25 June 2024: Articles 
Regenerative Endodontic Procedure on an Immature Necrotic Molar: A Case Report with a 5-Year Review
Unusual or unexpected effect of treatment
Majed A. AlmalkiDOI: 10.12659/AJCR.944179
Am J Case Rep 2024; 25:e944179






Abstract
BACKGROUND: The regenerative endodontic procedure (REP) for managing necrotic immature permanent teeth has the advantage of promoting root growth over the traditionally used apexification techniques. However, there is limited evidence on the long-term outcome of standardized REPs performed on immature molars. This case report presents the 5-year clinical and radiographic outcomes of REP performed on an immature mandibular first molar.
CASE REPORT: A healthy 7-year-old girl with a carious right mandibular first molar was referred to the endodontic clinic for evaluation and treatment. Clinical examination showed large occlusal caries, no tenderness to palpation and percussion tests, and no response to cold and electric pulp tests. Radiographic examination showed deep caries, apical radiolucency related to the open apices, and wide root canal space. Accordingly, the tooth was diagnosed with necrotic pulp and asymptomatic apical periodontitis. The REP was performed following the American Association of Endodontics guidelines, which comprise minimal instrumentation, disinfection with sodium hypochlorite irrigant, use of triple antibiotic paste, induced intracanal bleeding, and application of a coronal mineral trioxide aggregate plug. The patient missed the scheduled follow-up appointments but presented at the clinic 5 years later with an asymptomatic tooth. Clinical and radiographic examination revealed no tenderness to percussion and palpation test, no response to cold test, positive response to electric pulp test, apical healing, apical closure, root lengthening, and canal wall thickening and calcification.
CONCLUSIONS: While true pulp regeneration is unachievable, the REP, following the current protocol, is clinically successful in achieving root maturation and tooth retention.
Keywords: Regenerative Endodontics, Anti-Bacterial Agents, Apexification, Dentistry, Pediatric Dentistry, Mineral Trioxide Aggregate, Humans, Female, Child, Molar, Dental Pulp Necrosis, Drug Combinations, Periapical Periodontitis
Introduction
The success of endodontic management of necrotic immature teeth is adversely affected by several factors, including incomplete root formation and compromised crown/root ratio, which complicate performing a standard root canal therapy protocol and tooth restoration. Moreover, the wide apex of the root does not allow optimum filling, and the thin dentinal walls of the roots are highly vulnerable to fracture [1,2].
The classic treatment for necrotic immature permanent teeth is apexification with calcium hydroxide or mineral trioxide aggregate (MTA). Although both techniques produce satisfactory results, treatment difficulties and complications associated with a short and thin root have yet to be solved [1].
In 2004, Banchs and Trope proposed a revascularization protocol that includes the use of triple antibiotic paste (TAP; comprising metronidazole, ciprofloxacin, and minocycline) as an intracanal medicament, intracanal bleeding as a scaffold, and an MTA material as an intracanal barrier. They reported that after 2 years of follow-up visits, their patient’s tooth was symptom-free and responded to the cold test, while radiographic examination showed apical closure with dentinal wall thickening [3].
The American Association of Endodontics (AAE) and the European Society of Endodontology have published guidelines for the procedure to help standardize the treatment protocol [4,5]. However, several variations of these guidelines have been reported in the literature, including a single-visit regenerative endodontic procedure (REP), different disinfection protocols, different types of scaffold, and different types of sealing material [6]. Additionally, most published studies have focused primarily on single-rooted immature teeth, with only a limited number including immature molars, and had a relatively short follow-up period [7].
This case report presents the 5-year clinical and radiographic outcomes of REP performed according to the AAE guidelines on an immature mandibular molar.
