08 July 2024: Articles 
Effective Management of Severe Amlodipine/Atenolol Overdose with Intravenous Calcium, Hyperinsulinemic Euglycemia Therapy, and Continuous Veno-Venous Hemodialysis: A Case Report
Unusual clinical course, Challenging differential diagnosis, Management of emergency care, Adverse events of drug therapy
Cong Tan Nguyen12ACEF, Van Cuong Bui12ABC, Ngoc Son Do12AF, Thi Huong Giang BuiDOI: 10.12659/AJCR.943777
Am J Case Rep 2024; 25:e943777






Abstract
BACKGROUND: Amlodipine, a calcium channel blocker, and atenolol, a beta blocker, are commonly used as a fixed drug combination (FDC) to treat hypertension. Intentional or non-intentional overdose of amlodipine-atenolol results in hypotension and myocardial depression with a high risk of mortality. This report describes a 64-year-old man with an overdose of amlodipine-atenolol, presenting as an emergency with hypotension, bradycardia, and severe metabolic acidosis. He was successfully treated with intravenous calcium chloride infusion, hyperinsulinemia euglycemia therapy (HIE), and continuous veno-venous hemodialysis (CVVHD).
CASE REPORT: A 64-year-old man was diagnosed with essential hypertension 1 week prior to the admission. He had been prescribed 1 FDC tablet of amlodipine and atenolol (5+50 mg) per day; however, he took 1 table of the FDC per day for 3 days and then took 3-4 tablets each day during the next 4 days. He was brought to the hospital with hypotension, bradycardia, and severe metabolic acidosis and was diagnosed with amlodipine-atenolol overdose. He was treated with intravenous calcium chloride infusion, HIE, and CVVHD. His hemodynamics started to improve after administering these therapies for 6 h. Inotropes were gradually tapered off and stopped. He was extubated on day 5 and recovered completely.
CONCLUSIONS: This report shows the serious effects amlodipine-atenolol overdose and the challenges of emergency patient management. An overdose of FDC of amlodipine and atenolol can cause cardiovascular collapse and severe metabolic acidosis. Timely and aggressive management with intravenous calcium infusion, HIE, and CVVHD is essential.
Keywords: Drug Overdose, Continuous Renal Replacement Therapy, Toxicology, Resuscitation, cardiotoxicity, Humans, Male, Amlodipine, Middle Aged, atenolol, Calcium Channel Blockers, Infusions, Intravenous, Calcium Chloride, Antihypertensive Agents, Drug Combinations
Introduction
Calcium channel blockers (CCBs) and β-blockers (BBs) account for roughly 40% of cardiovascular drug exposures reported to Poison Centers. These drugs account for more than 65% of deaths from cardiovascular drug overdose [1]. Amlodipine is a dihydropyridine, which is 1 of 2 groups of CCBs. It inhibits the alpha-1 subunit of L-type voltage-gated calcium channels, preventing intracellular calcium influx and decreasing myocar-dial and vascular contraction [2]. It has a therapeutic dose of 2.5–10 mg/day with a slow onset (6–12 h) and long half-life (30–50 h) [1,2]. Atenolol is a β1-receptor selective antagonist with a recommended dose of 25–100 mg daily, decreasing intracellular cAMP and reducing calcium flow through L-type channels [1]. As a result, amlodipine and atenolol have a synergic effect on vasodilation and reducing cardiac muscle contractility. Thus, overdose of amlodipine-atenolol is associated with high mortality.
CCBs and BBs toxicity manifest a host of symptoms. Patients with CCBs and BBs intoxication may be asymptomatic or progress to cardiovascular collapse [1]. CCBs have a great affinity to specific tissues – myocardial, vascular, gastrointestinal muscle, and pancreas – leading to hypotension, bradycardia, hyperglycemia, and renal insufficiency [1]. BBs toxicity induces bradycardia, hypotension, seizures, hypoglycemia, hypokalemia, hypocalcemia, and bronchospasm [1].
