27 June 2024: Articles ")
Spinal Dural Arteriovenous Fistula with Low Back Pain as the Only Symptom at Onset: A Case Report
Unknown etiology, Mistake in diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Adverse events of drug therapy
Hui Ouyang1ABCDEF, Shuo Zhang1BDE, Fei Xu1BDF, Wenjing Lin2BC, Zunjing Liu3ADG*, Huailian Guo34ACEFDOI: 10.12659/AJCR.943947
Am J Case Rep 2024; 25:e943947






Abstract
BACKGROUND: Spinal cord arteriovenous fistula that only manifests as lower back pain is easily misdiagnosed as myofasciitis, lumbar spondylosis, and other diseases, and incorrect treatment such as glucocorticoid blockade might be given, leading to worsening of the condition.
CASE REPORT: We analyze the clinical characteristics of a patient with spinal dural arteriovenous fistula who presented with chronic-onset low back pain. A patient with spinal dural arteriovenous fistula presented with chronic-onset low back pain as the only symptom, and was misdiagnosed as having myofasciitis. We assessed the paraclinical data, clinical reasoning, and course of treatment. The patient was an elderly man with low back pain for 1 year. He was diagnosed with myofasciitis in a local hospital and received local blocking treatment using glucocorticoid, and left lower-limb weakness appeared after that. After he was admitted to our hospital, enhanced thoracic and lumbar magnetic resonance imaging and selective spinal angiography were performed, and the results indicated the diagnosis of spinal dural arteriovenous fistula. After surgical treatment, the low back pain and lower-limb weakness were alleviated, and the patient is still under follow-up.
CONCLUSIONS: The possibility of spinal dural arteriovenous fistula should not be overlooked among patients with chronic low back pain, and caution should be taken when using glucocorticoids for treatment of chronic low back pain.
Keywords: Back Pain, chronic pain, Spinal Cord, Spinal Cord Vascular Diseases, Humans, Male, Low Back Pain, Central Nervous System Vascular Malformations, Aged, Magnetic Resonance Imaging, Diagnosis, Differential
Introduction
Chronic low back pain, which affects nearly 1/3 of the population, is one of the main reasons for the loss of labor capacity worldwide and has become a serious medical and social problem [1]. Chronic low back pain affects the quality of life of patients, increases the incidence rate of emotional disorders such as depression and anxiety, and creates a huge burden on families and society [2]. The common causes of chronic low back pain include lumbar disc herniation, lumbar spinal stenosis, and back myofasciitis. The main treatment methods for chronic low back pain currently include physical therapy, drug therapy, cognitive behavioral therapy, and interventional therapy. Local blocking is also commonly used in clinical practice for the treatment of chronic low back pain.
However, in addition to the common diseases that cause chronic low back pain listed above, rare causes can also lead to chronic low back pain. Finding the rare causes of chronic low back pain is a relatively difficult part of clinical diagnosis and treatment. At the same time, missed diagnosis and misdiagnosis of rare diseases may lead to incorrect treatment planning for chronic low back pain. In 2023, the Department of Neurology at Peking University People’s Hospital admitted a patient with chronic low back pain as the main concern, who was transferred from Hebei province. During the diagnosis and treatment process, the etiology of the patient was analyzed, the diagnosis and treatment plan were repeatedly revised, and the cause of chronic low back pain was ultimately determined and the patient was cured. This case was relatively rare and diagnosis and treatment was complex. By analyzing clinical data and exploring the causes, we aim to improve clinical diagnosis.