Case Report
CLINICAL PRESENTATION:
A healthy 7-year-old girl was referred to the endodontic clinic for root canal treatment of the right mandibular first molar. The patient visited the clinic accompanied by her father. She presented with no complaints but had a history of tooth pain and extraoral swelling, which were treated by the general dentist 1 month before with an antibiotic course and a pain-killer. On clinical examination, the tooth had a large and deep carious cavity in the occlusal surface. Clinical tests were first performed on the left mandibular first molar (control tooth) to establish a baseline for the patient’s normal response. The control tooth was not tender to percussion or palpation and responded within the normal range to the cold test (Endo-Ice; Coltène/Whaledent Inc., Cuyahoga Falls, OH, USA) and electrical pulp test (Gentle-Pulse; Parkell Inc., Edgewood, NY, USA). Then, the same clinical tests were applied to the right mandibular first molar (offending tooth). The offending tooth was not tender to percussion or palpation and did not respond to the cold test or electrical pulp tester. Periodontal examination revealed a normal range of pocket depth (1–2 mm) and no tooth mobility. A periapical radiograph was taken using a GXS-700 digital sensor (Gendex Dental System, Des Plaines, IL, USA) and a KaVo Focus X-ray machine (Instrumentarium Dental, PaloDEx Group Oy, Tuusula, Finland) and visualized using the VixWin Platinum image management software (Gendex Software System, Hatfield, PA, USA). Deep caries and periapical radiolucency related to the open apices of both immature roots were evident in the radiograph (Figure 1). Accordingly, the tooth was diagnosed with necrotic pulp and asymptomatic apical periodontitis.
The diagnosis and treatment options of REP and MTA apexification with the associated procedural details, benefits, risks, and complications were explained to the patient and her father. The possible risks and complications associated with extraction and the no-treatment option were also discussed. The treatment plan of performing a multi-visit REP, followed by a composite buildup, was agreed upon, and a consent form was obtained from the patient’s father. However, consent for clinical photography was declined.
FIRST VISIT:
The tooth was anesthetized using 1 cartridge of 2% lidocaine with 1: 100 000 epinephrine (Lignospan Special; Septodont, Saint-Maur-des-Fosses, France) and isolated with a rubber dam (Hygienic; Coltène/Whaledent Inc., OH, USA). The tooth and rubber dam were wiped with 2% chlorohexidine (Consepsis; Ultradent Products, Inc., UT, USA), and soft caries were removed using a multi-purpose bur (Dentsply Maillefer, Ballaigues, Switzerland). Under a surgical microscope (OMS 2350; Zumax Medical Co., Ltd., Jiangsu, China), the access cavity was prepared with the same bur, and 3 canal orifices were identified, with no sign of vital tissue. The lengths of the canals were initially estimated from a digital periapical radiograph and then adjusted and confirmed using size 30 and 55 K-files (Dentsply Maillefer, Ballaigues, Switzerland) and a Root ZX apex locator (J Morita MFG Corp., Kyoto, Japan). Minimal instrumentation was achieved using a K-file 1 mm shorter than the working length. A 27-gauge side-vented needle (Miraject; Hager & Werken GmbH & Co. KG, Duisburg, Germany) attached to a 10-mL syringe was adjusted (made 2 mm shorter than the working length) and used in a back-and-forth motion while irrigating the canals. A total volume of 20 mL of 1.5% sodium hypochlorite (NaOCl; 5M; Biotischen, Riyadh, Saudi Arabia) was used to irrigate each canal. Next, the canals were irrigated with normal saline (Pharmaceutical Solution Ind., Riyadh, Saudi Arabia), followed by 17% ethylenediaminetetraacetic acid (EDTA; Canalarge, Ammdent, Punjab, India). The canals were dried with paper points, and a bonding agent (Tetric N Bond; Ivoclar Vivadent AG, Schaan, Liechtenstein) was applied to the coronal dentin. According to the AAE recommendations, the hospital pharmacy prepared a TAP mixture using equal portions of powders of ciprofloxacin (Cipromax; Spimaco, Buraydah, Saudi Arabia), metronidazole (Flazol; Tabuk Pharmaceutical Manufacturing CO., Tabuk, Saudi Arabia), and minocycline (Vulga; Jazeera Pharmaceutical Ind., Riyadh, Saudi Arabia). A plastic needle was used to apply the mixture in the canals. Lastly, the canal orifices were covered with small cotton pellets and sealed with a temporary filling (Cavit; 3M Deutschland GmbH, Neuss, Germany).