A multimodal approach should be used to treat CCBs and BBs overdose. Gastrointestinal decontamination can be effective if the patient is brought to the hospital early. Hyperinsulinemic euglycemic therapy, intravenous calcium, and inotropes infusions are standard treatments, as these medications improve myocardial contractility and heart rate. Glucagon and phosphodiesterase infusions also provide moderate hemodynamic improvement [3]. Hemodialysis can help filter out some CCBs and BBs, depending on their pharmacological properties [4,5]. In refractory cardiogenic shock, extracorporeal membrane oxygenation (ECMO) can help maintain the patient’s hemodynamics [3,6].
To date, few overdose cases of FDC of amlodipine and atenolol have been reported worldwide. This report describes a 64-year-old man with essential hypertension and an overdose of amlodipine-atenolol, presenting as an emergency with hypotension, bradycardia, and metabolic acidosis, treated with intravenous calcium chloride infusion, HIE, and CVVHD.
Case Report
A 64-year-old man with essential hypertension diagnosed 7 days prior to admission was brought to the provincial hospital by his wife due to fatigue and dyspnea. In the first 3 days after diagnosis, he took 1 FDC tablet of amlodipine and atenolol (5+50 mg) per day. However, in the next 4 days, he took 3-4 FDC tablets per day due to his concerns about his blood pressure fluctuation after measuring each time. On day 7, he felt extremely fatigued. Thus, he was brought to the provincial hospital with a heart rate of 45 beats per minute and blood pressure of 60/35 mmHg. He was started on inotropes and transferred to our hospital. On admission, his body temperature was 36.8ºC and he appeared agitated. He was on epinephrine (0.6 µg/kg/min), norepinephrine (0.4 µg/kg/min), and dobutamine (15 µg/kg/min). His blood pressure (BP) was 75/45 mmHg and heart rate (HR) was 45 beats per minute with regular S1, S2. No murmur was noted. His respiratory rate was 30, and peripheral oxygen saturation was 95% while he was breathing via a non-re-breather mask; the vesicular sound was clear with bibasilar wet crackles. The abdominal exam was unremarkable. His wife stated that he had no fever or chest pain and took no herbal medicine or drugs except for FDC tablets of amlodipine and atenolol.
Complete blood count (CBC) showed a mild increase in white blood cells (13.2 G/L), while procalcitonin was below the normal limit, and urine analysis and culture, as well as blood and sputum cultures, were done, but the test results were negative. Furthermore, a chest radiograph showed pulmonary edema (Figure 1), while an abdominal ultrasound showed no source of infection or bleeding. We also screened for frequently encountered toxins that might induce hypotension and metabolic acidosis, including organophosphorus, methanol, and phenformin, but the results were negative. Echocardiography, electrocardiography (ECG), and troponin T were assessed. Echocardiography demonstrated a mild ejection fraction (EF) decrease with EF of 50% and no regional wall motion abnormalities. ECG showed sinus bradycardia with junctional escape beats (Figure 2). Troponin T was 0.039 ng/mL, which was below normal limits. NT-pro BNP was increased significantly (685 pg/mL). Extended chemical panel and arterial blood gas (ABG) analysis suggested acute kidney injury (urea 25 mmol/L, creatinine 452 µmol/L) and severe acidosis (pH 7.16, HCO3 6 mmol/L, lactate 13.4 mmol/L) (Table 1).
We suspected the patient’s condition was caused by an amlodipine-atenolol overdose, which led to bradycardia, vasodilation, and myocardial contractility impairment. These mechanisms induced severe hypotension and then metabolic acidosis. Since we could not measure the concentration of amlodipine and atenolol in our laboratory, we consulted a toxicologist and a cardiologist and started treating the patient for an amlodipine-atenolol overdose. Upon admission, the patient was intubated and sedated. One liter of normal saline was immediately administered to expand the intravascular volume. Intravenous calcium and insulin were given simultaneously. We administered 1 g of calcium given as a bolus dose, followed by continuous intravenous infusion of 1 g per hour. Insulin was also given with a loading dose of 0.5 UI/kg and then a continuous infusion of 0.5 UI/kg/h. We also utilized CVVHD to correct the patient’s metabolic acidosis and help filter out atenolol. Since we expected his hemodynamics and heart rate would improve soon after initiating HIE and intravenous calcium infusion, we did not perform transvenous or transcutaneous pacing.
