22 July 2024: Articles 
Combined Prolotherapy and Physical Therapy in a 60-Year-Old Man with Left Shoulder Pain and Limited Range of Motion (Frozen Shoulder) Following a Hemiplegic Stroke: A Case Report
Unknown etiology, Unusual setting of medical care, Educational Purpose (only if useful for a systematic review or synthesis)
Nuralam Sam1ACDEF*, A. Tazkiyah Batari UlengDOI: 10.12659/AJCR.944054
Am J Case Rep 2024; 25:e944054






Abstract
BACKGROUND: Frozen shoulder with limited range of motion is a common and debilitating condition that occurs on the affected side following a stroke. The effectiveness of therapy was reported to be negatively correlated with the complexity of pathogenesis. Prolotherapy involves injection into the joint of a small amount of irritant, such as dextrose, which enhances tissue strength and facilitates healing by targeting joint spaces. The treatment is used to relieve pain. This report describes the effects of combined prolotherapy and physical therapy in a 60-year-old man with left shoulder pain and limited range of motion (frozen shoulder) following a hemiplegic stroke.
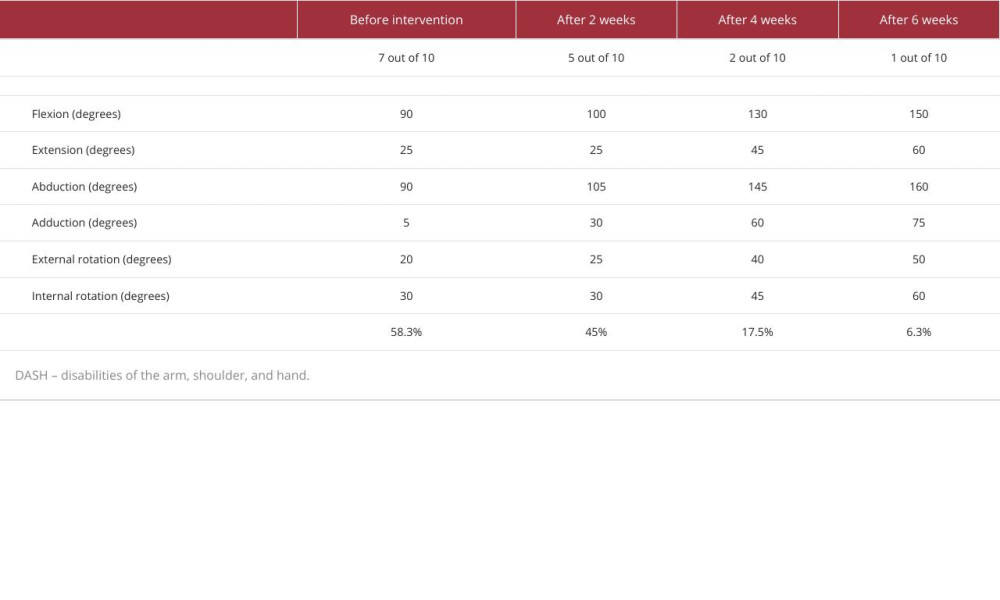
CASE REPORT: A 60-year-old man had left shoulder pain and limited ROM for 9 months, which disrupted daily life, with a NRS of 7 and a DASH score of 58.3%. The patient had an ischemic stroke 1 year ago, with left extremity weakness. On physical examination, joint active ROM was significantly restricted and the joint was tender upon palpation. Therapy is carried out using prolotherapy combined with exercise and physical therapy for 6 weeks. At the 6-week follow-up, he had good outcomes for pain relief, increasing ROM, and quality of life.
CONCLUSIONS: The use of prolotherapy with physical therapy may be an effective treatment for painful frozen shoulder following a hemiplegic stroke.
Keywords: Bursitis, ischemic stroke, Prolotherapy, Humans, Male, Middle Aged, shoulder pain, Range of Motion, Articular, Physical Therapy Modalities, Hemiplegia, Stroke, Combined Modality Therapy
Introduction
Stroke patients with arm paralysis are particularly at risk for frozen shoulder (FS) [1,2]. Frozen shoulders cause significant morbidity, with signs and symptoms of shoulder pain and restricted range of motion (ROM) that affect activities of daily living, reduced limb function, and cause withdrawal from rehabilitation programs [2,3]. FS is common after periods of immobilization, such as after a stroke [1]. The symptoms of FS usually last between from 6 months to several years without intervention, and it significantly reduces quality of life, especially with post-stroke patients [1,4]. A study of the association between ischemic stroke and FS found that the risk for FS in patients with stroke was higher than in healthy controls [4]. On the hemiplegic hand, pain impacts 22–23% of stroke survivors with stiffness of the shoulder [5]. It is caused by FS characteristics with fibroproliferative tissue fibrosis, producing type I and type III collagen, transforming into myofibroblasts, which is accompanied by inflammation, neo-angiogenesis, and neoinnervation, resulting in shoulder capsular fibrotic contractures and the associated clinical stiffness [6,7].