SECOND AND THIRD VISITS:
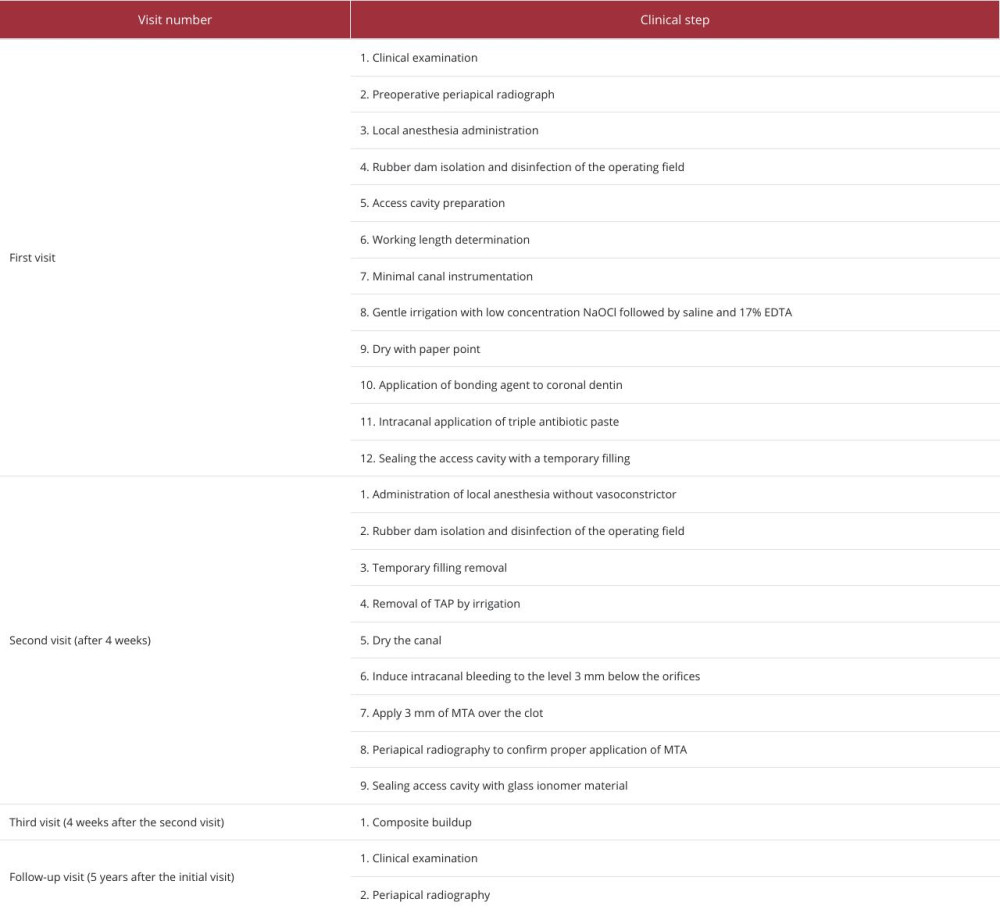
After 4 weeks, the patient presented with an asymptomatic tooth. The tooth was anesthetized using 4% prilocaine (4% Citanest Plain Dental; Dentsply Pharmaceutical, York, PA, USA) without a vasoconstrictor to encourage bleeding. Then, the tooth was isolated with a rubber dam and wiped with 2% chlorohexidine. Under a surgical microscope, the temporary filling was removed, and the canals were irrigated with 20 mL of 17% EDTA. Then, the canals were dried with a paper point, and a size 20 K-file with an apical bend was used to lacerate the periapical tissue and initiate bleeding in the canals. At first, it was easy to encourage bleeding from the distal canal to the level of 3 mm below the orifice, although a second attempt was required for the mesial canals. After clot formation, the orifices were filled with ProRoot white MTA (Dentsply Tulsa Dental, Tulsa, OK, USA) using an amalgam carrier, and a periapical radiograph was taken to confirm the proper application of the MTA (Figure 2). Finally, the access cavity was restored with a glass ionomer (Fuji II; GC, Tokyo, Japan) during the same visit, and 1 month later, the patient had a final composite filling placed (Filtek Z-250; 3M ESPE, Seefeld, Germany; Figure 3). A summary checklist of the regenerative procedure based on the AAE guidelines is presented in Table 1 [8].