Six hours after starting the treatment protocol, the patient’s hemodynamics and acidosis improved. We were able to reduce the inotropes’ infusion rates from 1 µg/kg/min for both epinephrine and norepinephrine (at the 12th hour) to just 0.1 µg/kg/min (at the 21st hour). We also halved the dobutamine infusion rate at the end of the first day (Table 2). On day 2, a chest radiograph illustrated improvement of the pulmonary edema (Figure 3), and the patient returned to sinus rhythm (Figure 4). The propofol, insulin, and calcium were continued until day 3, and CVVHD was stopped on day 4. Moreover, epinephrine and norepinephrine were discontinued on day 2, and dobutamine was withdrawn on day 4 (Table 3). The patient was extubated on day 5. His renal function had gradually improved. On day 7, urine output was 1670 mL/24 h without diuretics (blood creatine of 200 µmol/L), while heart rate was 70 beats per minute, BP was 140/80 mmHg, and he was transferred to a local hospital. His renal function completely recovered in the next 2 weeks, and he was discharged from that hospital and was prescribed telmisartan 40 mg per day for hypertension.
Discussion
An amlodipine-atenolol overdose is a life-threatening condition that is challenging for physicians to manage. A multi-modality approach, including intravenous calcium chloride infusion, HIE, and CVVHD, should be utilized to treat this overdose.
While previously reported cases involved massive intoxication due to psychiatric problems and suicide attempts, the present case is unique because the patient took just 2 times the therapeutic dose of amlodipine and atenolol (20 mg of amlodipine and 200 mg of atenolol) for 4 consecutive days [7,8], suggesting the low threshold for FDC of amlodipine-atenolol toxicity.
In all CCBs/BBs overdose cases, a resuscitation protocol must be employed immediately to ensure patient airway, breathing, and circulation. Because of mental status changes, ranging from comatose to agitated, intubation should be considered to protect the airway. Oxygen should be supplied in case of low blood oxygenation. In hypotensive patients, intravenous crystalloid bolus, inotropes, and vasopressors should be given to restore hemodynamics [1,2,9,10]. Our patient presented with agitation, hypotension, and shock; thus, we immediately intubated him and then gave him 1 L of normal saline bolus and increased inotropes and vasopressors’ infusion rates to improve hemodynamic parameters. In addition, gastrointestinal decontamination can be considered for CCBs and BBs intoxication, administered 1–2 h before admission, hemodynamically stable, neurologically intact, and low risk of aspiration [2,11]. We did not perform gastrointestinal decontamination in our case because of the time at which the amlodipine/atenolol was taken and the patient’s agitation.