Case Report
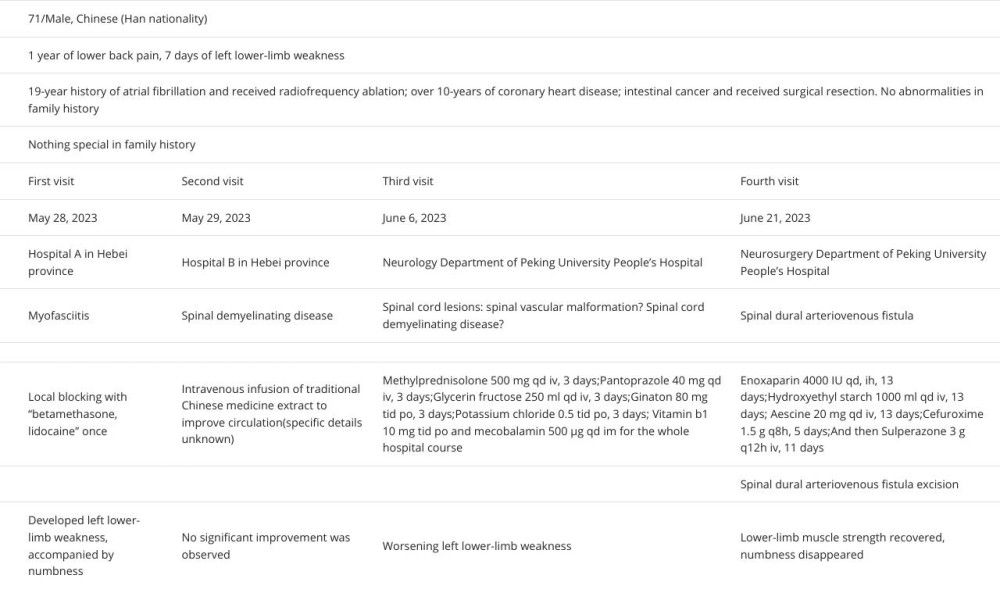
A 71-year-old man presented with 1 year of low back pain. He had lower back pain in May 2022, without obvious causes. The pain was persistent and dull, and was not related to posture changes. The visual analog scale (VAS) score for pain was 2, the patient did not seek medical care.
At the beginning of May 2023, the patient realized that his lower back pain had worsened, and the VAS score was 7. When he sought medical care from a local hospital, he was diagnosed with “myofasciitis” and received local blocking treatment. The medications used for local blocking were “betamethasone, lidocaine”, but there was no significant relief in the pain after injection. About half a day later, he developed left lower-limb weakness and had difficulty standing on his own.
He then sought medical attention at another local hospital, where thoracic and lumbar spine enhanced magnetic resonance imaging showed slight thickening of the thoracic spinal cord at T7-T12 level, with mild enhancement of lesions. The local hospital diagnosed him with spinal demyelinating disease. However, no significant improvement was observed in the patient’s low back pain and limb weakness after treatment.
One week later, the patient came to our hospital for treatment. Neurological physical examination showed left lower-limb muscle strength grade 4, and right lower-limb muscle strength was normal. Pain and touch sensation were reduced in the left inguinal area and left buttocks, there were a left Babinski sign and Chaddock sign (+), and no other abnormalities were found on neurological physical examination. The reexamination of enhanced thoracic MRI scan (Figure 1) showed abnormal signals in the medulla spinalis at the T7-T12 level. The re-examination of enhanced MR imaging of the lumbar spine found tortuous blood vessels in the vertebral canal, and point-like enhancement lesions in the posterior spinal cord at the T11 level. This characteristic imaging suggested spinal vascular malformation or arteriovenous fistula. Cerebrospinal fluid biochemistry testing showed total protein 0.56 g/L, and a routine examination and virus antibody test of cerebrospinal fluid showed no significant abnormalities. Cerebrospinal fluid anti-AQP4, anti-MOG antibody and oligoclonal band (OB) were negative. The admitting diagnosis was spinal cord lesions, with possible spinal vascular malformation or spinal cord demyelinating disease. However, no fistula was found after selective spinal cord angiography.
Considering the possibility of spinal cord demyelinating disease, he was given methylprednisolone 500 mg qd for diagnostic treatment of suspected demyelinating disease. Early the next day, he had worsening left lower-limb weakness and difficulty standing, with left lower-limb muscle strength grade 3 and right lower-limb muscle strength grade 4. One day later, he had worsening left lower-limb weakness and was unable to stand up. The left lower-limb muscle strength was grade 3, so methylprednisolone was immediately discontinued. Considering the possibility of spinal vascular disease, we performed super-selective whole-brain and spinal angiography (Figure 2), showing spinal dural arteriovenous fistula (on the right side, at the 12th thoracic level).