The best management option for FS remains controversial. Treatment of patients should be based on the stage of disease and symptoms. The goal of therapy is control of inflammation and relief of pain with increased ROM and quality of life [8,9]. Especially in patients with stroke, the effectiveness of therapy was negatively correlated with the complex pathogenesis. Currently, a number of therapy strategies are being researched to address FS in stroke survivors. Early rehabilitation and injection intervention are crucial to reduce the severity and prevent contractures and muscle atrophy in stroke survivors [5,10]. Consistent monitoring by healthcare professionals and well-informed patients is essential. This approach offers the chance to improve functionality and enhance the overall quality of life [11]. Prolotherapy has been employed in managing diverse chronic musculoskeletal conditions, demonstrating relative safety with minimal adverse effects or contraindications [12]. A systematic review showed good outcomes, indicating the therapeutic efficacy of prolotherapy in addressing musculoskeletal pain and joint laxity [13]. This injectable therapeutic approach specifically targets substances within tendons, ligaments, and articular spaces, addressing the underlying causes of pain and impairment associated with joint spaces. The aim is to stimulate a proliferative cascade, thereby enhancing tissue strength and promoting repair [14]. A systematic review and meta-analysis of dextrose-based prolotherapy by Bae et al showed a significant benefit for patients with chronic musculoskeletal pain, ranging from 6 months to 1 year, suggesting that prolotherapy has a better therapeutic effect than exercise [15]. This report describes the effects of combined prolotherapy and physical therapy in a 60-year-old man with left shoulder pain and limited range of motion (frozen shoulder) following a hemiplegic stoke.
Case Report
INTERVENTION:
Regular prolotherapy injections were administered in conjunction with physical therapy interventions as part of the patient’s treatment plan. The prolotherapy injection was prepared using a 10-ml disposable syringe, consisting of 3.75 ml of dextrose 15%, 1 ml of lidocaine, and 5.25 ml of sterile water. Injection points on the rotator cuff included the teres minor, subscapularis, supraspinatus, and infraspinatus. Intraarticular injections were performed by a licensed medical professional targeting the glenohumeral joint, subacromial bursa, long head biceps tendon, and acromioclavicular joint. A total of 4 injections were administered at 2-week intervals.
The patients who have been in the frozen phase for 9 months are beginning to experience a reduction in pain, but there is a characteristic progressive loss of range of motion (ROM). In this stage, physical therapy with stretching and strengthening exercises (isometric/static) of the shoulder, gentle stretches, and ultrasound diathermy using transcutaneous electrical nerve stimulation (TENS) modalities of the shoulder area are all part of the treatment, combined with stretching exercises for relief with gentle shoulder mobilization: active assisted shoulder forward flexion with a wand, active assisted shoulder external rotation with a wand, and pendulum exercise. Strengthening exercises are added to maintain muscle strength; exercises include scapular retraction with scapulae pulled towards each other, posterior capsule stretch, and isometric shoulder external rotation, as well as rotator cuff exercise and posture exercise. Interventions included a home exercise program, instruction in shoulder compression heat/ice use, and stretching and muscle strengthening.
Our patient underwent a regimen of three 2-weekly therapy sessions, followed by clinical evaluations that included assessments of pain, range of motion (ROM), and the DASH score. The patient received intensive and consistent therapeutic interventions from the first through the sixth week.
During the second-week visit, the patient’s left range of motion (ROM) measured using goniometry was: flexion 100 degrees, extension 25 degrees, abduction 105 degrees, adduction 30 degrees, external rotation 25 degrees, and internal rotation 30 degrees. At that point, quality of life assessed based on the Disability of the Arm, Shoulder, and Hand (DASH) score was 45%, suggesting an improvement in overall function, with NRS score 5 out of 10.