Medications that counter the effect of CCBs and BBs on myocardial and vascular muscle should be promptly given to treat CCBs/BBs overdose. Inotropes and vasopressors can help increase myocardial contractility and vasoconstriction. Intravenous calcium infusion increases blood pressure by augmenting cardiac output or increasing systemic vascular resistance [1,2,12,13]. Administration of calcium increases extracellular calcium concentration, allowing calcium influx via the remaining unblocked L-type calcium channels [2]. Calcium chloride is the preferred choice, with initial bolus administration of 10–20 mL (1–2 g), then repeat boluses or infused continuously [2,12,13]. Our hospital has used the protocol with an initial bolus dose of 10 mL calcium chloride followed by continuous infusion to keep serum ionized calcium levels above 2 mEq/L. A high insulin infusion dose is another adjuvant therapy, known as hyperinsulinemic euglycemia (HIE) [1,2,9,14–16]. CCBs and BBs overdose influence myocardial metabolism, shifting from fatty acids to glucose utilization [17]. However, hypoinsulinemia and insulin resistance from CCBs and BBs overdose make myocardial cells unable to freely utilize glucose for energy. Thus, high-dose insulin therapy allows myocardial cells to use glucose as energy [3]. In addition, insulin has direct and concentration-dependent inotropic effects on myocardial cells [18]. Both these mechanisms provide a sound theoretical rationale for using HIE. There are several insulin dosing regimens for HIE, ranging from 0.1 to 1 UI/kg bolus, followed by 0.5–1 UI/kg/h continuous infusion [14]. Because insulin also increases other tissues’ glucose uptake, which can cause hypoglycemia, intravenous glucose infusion is required to prevent this. Our center has utilized the HIE protocol with an insulin bolus dose of 0.5 UI/kg followed by 0.5 UI/kg/h continuous infusion and 10% dextrose simultaneously being given to keep blood glucose above 10 mmol/L. In a similar case, Tale et al also used HIE to treat a patient with FDC of amlodipine-atenolol overdose [7]. Glucagon and phosphodiesterase inhibitors are also advocated for CCBs and BBs, as both drugs have inotropic and chronotropic cardiac effects, activating adenylate cyclase unaffected by beta-receptor blockade [1]. However, due to the lack of availability in our center, we could not use them for our patient.
Atropine can be considered if the patient has bradycardia. Given that our patient was already on epinephrine, norepinephrine, and dobutamine, we did not administer intravenous atropine. Intravenous lipid emulsion (ILE) has been used to treat CCBs/BBs poisoning reported in a few cases worldwide [19]. However, due to a lack of literature and convincing rationale for using ILE, we decided not to utilize ILE for our patient.
Extracorporeal treatment (ECTR) is a controversial adjunctive therapy for treating CCBs and BBs poisoning. Because of the heterogeneous pharmacological properties of these drugs, they should be considered on a case-by-case basis. ECTRs have been developing for the past several decades; thus, the efficacy of this therapy on CCBs and BBs overdose has been a subject of review. In recent studies, ECTRs have been recommended for some cases of CCBs and BBs poisoning [4,5]. ECTRs were recommended for atenolol and sotalol poisoning with kidney impairment but not for amlodipine poisoning. Of note, use of atenolol clearance by ERTCs has tripled in the past 30 years [5]. Rao et al used ERTC with sustained low-efficiency dialysis (SLED) in treating a similar case and found it effective [8]. We performed CVVHD but not SLED for our patient, as CVVHD helps filter out atenolol and also helps correct metabolic acidosis.
Extracorporeal membrane oxygenation (ECMO) has been increasingly used for cardiogenic shock, including from CCBs and BBs intoxication. Veno-arterial ECMO helps augment cardiac output, maintaining adequate blood flow to vital organs. It can be considered as a last resort and has been used successfully in several cases of life-threatening cardiovascular toxicity [6,20,21].
Conclusions
An overdose of FDC of amlodipine-atenolol is potentially lethal as it can cause cardiovascular collapse and severe metabolic acidosis. Although its management presents challenges to physicians, prompt treatment with intravenous calcium infusion, HIE, and CVVHD can help successfully treat this overdose.
