for the evaluation of catheter thrombogenicity: J Biomed Mater Res, 1987; 21(1); 43-57
17.. Monteiro A, Burke SM, Baig AA, A systematic review and meta-analysis of the Derivo Embolization Device: A novel surface-modified flow diverter for intracranial aneurysm treatment: J Neurointerv Surg, 2022; 14(11); 1125-29
18.. Finley A, Greenberg C, Heparin sensitivity and resistance: Anesth Analg, 2013; 116(6); 1210-22
19.. Bleich HL, Boro ES, Rosenberg RD, Actions and Interactions of Antithrombin and Heparin: N Engl J Med, 1975; 292(3); 146-51
20.. Spiess BD, Treating heparin resistance with antithrombin or fresh frozen plasma: Ann Thorac Surg, 2008; 85(6); 2153-60
Figures
Tables
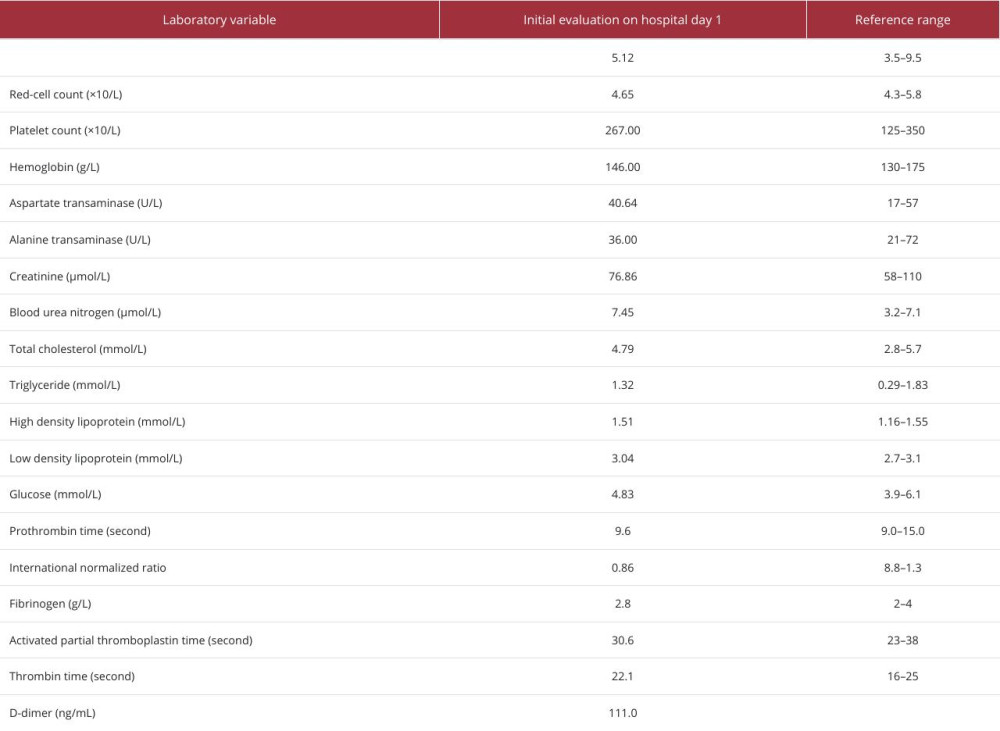 Table 1.. Laboratory data.
Table 1.. Laboratory data.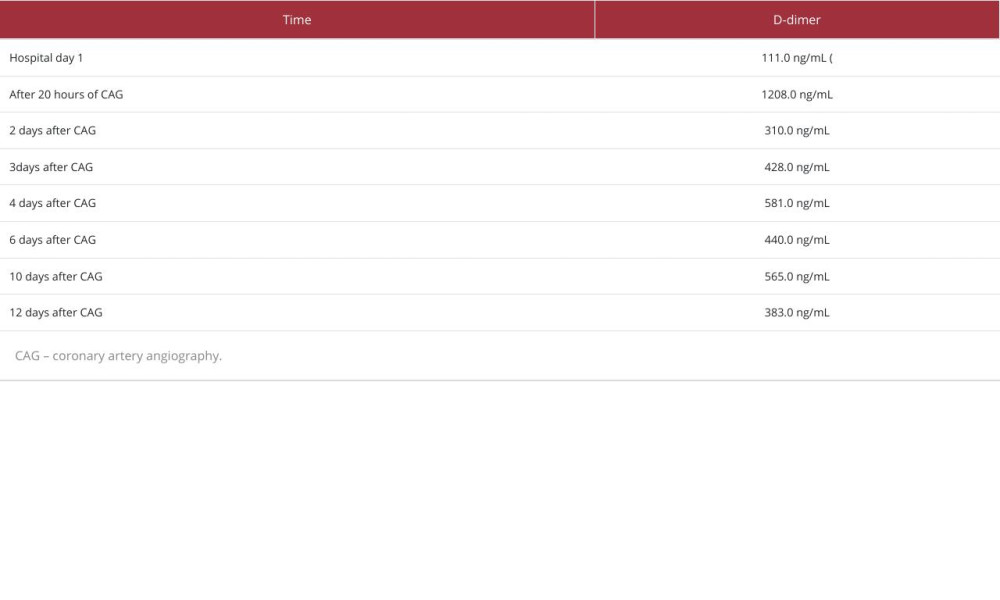 Table 2.. Blood D-dimer level during hospitalization.
