13 August 2024: Articles 
Effective Management of Methicillin-Resistant Shoulder Septic Arthritis Using Continuous Local Antibiotic Perfusion: A Case Study and Long-Term Follow-Up
Unusual setting of medical care, Rare disease
Shunya Yamaguchi1BDE, Shusuke Ueda1ABCDEF*, Toru Ichiseki12ABCDEFG, Daisuke Soma1B, Ayumi Kaneuji1G, Norio Kawahara1DGDOI: 10.12659/AJCR.944491
Am J Case Rep 2024; 25:e944491






Abstract
BACKGROUND: Septic arthritis of the shoulder is a rare and challenging condition to treat. Typically, arthroscopic debridement is the common approach. Specifically, septic arthritis of the shoulder caused by methicillin-resistant bacteria is extremely difficult to cure due to persistent infection and limited antibiotic options. However, recent studies have demonstrated that continuous local antibiotic perfusion (CLAP) can provide favorable results for bone and soft tissue infections. By administering the antibiotics required to suppress the biofilm, CLAP can effectively treat the infection while sparing the tissue.
CASE REPORT: A 46-year-old woman undergoing long-term hemodialysis treatment for congenital anomalies of the kidney and urinary tract experienced severe pain in the left shoulder joint during glucocorticoid treatment for amyloid arthritis of the right shoulder. Despite the absence of fever, significant swelling and fluid accumulation were observed in the left shoulder joint, leading to the performance of a puncture. A bacterial examination of the puncture fluid detected methicillin-resistant coagulase-negative Staphylococcus epidermidis (MRCNS). In this report, we present a case in which CLAP was administered for septic arthritis of the shoulder caused by methicillin-resistant bacteria. After irrigation debridement, the patient received intravenous antibiotics and CLAP. Following the initiation of treatment, the dosage of antibiotics was adjusted while performing therapeutic drug monitoring. An early improvement in the inflammatory response and sedation of the infection was observed, with no relapse after 2 years.
CONCLUSIONS: Septic arthritis can lead to serious functional impairment if left untreated. CLAP is a promising option for managing septic arthritis of the shoulder.
Keywords: Arthritis, Infectious, Methicillin Resistance, Perfusion, Shoulder, Drainage, Humans, Female, Middle Aged, Anti-Bacterial Agents, Shoulder Joint, Staphylococcal Infections, Debridement, Follow-Up Studies, Staphylococcus epidermidis, Methicillin-resistant Staphylococcus aureus
Introduction
According to reports, 4–10 persons out of every 100 000 develop septic arthritis each year, with some areas experiencing higher incidences of up to 29 cases per 100 000 individuals, and the number is increasing annually [1]. Septic arthritis of the shoulder is rare compared to that of the knee and hip joints, accounting for 5–12% of all cases of septic arthritis [2,3]. Delayed or inadequate treatment may result in joint destruction and a fatality rate of approximately 11%. Furthermore, if the infection spreads to multiple joints, the fatality rate reaches approximately 50% [4]. Given the important role the shoulder joint plays in daily activities, inappropriate treatment of septic arthritis may lead to considerable functional impairment and a high mortality rate [5].