References:
1.. DeWitt CR, Waksman JC, Pharmacology, pathophysiology and management of calcium channel blocker and beta-blocker toxicity: Toxicol Rev, 2004; 23(4); 223-38
2.. Alshaya OA, Alhamed A, Althewaibi S, Calcium channel blocker toxicity: A practical approach: J Multidiscip Healthc, 2022; 15; 1851-62
3.. Graudins A, Lee HM, Druda D, Calcium channel antagonist and beta-blocker overdose: Antidotes and adjunct therapies: Br J Clin Pharmacol, 2016; 81(3); 453-61
4.. Wong A, Hoffman RS, Walsh SJ, Extracorporeal treatment for calcium channel blocker poisoning: Systematic review and recommendations from the EXTRIP workgroup: Clin Toxicol Phila Pa, 2021; 59(5); 361-75
5.. Bouchard J, Shepherd G, Hoffman RS, Extracorporeal treatment for poisoning to beta-adrenergic antagonists: Systematic review and recommendations from the EXTRIP workgroup: Crit Care, 2021; 25(1); 201
6.. Vignesh C, Kumar M, Venkataraman R, Extracorporeal membrane oxygenation in drug overdose: A clinical case series: Indian J Crit Care Med, 2018; 22(2); 111-15
7.. Tale S, Kumar M, Ghosh S, Bhalla A, A case of life-threatening amlodipine and atenolol overdose: Indian J Crit Care Med, 2019; 23(6); 281-83
8.. Rao NK, Jayaprakash B, Patil N, Amlodipine-atenolol overdose management: A physician’s nightmare: J Appl Pharm Sci, 2016; 6(1); 153-55
9.. Newton CRH, Delgado JH, Gomez HF, Calcium and beta receptor antagonist overdose: A review and update of pharmacological principles and management: Semin Respir Crit Care Med, 2002; 23(1); 19-25
10.. Lauterbach M, Clinical toxicology of beta-blocker overdose in adults: Basic Clin Pharmacol Toxicol, 2019; 125(2); 178-86
11.. Khalid MM, Galuska MA, Hamilton RJ, Beta-blocker toxicity: StatPearls, 2023, StatPearls Publishing Accessed November 28, 2023. http://www.ncbi.nlm.nih.gov/books/NBK448097/