The patient was subsequently transferred to the neurosurgery department for spinal dural arteriovenous fistula excision. After opening the dura mater during the surgery, an abnormally thick and tortuous arterial drainage vein was seen draining from the right T12 nerve root into the dura mater to the surface of the spinal cord, which was electro-coagulated and cut off. On the 5th day after surgery, the patient’s lower-limb muscle strength recovered completely, symptoms of numbness disappeared, vibratory and pain sensation returned to normal, and pathological signs disappeared. At the same time, the degree of back pain was reduced, indicating a satisfactory therapeutic effect (Table 1).
Discussion
The patient had experienced chronic pain in the lower back for over a year, during which he visited several hospitals and was diagnosed as myofasciitis and myelitis. He was treated with glucocorticoids, which worsened his condition. Finally, he was diagnosed with spinal dural arteriovenous fistula, which is an uncommon cause of low back pain in clinical practice, as its clinical symptoms are not specific and it can be misdiagnosed as intervertebral disc herniation, spinal stenosis, acute myelitis, spinal demyelinating disease, syringomyelia, or spinal cord tumors [3–5]. There are reports that patients with spinal dural arteriovenous fistula have symptoms that persist for several years before receiving a confirmed diagnosis. This case suggests that when low back pain occurs, the possibility of spinal dural arteriovenous fistula should be considered, and the use of glucocorticoids for local blocking therapy requires caution.
It is not uncommon for patients with spinal arteriovenous fistula to experience accompanying symptoms of pain. However, there are currently few reports of spinal dural arteriovenous fistula with chronic low back pain as the only symptom at disease onset, especially cases of pain lasting for 1 year without showing any other symptoms. The clinical symptoms are often manifested as subacute or chronic onset of myelopathy symptoms such as limb weakness, sensory disorders, and sphincter disturbances. Hence, it is important to consider spinal arteriovenous fistula in patients with chronic low back pain. There are case reports suggesting that patients with spinal cord arteriovenous malformations have relatively mild back pain (VAS score 1–6), often manifested as radiating pain accompanied by neurological deficits [6]. The physiological mechanism of chronic low back pain caused by spinal dural arteriovenous fistula is currently not fully understood. It may be related to the compression of the spinal cord and nerve roots, spinal cord ischemia and edema, hemodynamic changes caused by arteriovenous fistula, or other causes of neuropathic pain [7]. The arteriovenous fistula-associated steal mechanism could be the possible reason for the pain, swelling, and necrosis. This patient’s T7-T12 spinal swelling and demyelination could have been congestive myelopathy secondary to progressive venous hypertension from spinal arteriovenous fistula [8]. Other diseases with chronic low back pain as the main clinical symptoms include lumbar spondylosis, myofasciitis, and spinal artery infarction. However, the clinical manifestations of pain caused by these diseases may differ from that caused by spinal dural arteriovenous fistula. The low back pain of lumbar spondylosis worsens during weight-bearing, often manifested as severe low back pain and numbness and weakness in the lower limbs, with relatively severe pain levels (VAS 9–10), and often accompanied by severe limitations in lumbar forward flexion function. Myofasciitis accounts for a large proportion of patients with low back pain [9], often manifested as chronic pain in areas such as the lower back, with limited mobility, local tenderness, referred pain, and tight muscles, with moderate pain levels (VAS 7–8). Most of these 2 types of pain are relieved after local blocking treatment. Spinal artery infarction can also manifest as low back pain, but in most of cases the disease onset is sudden, the degree of pain does not change with body position, and the degree of pain is severe (VAS 9–10) [6].
As the disease progresses, some patients may receive “local blocking treatment” with injections of corticosteroids and other drugs when they experience worsening back pain. There are reports suggesting that the use of glucocorticoids worsens symptoms in patients with spinal dural arteriovenous fistula [10,11]. The possible mechanism is the retention of water and sodium after intravenous drip or local use of glucocorticoid, and the increase of venous blood volume, which can further increase the spinal cord venous pressure, aggravate obstruction of venous circumfluence, and thus lead to aggravation of spinal cord edema and ischemia. The worsening of symptoms after the use of glucocorticoids is one of the clinical characteristics of spinal dural arteriovenous fistula [12]. Therefore, for patients with suspected spinal dural arteriovenous fistula, it is recommended to avoid the use of glucocorticoids as much as possible. Complete and comprehensive super-selective spinal angiography should be performed on suspected spinal dural arteriovenous fistula patients to avoid misdiagnosis.