Table 2.. Blood D-dimer level during hospitalization.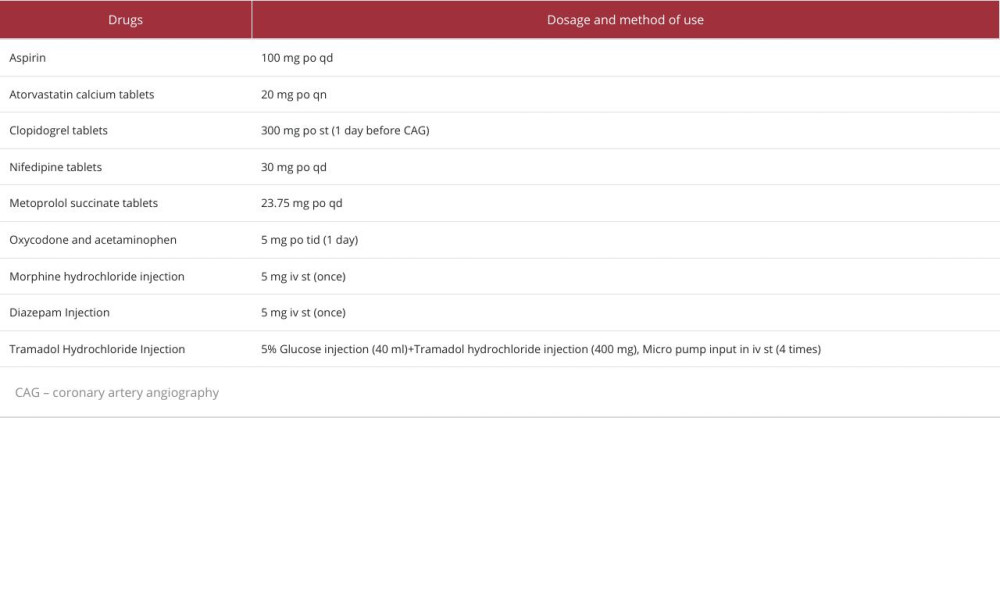 Table 3.. Drugs and methods of use.
Table 3.. Drugs and methods of use.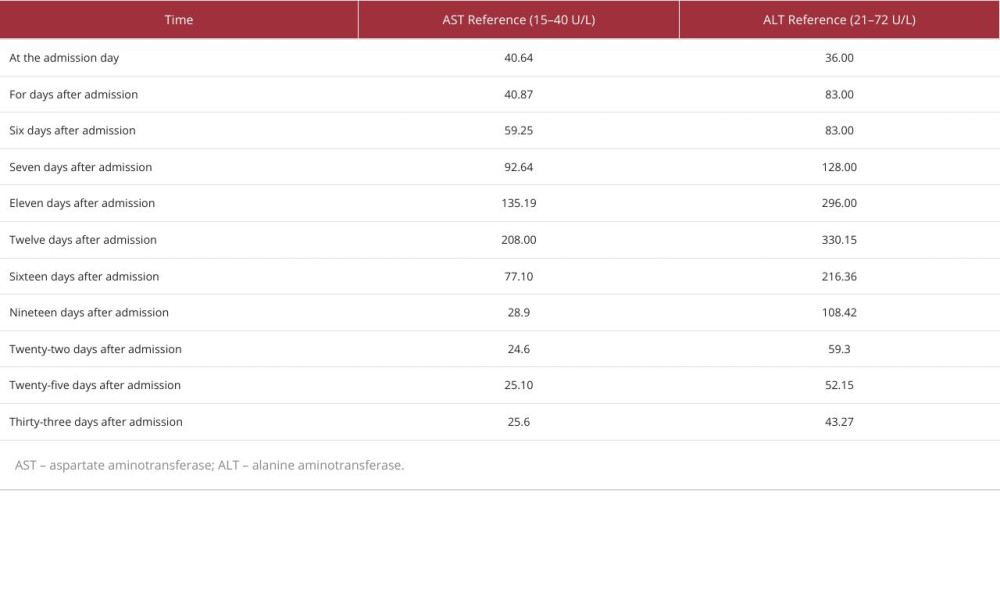 Table 4.. Indicators of liver function during treatment.Table 1.. Laboratory data.Table 2.. Blood D-dimer level during hospitalization.Table 3.. Drugs and methods of use.Table 4.. Indicators of liver function during treatment.
Table 4.. Indicators of liver function during treatment.Table 1.. Laboratory data.Table 2.. Blood D-dimer level during hospitalization.Table 3.. Drugs and methods of use.Table 4.. Indicators of liver function during treatment. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133