12.. Lam YM, Tse HF, Lau CP, Continuous calcium chloride infusion for massive nifedipine overdose: Chest, 2001; 119(4); 1280-82
13.. Koch AR, Vogelaers DP, Decruyenaere JM, Fatal intoxication with amlodipine: J Toxicol Clin Toxicol, 1995; 33(3); 253-56
14.. Krenz JR, Kaakeh Y, An overview of hyperinsulinemic-euglycemic therapy in calcium channel blocker and β-blocker overdose: Pharmacotherapy, 2018; 38(11); 1130-42
15.. Shepherd G, Klein-Schwartz W, High-dose insulin therapy for calcium-channel blocker overdose: Ann Pharmacother, 2005; 39(5); 923-30
16.. Yuan TH, Kerns WP, Tomaszewski CA, Insulin-glucose as adjunctive therapy for severe calcium channel antagonist poisoning: J Toxicol Clin Toxicol, 1999; 37(4); 463-74
17.. Hantson P, Beauloye C, Myocardial metabolism in toxin-induced heart failure and therapeutic implications: Clin Toxicol Phila Pa, 2012; 50(3); 166-71
18.. von Lewinski D, Bruns S, Walther S, Insulin causes [Ca2+]i-dependent and [Ca2+]i-independent positive inotropic effects in failing human myocardium: Circulation, 2005; 111(20); 2588-95
19.. Meaney CJ, Sareh H, Hayes BD, Gonzales JP, Intravenous lipid emulsion in the management of amlodipine overdose: Hosp Pharm, 2013; 48(10); 848-54
20.. Voicu S, M’Rad A, Malissin I, Deye N, Mégarbane B, Extracorporeal life support in cardiotoxicant poisoning – a narrative review: Basic Clin Pharmacol Toxicol, 2023; 132(1); 5-20
21.. Rona R, Cortinovis B, Marcolin R, Extra-corporeal life support for near-fatal multi-drug intoxication: A case report: J Med Case Reports, 2011; 5; 231
Figures
Tables
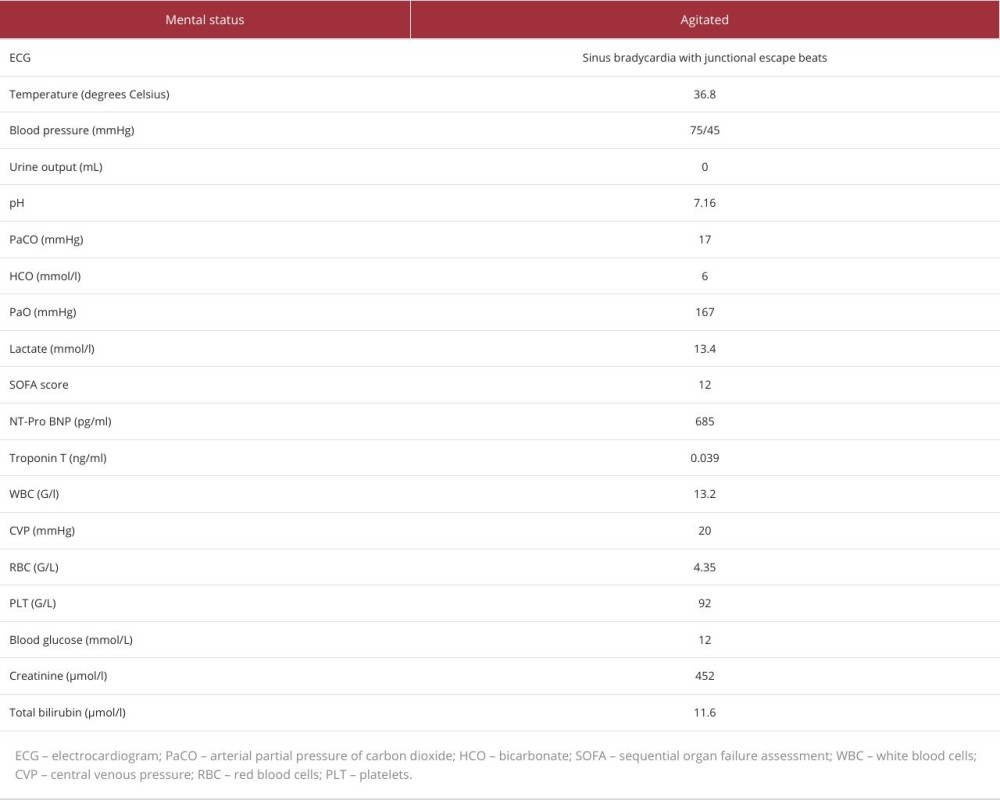 Table 1.. Characteristics of the patient on admission.
Table 1.. Characteristics of the patient on admission.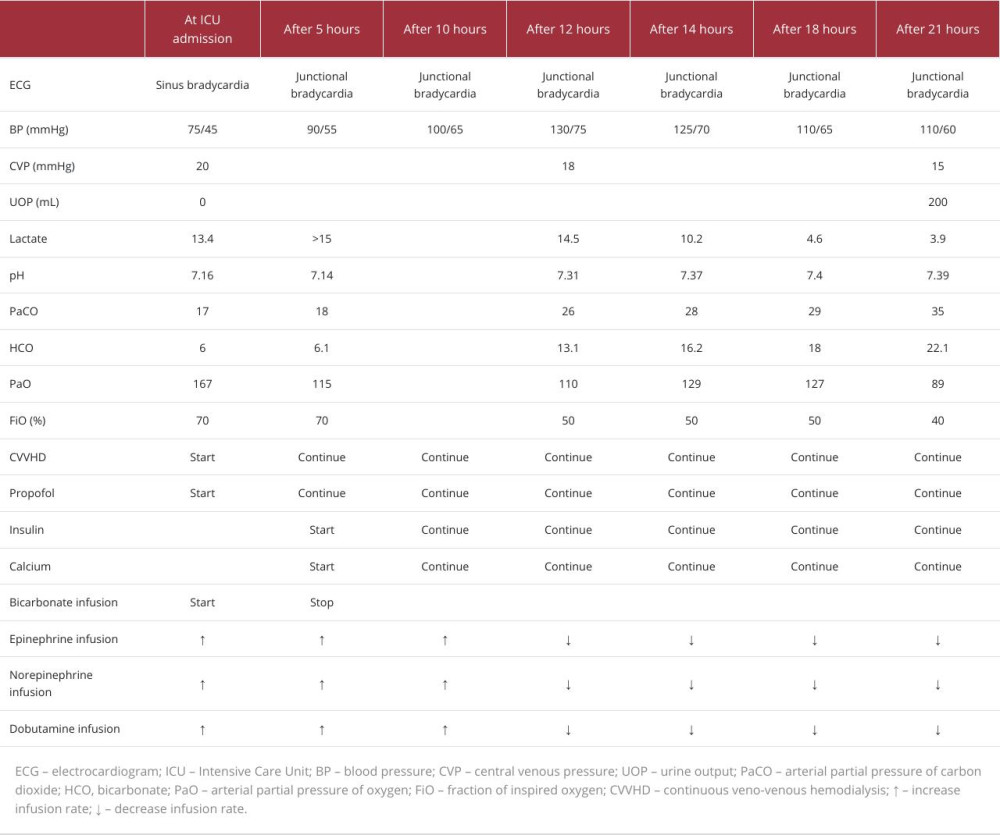 Table 2.. The clinical course of the patient during treatment on day 1.