Upon assessment in the fourth week, the patient demonstrated further improvement, with a DASH score of 17.5%. The left range of motion during this appointment was: flexion 130 degrees, extension 45 degrees, abduction 145 degrees, adduction 60 degrees, external rotation 40 degrees, and internal rotation 45 degrees.
During the sixth-week visit, the patient exhibited notable improvements in the right glenohumeral active range of motion (ROM). The measurements included 150 degrees of flexion, 60 degrees of extension, 160 degrees of abduction, 75 degrees of adduction, 50 degrees of external rotation, and 60 degrees of internal rotation, and there were improvements in other aspects of range of motion. There were no complications or adverse reactions after intervention during the sixth week.
The combined approach of prolotherapy injections and physical therapy over the 6-week treatment period demonstrated enhanced pain management and functional improvement, as indicated by a decrease in the Disability of the Arm, Shoulder, and Hand (DASH) score to 6.3%, as detailed in Table 1.
Discussion
Frozen shoulder after a stroke can be effectively treated with early shoulder physical therapy. With this therapy, the shoulder gradually becomes easier to move and the brain is stimulated to rewire neural pathways between the brain and muscles [16]. According to Page et al, patients with FS showed a gain in function and ROM when they received therapy that included strengthening, stretching, and diathermy ultrasound. Interventions aim to reduce pain, promote healing, decrease spasms in the muscles, increase the range of motion of the joints, strengthen weak muscles, and enhance biomechanics and function [17].
After a stroke, patients with weakened hemiparetic shoulders are more susceptible to frozen shoulder than the general population [18]. The hemiparetic shoulder’s soft tissue is more resistant to injury and inflammation due to aging, microvascular comorbidities, and subluxation. Inflammation can trigger fibrosis of the ligamentous capsule around the shoulder. It is this fibrosis that results in the common presentation features of FS, namely restriction of range of motion and pain [18–20]. This is consistent with the patient’s symptoms in the case above.
Treatment of hemiparetic frozen shoulder is mainly based on experience with the general population. Improvements in symptoms and shoulder ROM depend on education to prevent any movement fear and to encourage regular daily hemiparetic shoulder movements [21]. In daily clinical practice, various physical treatment modalities are used for FS. Prolotherapy injection-based regenerative method, which gains popularity in the treatment of musculoskeletal pathologies [22], were tried by Lee et al [23] to treat patients with non-traumatic refractory rotator cuff disease who had been experiencing symptoms for 3 months. The authors reported a significant reduction in pain, disability, isometric strength, and shoulder motion after 3–8 injection sessions. Prolotherapy injections were used by Bertrand et al [24] for rotator cuff tendinopathy in a randomized controlled trial. Prolotherapy in patients with frozen shoulder has proven to be a good adjunctive approach, showing promising benefits in reducing pain, enhancing range of motion, and improving shoulder functionality [25,26]. The results showed a significant improvement in pain and functional scores. Prolotherapy is a potential treatment option for many shoulder pathologies and stiffness, including hemiparetic frozen shoulder.
Fortunately, the results show that prolotherapy injection combined with physical therapy exercise during 6 weeks decreased pain and improved shoulder ROM and quality of life in our patient with frozen shoulder. These interventions are used when the previous conventional physiotherapies have not caused improvement. However, further research is needed with a randomized controlled study and a larger sample to determine the effectiveness of prolotherapy in hemiparetic frozen shoulder.
A limitation of this report is that it is based on a single case, so the findings cannot be generalized, and the patients must be highly motivated in performing a home exercise program for the maximum improvement of range of motion.
Conclusions
We found that use of prolotherapy with physical therapy can achieve good results in a patient with painful frozen shoulder following a hemiplegic stroke, significantly decreasing pain, improving ROM, and improving quality of life.