FOLLOW-UP VISIT:
The patient had follow-up appointments scheduled at 6, 12, and 24 months. To ensure attendance, the patient received reminder messages 1 week and 1 day before each follow-up appointment. However, the patient consistently failed to attend. After 5 years, the patient finally visited her general dentist for a checkup appointment and was referred to the endodontic clinic. The patient’s father mentioned that the patient had no complaints and saw no reason to attend the prior appointments. The reason for the visit was to start orthodontic treatment, which required preliminary screening by a general dentist and endodontist.
Upon clinical examination, her tooth was symptom-free with intact restoration and was not tender to percussion or palpation. The probing depth was also within the normal range. Furthermore, her tooth was responsive to the electric pulp tester, although it was unresponsive to the cold test. A peri-apical radiograph was taken with the same X-ray machine used in the first visit but with a different sensor (VistaScan system; Dürr Dental AG, Beitigheim-Bissingen, Germany) and imaging software (DBSWIN; Dürr Dental AG, Beitigheim-Bissingen, Germany). In addition, the panoramic image was obtained using OP 3D Pro (Instrumentarium Dental, PaloDEx Group Oy, Tuusula, Finland) and imaging software (CliniView; Instrumentarium Dental, PaloDEx Group Oy, Tuusula, Finland). Radiographic examination showed complete periapical healing, apical closure, increased root length, increased dentin thickness, and narrowed canal spaces (Figures 4, 5).
Discussion
Endodontists face significant challenges when treating necrotic immature permanent teeth. They routinely practice both apexification and the REP when treating these cases, requiring careful selection of the appropriate procedure based on the case [9]. Patients with medical or psychological conditions that impair the immune system, blood clotting, normal healing, compliance with dental procedures, or attendance at multiple visits are poor candidates for the REP and are preferentially treated with apexification [9,10].
Patients’ ages and stages of tooth development are considered significant factors affecting the success of the REP. For instance, while several case reports have shown the feasibility of using the REP for mature and immature teeth in adult patients, the procedure has limited benefits, a low success rate, and a high risk of complications in these cases [9,10]. Another important factor is the diameter of the open apex. While an apical diameter as small as 0.24 mm is considered suitable for the REP, studies have shown that an apical diameter of at least 1 mm has better outcomes [9,11].
The patient in this case report was 7 years old at the time of treatment. Furthermore, she was categorized as ASA1 under the American Association of Anesthesiologists’ Health Classification System [12]. She also had stage IV root development based on the Cvek classification [13], and the apical diameter was >1 mm in both roots. Considering these factors and the potential advantages of each treatment option, the REP was suggested to and accepted by the patient’s father.
Patients’ compliance with dental visits is a crucial factor for the success of the multi-visit REP [10]. While a single-visit REP has been proposed as a viable alternative to overcome the issue of poor compliance, a recent systematic review emphasized its unpredictability [14]. The patient in this case report showed commitment to attend all visits required to treat the tooth. However, due to her father’s perception that they were unnecessary, she did not attend any follow-up appointments. A previous study reported that a lack of motivation was the main barrier to pediatric patients’ attendance at follow-up dental visits and the compliance of pediatric patients to dental follow-up visits was as low as 39.5% [15].
There should be 2 main clinical concerns when treating necrotic immature teeth with the REP. The first concern should be the dentinal wall since a thin wall limits the scope for mechanical preparation to the minimum [16]. The second should be balancing the antimicrobial ability of the irrigant and intracanal medicament with their cytotoxic effects on stem cells [17–19].
In the presented case, the apical lesion healing and maturity of the roots support the effectiveness of the low concentrations of NaOCl and TAP, as recommended by the AAE guidelines [4]. While 6% NaOCl and high-concentration TAP are reported to have been used in successful REP cases, they have also been shown to adversely affect stem cell survival in laboratory studies [3,19–21].