Although selective spinal cord angiography has been performed on some patients, the arteries that supply spinal vascular lesions may also be missed, causing such patients to be misdiagnosed, possibly because no super-selective catheterization angiography was performed on blood vessels, no prolonged or enlarged angiography was performed on small spinal vascular lesions, or no selective angiography was performed on rare spinal vascular diseases caused by paravertebral vein stenosis or occlusion, such as azygos vein, semi-azygos vein, accessory azygos vein, ascending lumbar vein, internal iliac vein, or left renal vein. Failure to perform multimodal 3D image fusion for complex vascular lesions in the spinal cord can also lead to missed diagnosis of spinal vascular malformations [13,14]. There are also cases where some clinical symptoms and MRI examinations indicate spinal vascular disease, but multiple comprehensive spinal angiography and cerebral angiography have not found the cause, which is believed to be occult dural arteriovenous fistula according to previous research [15]. MRI shows that the flow signal behind the spinal cord is an imaging feature of spinal arteriovenous fistula. However, MRI has certain limitations in diagnosing spinal arteriovenous fistula. The sensitivity of advanced MRI techniques remains unclear, notably for the detection of low-flow shunts without flow voids. In our patient, the first MRI examination of the patient did not detect any abnormalities indicating spinal arteriovenous fistula. After the symptoms worsened, a re-examination of MRI showed a flow signal behind the spinal cord, which may have been related to changes in the flow rate of the fistula. Therefore, catheter angiography remains the criterion standard modality for evaluation of spinal vasculature and its disorders [16].
At present, surgical resection of drainage or endovascular embolization of the fistula is the main method for spinal dural arteriovenous fistula (SDAVF) treatment. Endovascular embolization has promise as a new treatment for spinal AVF/arteriovenous malformation(AVM) because it is less invasive, and it may be useful in the process of diagnostic DSA [8]. Previous research has shown that due to a recurrence rate of over 83% after endovascular embolization, interventional embolization is not the preferred treatment for SDAVF [17–19]. With the development of intravascular interventional technology, recent studies have shown that there is no significant difference between endovascular embolization treatment and surgical treatment in terms of recurrence rate, neurological function recovery, and complications. The choice of treatment of spinal AVF/AVM mainly depends on the type of lesions; surgery is preferred for intradural dorsal AVF[20] (as with our patient’s situation). Endovascular embolization therapy has the following limitations: (1) Abnormal tortuous root artery obstructs the catheter from entering the fistula; and (2) If the supply artery of SDAVF supplies both a spinal cord blood vessel and a fistula, it is more suitable for surgical resection. Otherwise, embolization of the supply artery will lead to spinal cord ischemic necrosis [21,22]. The patient in this case had the second condition, therefore, surgical resection treatment was used.
Conclusions
In summary, this case suggests that: (1) For patients with chronic low back pain, the possibility of spinal cord arteriovenous malformations should be considered, especially for patients with mild pain at the onset, pain is related to changes in posture, and symptoms worsen after the use of glucocorticoids; and (2) Chronic pain is one of the causes of disability in spinal dural arteriovenous fistula. It is necessary to further study the mechanism of low back pain caused by spinal dural arteriovenous fistula, and to consider medication, psychological, and behavioral therapy for chronic low back pain as an important component of the treatment.