References:
1.. Zreik NH, Malik RA, Charalambous CP, Adhesive capsulitis of the shoulder and diabetes: A meta-analysis of prevalence: Muscles Ligaments Tendons J, 2016; 6(1); 26-34
2.. Lv X, Hu Z, Liang F, Causal relationship between ischemic stroke and its subtypes and frozen shoulder: A two-sample Mendelian randomization analysis: Front Neurol, 2023; 14; 1178051
3.. Millar NL, Meakins A, Struyf F, Frozen shoulder: Nat Rev Dis Primers, 2022; 8(1); 59
4.. Kang JH, Sheu JJ, Lin HC, Increased risk of stroke after adhesive capsulitis: A population-based study: Stroke, 2010; 41; 1044-47
5.. Zhu Y, Su B, Li N, Jin H, Pain management of hemiplegic shoulder pain post stroke in patients from Nanjing, China: Neural Regen Res, 2013; 8; 2389-98
6.. Le HV, Lee SJ, Nazarian A, Rodriguez EK, Adhesive capsulitis of the shoulder: Review of pathophysiology and current clinical treatments: Shoulder Elb, 2017; 9; 75-84
7.. Pietrzak M, Adhesive capsulitis: An age-related symptom of metabolic syndrome and chronic low-grade inflammation?: Med Hypotheses, 2016; 88; 12-17
8.. Neviaser AS, Hannafin JA, Adhesive capsulitis: a review of current treatment: Am J Sports Med, 2010; 38(11); 2346-56
9.. Via AG, Frizziero A, Oliva F, Treatment of adhesive capsulitis: A review: Muscles Ligaments Tendons J, 2012; 2(2); 70-78
10.. Smith M, Management of hemiplegic shoulder pain following stroke: Nurs Stand, 2012; 26(44); 35-44
11.. Vasudevan JM, Browne BJ, Hemiplegic shoulder pain: An approach to diagnosis and management: Phys Med Rehabil Clin N Am, 2014; 25(2); 411-37
12.. Distel LM, Best TM, Prolotherapy: A clinical review of its role in treating chronic musculoskeletal pain: PM R, 2011; 3(6 Suppl. 1); S78-81
13.. Rabago D, Best TM, Beamsley M, Patterson J, A systematic review of prolotherapy for chronic musculoskeletal pain: Clin J Sport Med, 2005; 15(5); 376-80
14.. Hung CY, Hsiao MY, Chang KV, Comparative effectiveness of dextrose prolotherapy versus control injections and exercise in the management of osteoarthritis pain: A systematic review and meta-analysis: J Pain Res, 2016; 9; 847-57
15.. Bae G, Kim S, Lee S, Lee WY, Lim Y, Prolotherapy for the patients with chronic musculoskeletal pain: Systematic review and meta-analysis: Anesth Pain Med (Seoul), 2020; 16(1); 81-95
16.. Bertrand H, Reeves KD, Bennett CJ, Dextrose prolotherapy versus control injections in painful rotator cuff tendinopathy: Arch Phys Med Rehabil, 2016; 97; 17-25
17.. Millar NL, Meakins A, Struyf F, Frozen shoulder: Nat Rev Dis Primers, 2022; 8(1); 59
18.. Lo SF, Chen SY, Lin HC, Arthrographic and clinical findings in patients with hemiplegic shoulder pain: Arch Phys Med Rehabil, 2003; 84(12); 1786-91
19.. Ada L, Preston E, Langhammer B, Canning CG, Profile of upper limb recovery and development of secondary impairments in patients after stroke with a disabled upper limb: An observational study: Physiother Theory Pract, 2020; 36(1); 196-202
20.. Andrews AW, Bohannon RW, Decreased shoulder range of motion on paretic side after stroke: Phys Ther, 1989; 69(9); 768-72
21.. Hou Y, Wang Y, Sun X, Effectiveness of suprascapular nerve block in the treatment of hemiplegic shoulder pain: A systematic review and meta-analysis: Front Neurol, 2021; 12; 723664
22.. Ersen O, Koca K, Akpancar S, A randomized-controlled trial of prolotherapy injections in the treatment of plantar fasciitis: Turk J Phys Med Rehab, 2018; 64; 59-65
23.. Lee DH, Kwack KS, Rah UW, Yoon SH, Prolotherapy for refractory rotator cuff disease: Retrospective case-control study of 1-year follow-up: Arch Phys Med Rehabil, 2015; 96; 2027-32
24.. Page MJ, Green S, Kramer S, Manual therapy and exercise for adhesive capsulitis (frozen shoulder): Cochrane Database Syst Rev, 2014(8); CD011275
25.. Sam N, Yusuf I, Idris I, A case series: Effect of comorbidities on the outcomes of prolotherapy injection for frozen shoulder patients: Int Med Case Rep J, 2023; 16; 257-63
26.. Seven MM, Ersen O, Akpancar S, Effectiveness of prolotherapy in the treatment of chronic rotator cuff lesions: Orthop Traumatol Surg Res, 2017; 103(3); 427-33
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133