Calcium hydroxide (Ca[OH]2) is an alternative intracanal medicament that could have been used in this case. However, previous studies have demonstrated better antibacterial activity and higher percentages of root wall thickening with TAP [22,23].
Moreover, 17% EDTA was used as part of the irrigation protocol during the first and second appointments to promote the survival of the stem cells. This effect of EDTA is attributed to its interaction with NaOCl, which reduces the latter’s effect on stem cells and encourages the release of growth factors from dentin [24]. Dentin conditioning with EDTA has been demonstrated to release transforming growth factor beta (TGF-β) from root dentin, influencing stem cell migration and differentiation [25,26].
In the presented case, the scaffold was established by lacerating the apical tissue to induce intracanal bleeding. The first attempt successfully achieved sufficient bleeding in the distal canal, whereas an additional attempt was required for the mesial canals. Previous studies have suggested transferring blood from the distal to the mesial canal to overcome this issue [27,28]. However, the AAE guidelines suggest using platelet-rich plasma, platelet-rich fibrin, or autologous fibrin matrix as an alternative to blood clots [8].
The outcome of the REP can be assessed through achievement of treatment goals, which include resolution of apical periodontitis, tooth retention, root maturation, and regaining tooth vitality. In the presented case, the tooth was clinically asymptomatic, and apical radiolucency was resolved. This outcome is consistent with the high success rate reported with the REP, with a meta-analysis reporting an apical periodontitis healing rate of 93% [29]. Moreover, it has been reported that, compared to calcium hydroxide and MTA apexification, cases treated with the REP have shown better resolution of apical periodontitis [30].
Furthermore, root maturation is crucial for strengthening the root against fracture and increasing tooth retention. Studies have revealed that the REP promotes root elongation and dentin wall thickness better than apexification [30,31]. In the presented case, radiographic evidence confirmed the positive effect of the REP since root length and dentin thickness increased and the root apices were closed compared to their presentation at the initial visit and the counterpart tooth at the follow-up visit. A prospective study reported similar findings based on the Banchs and Trope treatment protocol, observing at follow-up after 8 years that root length and dentinal wall thickness showed a progressive increase, while a decrease in apical diameter was evident throughout the follow-up period [32]. However, the study involved only 2 molar teeth that were followed up for only 2 years.
In the literature, extensive canal obliteration is considered a typical drawback associated with the REP that could interfere with normal pulp function and complicate future retreatment in case of failure [6]. In the presented case, extensive calcification was visible. However, because there were no periodic follow-up radiographs, it is unknown whether this was progressive, like most reported cases in the literature. Therefore, future follow-up will be needed.
The AAE guidelines highly recommend using cone-beam computed tomography (CBCT) in initial and follow-up visits [8]. However, this analysis was not performed on the presented case because the CBCT machine was unavailable at the time of the initial visit. Consequently, conducting a CBCT scan at the follow-up visit had limited value. In addition, the AAE and the American Academy of Oral and Maxillofacial Radiology recommend using CBCT as an adjunct in situations where the interpretation of two-dimensional radiography is inconclusive [33].
Recent advancements in cellular therapy have shown promising results in terms of inducing pulp regeneration, and researchers have demonstrated the clinical potential of using allogeneic stromal cell transplantation to induce a dentin-pulp complex-like formation in immature teeth with necrotic pulp and apical periodontitis. However, additional studies are required to evaluate the full potential of this technique [34]. In the presented case, a positive response to the electric pulp test indicated revitalization but not histological regeneration of the pulp-dentin complex [6].
Furthermore, regenerative endodontic treatment involves a multistep procedure and relatively lengthy appointments that might be challenging for a young patient to tolerate. Therefore, the clinician should make every effort to reduce the patient’s fear and anxiety. The use of low-noise instruments and computerized devices for local anesthesia has recently gained attention for improving the clinical experience of pediatric patients [35,36]. Future research is needed to explore the implementation of such features with the REP.
The limitations of this case report include the common limitations of such studies that restrict their generalizability and interpretability, such as small sample size, selection bias, lack of control group, and reliance on retrospective data on the case. Therefore, findings of this report should be interpreted with caution. However, since current evidence on the long-term outcomes of applying the standardized REP on immature molars is inadequate, this study provides valuable insights. Nonetheless, further research, including randomized control trials, is required.