Septic arthritis of the shoulder requires early diagnosis and treatment. Invasive treatment within 2 weeks of onset of the infection has yielded favorable results [6]. Effective treatment methods include intravenous administration of antibiotics, curettage of localized foci of infection, and debridement and drainage [7]. However, it often becomes refractory in high-risk cases, such as in diabetes mellitus, in patients on long-term dialysis, and in cases caused by antibiotic-resistant bacteria. Recently, the efficacy of continuous local antibiotic perfusion (CLAP) for bone and soft tissue infections has been reported [8–14]. In this study, we present a case of a patient undergoing long-term hemodialysis for congenital anomalies of the kidney and urinary tract who developed methicillin-resistant coagulase-negative
Case Report
INTRAOPERATIVE FINDINGS:
Immediately after the diagnosis, we performed irrigation and debridement of the joint using an arthroscope. Intraoperative findings revealed hemorrhage in both the glenohumeral joint and subacromial bursa, with marked hyperplasia and degeneration of the synovial membrane. For abscesses outside the joint, irrigation and debridement were performed under direct vision. After adequate irrigation and debridement, double-lumen drain with an anti-reflux valve (18Fr, 2 tubes in total) was placed for CLAP to allow for intra- and extra-articular antibiotic injection and drainage. A drain tube was inserted into the joint from the anterior portal made with skin incision for arthroscopic surgery. Also, due to the accumulation of an abscess from lateral to posterior of the humerus, the lateral deltoid muscle was split, and the other drain tube was placed at the posterior of the humerus (Figure 3). It has been reported that a minimal biofilm eradication concentration (MBEC), which is 100–1000 times the minimal inhibitory concentration (MIC), is needed to eradicate biofilms formed by bacteria [15]. Using CLAP, 2 mg/mL of aminoglycoside gentamicin, which is 1000 times the minimal inhibitory concentration (MIC <2 µg/mL), was administered at 2 mL/h. The risk of adverse effects, such as renal disorder and eighth cranial nerve disorder, increases when the minimum blood concentration of gentamicin exceeds 2 µg/mL. Also, it has recently been reported that the administration of high-concentration gentamicin affects the function of bone tissue-derived cells, although this was an in vitro study [16]. For these reasons, we performed therapeutic drug monitoring (TDM) after starting the administration of gentamicin, and the dosage was adjusted to maintain the blood concentration below 2 µg/mL. Vancomycin, which is sensitive to the bacterium, was intravenously administered systemically. The administration of vancomycin was initiated at 1 g/day, followed by alternate-day administration of 0.5 g. Thereafter, the dosage was adjusted while performing TDM of vancomycin.
POSTOPERATIVE COURSE:
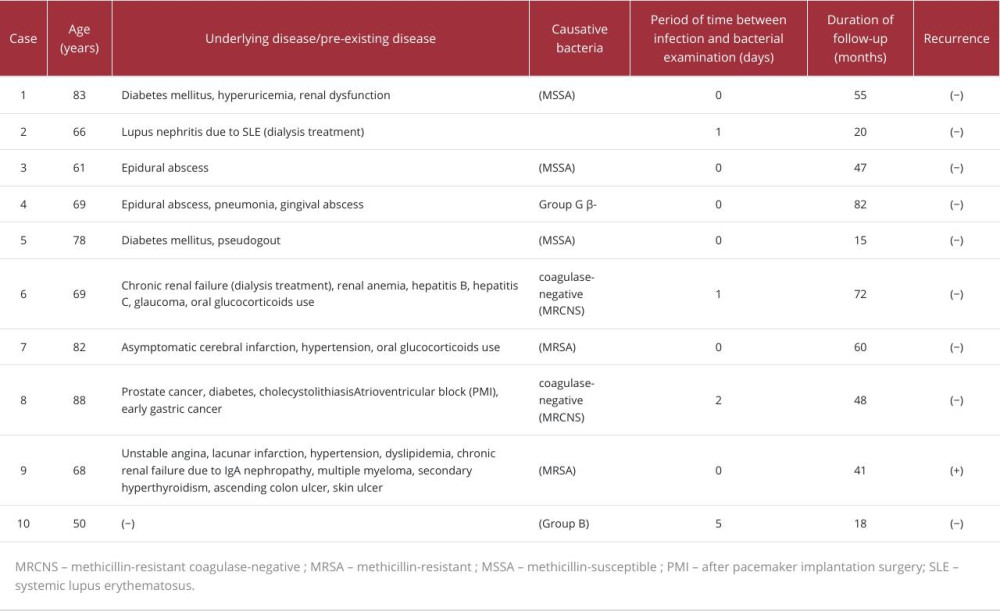
Among the 10 cases of septic arthritis of the shoulder with open drainage treated at our hospital (Table 1), remission was achieved in 9 cases. However, in 1 patient who was undergoing long-term dialysis and underwent reoperation, a relapse of septic arthritis of the shoulder caused by methicillin-resistant Staphylococcus aureus (MRSA) occurred. Therefore, CLAP was administered to this patient, who was at high risk of recurrence. Approximately 3 weeks after surgery, the CRP level decreased to 0.26 mg/dl. Thereafter, CLAP was discontinued 4 weeks after the operation because the blood CRP level was maintained at ≤0.3 mg/dL, and oral antibiotics (sulfamethoxazole trimethoprim) were subsequently administered 5 weeks after the operation. Infectious symptoms disappeared after CLAP, and bacterial culture was negative. There were no recurrent symptoms during follow-up and no complications such as acute renal failure, ototoxicity, or allergic or hypersensitivity reactions. In this case, no bone destruction was observed and there was no relapse 2 years after the infection subsided. Moreover, although the patient originally had a rotator cuff tear, no remarkable limitations on the range of motion were oserved. Therefore, the range of motion returned to that before the onset of infection, and there were no impediments to activities of daily life.