Table 2.. The clinical course of the patient during treatment on day 1.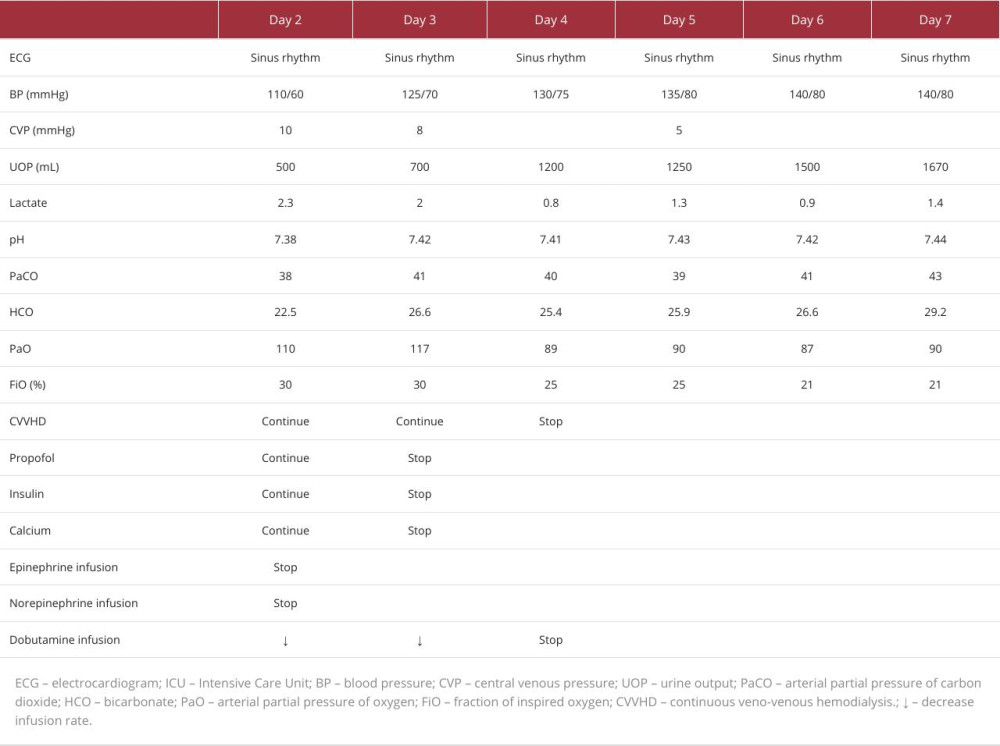 Table 3.. The clinical course of the patient from day 2 to day 7.Table 1.. Characteristics of the patient on admission.Table 2.. The clinical course of the patient during treatment on day 1.Table 3.. The clinical course of the patient from day 2 to day 7.
Table 3.. The clinical course of the patient from day 2 to day 7.Table 1.. Characteristics of the patient on admission.Table 2.. The clinical course of the patient during treatment on day 1.Table 3.. The clinical course of the patient from day 2 to day 7. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133