Conclusions
This case report presents the 5-year clinical and radiographic outcomes of an immature necrotic molar treated with the REP according to the AAE guidelines. While the goal of promoting true histological regeneration of the pulp-dentin complex has yet to be achieved, applying the REP with the current AAE protocol is clinically successful regarding the healing of apical periodontitis, root maturation, and tooth function. However, additional studies with larger numbers of cases and longer follow-up periods are needed.
Figures
References:
1.. Trope M, Treatment of the immature tooth with a non-vital pulp and apical periodontitis: Dent Clin N Am, 2010; 54(2); 313-24
2.. Cvek M, Tsilingaridis G, Andreasen JO, Survival of 534 incisors after intra-alveolar root fracture in patients aged 7–17 years: Dent Traumatol, 2008; 24(4); 379-87
3.. Banchs F, Trope M, Revascularization of immature permanent teeth with apical periodontitis: New treatment protocol?: J Endod, 2004; 30(4); 196-200
4.. , Considerations for a regenerative endodontics procedure: American Association of Endodontists, 2013 Available from: https://www.aae.org/specialty/wp-content/uploads/sites/2/2017/07/considerationsregendo.pdf
5.. Segura-Egea JJ, Gould K, Şen BH, European Society of Endodontology position statement: The use of antibiotics in endodontics: Int Endod J, 2018; 51(1); 20-25
6.. Kim SG, Malek M, Sigurdsson A, Regenerative endodontics: A comprehensive review: Int Endod J, 2018; 51(12); 1367-88
7.. Glynis A, Foschi F, Kefalou I, Regenerative endodontic procedures for the treatment of necrotic mature teeth with apical periodontitis: A systematic review and meta-analysis of randomized controlled trials: J Endod, 2021; 47(6); 873-82
8.. , Considerations for regenerative procedures: American Association of Endodontists, 2018 [cited 2018]. Available from: https://www.aae.org/specialty/wp-content/uploads/sites/2/2018/06/ConsiderationsForRegEndo_AsOfApril2018.pdf
9.. Wei X, Yang M, Yue L, Expert consensus on regenerative endodontic procedures: Int J Oral Sci, 2022; 14(1); 55
10.. Murray PE, Review of guidance for the selection of regenerative endodontics, apexogenesis, apexification, pulpotomy, and other endodontic treatments for immature permanent teeth: Int Endod J, 2023; 56(S2); 188-99
11.. Estefan BS, El Batouty KM, Nagy MM, Diogenes A, Influence of age and apical diameter on the success of endodontic regeneration procedures: J Endod, 2016; 42(11); 1620-25
12.. , Statement on ASA Physical Status Classification System: American Society of Anesthesiologists original approval: October 15, 2014. Available from:https://www.asahq.org/standards-and-practice-parameters/statement-on-asa-physical-status-classification-system
13.. Cvek M, Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha: A retrospective clinical study. Endod Dent Traumatol, 1992; 8(2); 45-55
14.. Rossi-Fedele G, Kahler B, Venkateshbabu N, Limited evidence suggests benefits of single visit revascularization endodontic procedures – a systematic review: Braz Dent J, 2019; 30(6); 527-35
15.. Gune NS, Katre AN, Dental practitioner’s perception of the compliance of pediatric patients to orofacial myotherapy treatment protocols: A mixed methods study: Int J Clin Pediatr Dent, 2021; 14(2); 222-28
16.. Fouad AF, Nosrat A, Pulp regeneration in previously infected root canal space: Endod Topics, 2013; 28(1); 24-37
17.. Galler KM, Buchalla W, Hiller K-A, Influence of root canal disinfectants on growth factor release from dentin: J Endod, 2015; 41(3); 363-68
18.. Trevino EG, Patwardhan AN, Henry MA, Effect of irrigants on the survival of human stem cells of the apical papilla in a platelet-rich plasma scaffold in human root tips: J Endod, 2011; 37(8); 1109-15