Figures
References:
1.. Foster NE, Anema JR, Cherkin D, Prevention and treatment of low back pain: Evidence, challenges, and promising directions: Lancet (London, England), 2018; 391; 2368-83
2.. Harrisson SA, Stynes S, Dunn KM, Neuropathic pain in low back-related leg pain patients: What is the evidence of prevalence, characteristics, and prognosis in primary care? A systematic review of the literature: J Pain, 2017; 18; 1295-312
3.. Tobin WO, Weinshenker BG, Lucchinetti CF, Longitudinally extensive transverse myelitis: Curr Opin Neurol, 2014; 27; 279-89
4.. Zhang HB, Zhai XL, Li L, Imaging characteristics, misdiagnosis and microsurgical outcomes of patients with spinal dural arteriovenous fistula: A retrospective study of 32 patients: Ann Transl Med, 2022; 10; 832
5.. Kim MG, Jeong SW, Solli E, Temporal evolution of a patient with a spinal dural arteriovenous fistula on serial MRI: Spinal Cord Ser Cases, 2018; 4; 10
6.. Gogu AE, Pusztai A, Stroe AZ, Back pain in rare diseases: A comparison of neck and back pain between spinal cord ischemia and spinal dural arteriovenous fistula: Brain Sci, 2020; 10(9); 618
7.. Uchida K, Hokaku H, Aoyagi C, [Consideration of the mechanism for anterior condylar confluent dural AVF diagnosed with neck pain.]: No Shinkei Geka, 2019; 47; 419-27 [in Japanese]
8.. Essibayi MA, Srinivasan VM, Spinal dorsal intradural arteriovenous fistulas: Natural history, imaging, and management: Neurology, 2023; 101(12); 524-35
9.. Nouged E, Dajani J, Ku B, Local anesthetic injections for the short-term treatment of head and neck myofascial pain syndrome: A systematic review with meta-analysis: J Oral Facial Pain Headache, 2019; 33(2); 183-98
10.. DiSano MA, Cerejo R, Mays M, Acute paraparesis and sensory loss following intravenous corticosteroid administration in a case of longitudinally extensive transverse myelitis caused by spinal dural arteriovenous fistula: Case report and review of literature: Spinal Cord Ser Cases, 2017; 3; 17025
11.. Nasr DM, Brinjikji W, Rabinstein AA, Lanzino G, Clinical outcomes following corticosteroid administration in patients with delayed diagnosis of spinal arteriovenous fistulas: J Neurointerv Surg, 2017; 9; 607-10
12.. Hsu WC, Lin WC, Lieu AS, Acute quadriparesis caused by spinal arteriovenous malformation: A case report: Am J Emerg Med, 2008; 26; 731.e1-3
13.. Fukuda K, Higashi T, Okawa M, Fusion technique using three-dimensional digital subtraction angiography in the evaluation of complex cerebral and spinal vascular malformations: World Neurosurg, 2016; 85; 353-58
14.. Gailloud P, Diagnostic inefficiency of nonselective spinal angiography(Flush Aortography) in the evaluation of the normal and pathological spinal vasculature: Curr Probl Diagn Radiol, 2016; 45(3); 180-84
15.. Tsutsumi S, Abe Y, Yasumoto Y, Ito M, Lumbar congestive myelopathy mimicking neoplasia without concurrent vascular malformation: Neurol Med Chir (Tokyo), 2009; 49; 316-19
16.. Gailloud P, Spinal vascular malformations: Angiographic evaluation and endovascular management: Handb Clin Neurol, 2021; 176; 267-304
17.. Fiaschi P, Prior A, Sbaffi PF, Spinal dural arteriovenous fistulas: Clinical results and quality of life assessment with surgical treatment as a crucial therapy. The joint experience of two centers: World Neurosurg, 2019; 122; e270-e78
18.. , Open and endovascular treatment of spinal dural arteriovenous fistulas: A 10-year experience: J Neurosurg Spine, 2017; 26(4); 519-23
19.. Xu DS, Sun H, Spetzler RF, Spinal arteriovenous malformations: Surgical management: Handb Clin Neurol, 2017; 143; 153-60
20.. Ehresman J, Catapano JS, Baranoski JF, Treatment of spinal arteriovenous malformation and fistula: Neurosurg Clin North Am, 2022; 33(2); 193-206
21.. Sasamori T, Hida K, Yano S, Long-term outcomes after surgical and endovascular treatment of spinal dural arteriovenous fistulae: Eur Spine J, 2016; 25(3); 748-54
22.. Signorelli F, Gory B, Maduri R, Intracranial dural arteriovenous fistulas: A review of their current management based on emerging knowledge: J Neurosurg Sci, 2017; 61(2); 193-206
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952791

Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133