Discussion
In patients with septic arthritis of the shoulder, intravenously administered antibiotics are not easily transferred to the focus of infection due to poor blood flow at the focus. Furthermore, bacteria in the focus of bone infections tend to form biofilms, and it is particularly difficult for antibiotics to reach the bacteria that grow in the focus. CLAP can continuously inject and perfuse antibiotics directly into the focus, making it possible to locally transfer high concentrations of antibiotics that are effective in suppressing biofilms [13,14]. The present case was a compromised host with an MRCNS infection, indicating a high possibility of infection recurrence. However, the disease subsided as a result of irrigation debridement and CLAP, with no recurrence for at least 2 years after the surgery.
Early diagnosis and treatment are crucial in septic arthritis. In this case, the patient had a rotator cuff tear, and was a compromised host with localized swelling and fluid accumulation. Therefore, puncture was performed as soon as possible, and MRCNS was observed in the aspirate culture, enabling early diagnosis. Septic arthritis of the shoulder is often associated with a rotator cuff tear. Therefore, vigilance is required because the infection may be overlooked as a symptom associated with a rotator cuff tear, particularly if the infection is mild [17]. In addition to visual inspection and palpation, when joint fluid accumulation is observed, it is necessary to perform joint fluid tests in addition to blood tests.
Treatment of septic arthritis is based on early debridement of the infected focus and intravenous administration of antibiotics [3,6,18,19]. In recent years, although arthroscopic surgery has been reported [20], both direct arthrotomy and arthroscopic surgery have been reported to achieve favorable results [7,21]. There is currently no consensus regarding which treatment method is better [18]. Postoperative drainage methods include continuous perfusion, closed drainage, and open drainage using a Penrose drain. Of these, open drainage after arthroscopic irrigation debridement has been reported to have a favorable functional prognosis because of the advantage that rehabilitation can be started from the early postoperative period [22]. However, when the infection is caused by an antibiotic-resistant bacterium such as MRSA, the recurrence rate of infection is high, with approximately 60% being considered refractory [23].
In recent years, CLAP demonstrated efficacy against infected foci and can also be effective against resistant bacteria when high concentrations of antibacterial agents are administered. Furthermore, high-concentration antibiotics at 100–1000 times the MIC are required to eliminate bacteria within biofilms [15]. For injectable antibiotics, genes for aminoglycoside-inactivating enzymes have been identified [24]. It is recommended to select a high concentration of aminoglycosides because it can suppress infection regardless of drug susceptibility by achieving localized concentrations that exceed the resistance function of the inactivating enzyme [13]. Similarly, the use of high-concentration gentamicin, an aminoglycoside antibiotic, in this case, resulted in early remission of the infection.
Currently, open drainage after irrigation and debridement of the lesion is performed for septic arthritis. Open drainage is believed to reduce functional impairment because it facilitates early initiation of rehabilitation [22]. On the other hand, for CLAP, which was performed in the current case, range of motion training was not performed for a while after surgery. In septic arthritis of the shoulder complicated with a rotator cuff tear, as in this case, strong functional impairment may remain after the infection subsides because of the spread of infection to surrounding tissues, degeneration and functional decline, as well as the expansion of rupture area due to combined debridement [2]. However, in the current case, the infection subsided soon after CLAP. Subsequent rehabilitation proceeded smoothly; hence, no serious functional impairments remained, and no impediments to activities of daily life persisted 2 years after the surgery.
Conclusions
CLAP may be considered as an effective therapeutic option for septic arthritis of the shoulder that can alleviate the infection at an early stage, enable early rehabilitation, and thereby reduce the risk of functional deficits.