19.. Martin DE, De Almeida JFA, Henry MA, Concentration-dependent effect of sodium hypochlorite on stem cells of apical papilla survival and differentiation: J Endod, 2014; 40(1); 51-55
20.. de-Jesus-Soares A, Prado MC, Nardello LCL, Clinical and molecular microbiological evaluation of regenerative endodontic procedures in immature permanent teeth: J Endod, 2020; 46(10); 1448-54
21.. Ruparel NB, Teixeira FB, Ferraz CC, Diogenes A, Direct effect of intracanal medicaments on survival of stem cells of the apical papilla: J Endod, 2012; 38(10); 1372-75
22.. Maniglia-Ferreira C, de Almeida-Gomes F, Pinto MMN, de Sousa Barbosa FT, In vitro evaluation of the antimicrobial effects of different intra-canal medications in necrotic immature teeth: Eur Arch Paediatr Dent, 2016; 17(4); 251-55
23.. Báez V, Corcos L, Morgillo F, Meta-analysis of regenerative endodontics outcomes with antibiotics pastes and calcium hydroxide: The apex of the iceberg. J Oral Biol Craniofac Res, 2022; 12(1); 90-98
24.. Galler KM, D’Souza RN, Federlin M, Dentin conditioning codetermines cell fate in regenerative endodontics: J Endod, 2011; 37(11); 1536-41
25.. Nangia D, Saini A, Sharma S, Treatment outcome of regenerative endodontic procedures in mature permanent teeth compared to nonsurgical endodontic treatment: A systematic review and meta-analysis: J Conserv Dent, 2021; 24(6); 530-38
26.. Taweewattanapaisan P, Jantarat J, Ounjai P, Janebodin K, The effects of EDTA on blood clot in regenerative endodontic procedures: J Endod, 2019; 45(3); 281-86
27.. Alasqah M, Khan SIR, Alfouzan K, Jamleh A, Regenerative endodontic management of an immature molar using calcium hydroxide and triple antibiotic paste: A two-year follow-up: Case Rep Dent, 2020; 2020; 9025847
28.. Nosrat A, Seifi A, Asgary S, Regenerative endodontic treatment (revascularization) for necrotic immature permanent molars: A review and report of two cases with a new biomaterial: J Endod, 2011; 37(4); 562-67
29.. Ong TK, Lim GS, Singh M, Fial AV, Quantitative assessment of root development after regenerative endodontic therapy: A systematic review and meta-analysis: J Endod, 2020; 46(12); 1856-66.e2
30.. Jeeruphan T, Jantarat J, Yanpiset K, Mahidol Study 1: Comparison of radiographic and survival outcomes of immature teeth treated with either regenerative endodontic or apexification methods: A retrospective study: J Endod, 2012; 38(10); 1330-36
31.. Nagy MM, Tawfik HE, Hashem AAR, Abu-Seida AM, Regenerative potential of immature permanent teeth with necrotic pulps after different regenerative protocols: J Endod, 2014; 40(2); 192-98
32.. Abu Zeid ST, Alamoudi RA, Alothmani OS, A prospective study of long-term regenerative endodontics outcomes of necrotic immature permanent teeth: An 8-year follow-up: Healthcare (Basel), 2021; 9(12); 1670
33.. , AAE and AAOMR Joint Position Statement: Use of cone beam computed tomography in endodontics 2015 update: J Endod, 2015; 41(9); 1393-96
34.. Gomez-Sosa JF, Cardier JE, Wittig O, Allogeneic bone marrow mesenchymal stromal cell transplantation induces dentin pulp complex-like formation in immature teeth with pulp necrosis and apical periodontitis: J Endod, 2024; 50(4); 483-92
35.. Vitale MC, Gallo S, Pascadopoli M, Local anesthesia with SleeperOne S4 computerized device vs traditional syringe and perceived pain in pediatric patients: A randomized clinical trial: J Clin Pediatr Dent, 2023; 47(1); 82-90
36.. Kim IH, Cho H, Song JS, Assessment of real-time active noise control devices in dental treatment conditions: Int J Environ Res Public Health, 2022; 19(15); 9417
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952791

Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133