Figures
References:
1.. Bovonratwet P, Fu MC, Pathak N, Surgical treatment of septic shoulders: A comparison between arthrotomy and arthroscopy: Arthroscopy, 2019; 35; 1984-91
2.. Leslie BM, Harris JM, Driscoll D, Septic arthritis of the shoulder in adults: J Bone Joint Surg Am, 1989; 71; 1516-22
3.. Stutz G, Kuster MS, Kleinstück F, Gächter A, Arthroscopic management of septic arthritis: Stages of infection and results: Knee Surg Sports Traumatol Arthrosc, 2000; 8; 270-74
4.. Mathews CJ, Weston VC, Jones A, Bacterial septic arthritis in adults: Lancet, 2010; 375; 846-55
5.. Jiang JJ, Piponov HI, Mass DP, Septic arthritis of the shoulder: A comparison of treatment methods.: J Am Acad Orthop Surg., 2017; 25; e175-e84
6.. Klinger HM, Baums MH, Freche S, Septic arthritis of the shoulder joint: An analysis of management and outcome.: Acta Orthop Belg, 2010; 76; 598-603
7.. Stone MA, Henry TW, Gutman MJ, Surgical treatment of shoulder infection following rotator cuff repair: Arch Bone Jt Surg, 2023; 11; 111-16
8.. Takahashi H, Koda M, Funayama T, Continuous local antibiotic perfusion for patients with surgical site infection after instrumented spinal surgery; A novel technique to retain the implants: J Clin Neurosci, 2021; 93; 70-74
9.. Oe K, Maruo A, Fukui T, Treatment of chronic osteomyelitis of the femur by intramedullary antibiotic perfusion (iMAP): A case report: J Orthop Case Rep, 2021; 11; 35-38
10.. Takahara S, Maruo A, Takayama H, Harada T, Continuous local antibiotics perfusion therapy for acute deep infections after open fractures.: Case Rep Orthop., 2022; 2022; 2563939
11.. Iwamoto K, Yamamoto N, Saiga K, Prosthetic joint infection after total talar replacement: An implant-retained case treated with combined continuous local antibiotic perfusion (CLAP).: J Orthop Sci, 2024; 29(1); 349-53
12.. Maruo A, Oda T, Mineo R, Continuous local antibiotic perfusion: A treatment strategy that allows implant retention in fracture-related infections.: J Orthop Surg (Hong Kong)., 2022; 30(2) 10225536221111902
13.. Kosugi K, Zenke Y, Sato N, Potential of continuous local antibiotic perfusion therapy for fracture-related infections.: Infect Dis Ther, 2022; 11; 1741-55
14.. Himeno D, Matsuura Y, Maruo A, Ohtori S, A novel treatment strategy using continuous local antibiotic perfusion: A case series study of a refractory infection caused by hypervirulent Klebsiella pneumoniae: J Orthop Sci, 2022; 27(1); 272-80
15.. Ceri H, Olson ME, Stremick C, The Calgary Biofilm Device: New technology for rapid determination of antibiotic susceptibilities of bacterial biofilms: J Clin Microbiol, 1999; 37; 1771-76
16.. Yamamoto Y, Fukui T, Sawauchi K, Effects of high antibiotic concentrations applied to continuous local antibiotic perfusion on human bone tissue-derived cells: Bone Joint Res, 2024; 13(3); 91-100
17.. Sobreira D, Souza Nd, Almeida JI, Septic arthritis and arthropathy of the rotator cuff: remember this association: Rev Bras Ortop, 2016; 51(4); 444-48
18.. Jeon IH, Choi CH, Seo JS, Arthroscopic management of septic arthritis of the shoulder joint: J Bone Joint Surg Am, 2006; 88; 1802-6
19.. Goetti P, Gallusser N, Antoniadis A, Advanced septic arthritis of the shoulder treated by a two-stage arthroplasty: World J Orthop, 2019; 10; 356-63
20.. Abdel MP, Perry KI, Morrey ME, Arthroscopic management of native shoulder septic arthritis: J Shoulder Elbow Surg, 2013; 22; 418-21
21.. Kirchhoff C, Braunstein V, Buhmann Kirchhoff S, Stage-dependant management of septic arthritis of the shoulder in adults: Int Orthop, 2009; 33; 1015-24
22.. Costales C, Butler-Wu SM, A real pain: Diagnostic quandaries and septic arthritis.: J Clin Microbiol., 2018; 56; e01358-17
23.. Takahashi R, Kajita Y, Harada Y, Factors affecting the outcome of septic arthritis of the shoulder joint with arthroscopic management.: J Orthop Sci, 2021; 26; 381-84
24.. Lyon BR, Skurray R: Microbiol Rev, 1987; 51; 88-134
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133