20 August 2024: Articles 
Acute Abdominal Crisis in Type A Hemophilia: Unraveling Retroperitoneal Hematoma: A Case Report
Unusual clinical course, Challenging differential diagnosis, Management of emergency care
Hisham A. Althobaiti1ACE, Bahjat F. Alabou Houseen2ACE, Eyad M. Alsaqqa3ABE, Abdulhameed Fouad SarriyahDOI: 10.12659/AJCR.944694
Am J Case Rep 2024; 25:e944694






Abstract
BACKGROUND: Classical hemophilia A, an X-linked recessive disorder, is characterized by an inability to produce factor VIII in normal quantities. This condition, also leading to factor IX deficiency, underpins the bleeding disorder known as hemophilia A. Among the complications of this illness, spontaneous retroperitoneal hematoma is rare but can be associated with congenital coagulopathies such as von Willebrand disease or hemophilia A. This type of spontaneous internal bleeding has been the subject of a limited number of studies.
CASE REPORT: A 38-year-old man with a known diagnosis of hemophilia A presented to the Emergency Department exhibiting acute pain in the right lower abdomen. A computed tomography scan of the abdomen identified a right-sided retroperitoneal mass, suspected to be a hematoma. Within 7 h after admission, the patient experienced significant drops in the hemoglobin level and platelet count. He was administered packed red blood cells, fresh frozen plasma, and platelet transfusions prior to transfer to the Intensive Care Unit. There, he was treated with factor VIII and recombinant factor VIIa, coupled with stringent monitoring. Following clinical and laboratory findings and stabilization, he was discharged with specific medications, and a follow-up appointment was scheduled.
CONCLUSIONS: Spontaneous retroperitoneal hematoma in patients with hemophilia A is a rare and grave emergency. This case underscores the need for precise diagnostic approaches, tailored management strategies, and vigilant surveillance to prevent and mitigate the potentially life-threatening complications associated with spontaneous hemorrhage in this population.
Keywords: Hematoma, Hemophilia A, Retroperitoneal Space, hemostatic disorders, Blood Coagulation Factors, Factor VIII, adult, Humans, Male, Abdomen, Acute, Tomography, X-Ray Computed
Introduction
Classical hemophilia, known as hemophilia A, is a sex-linked recessive disorder characterized by the failure to synthesize factor VIII in normal proportions that is inherited as a recessive trait. While spontaneous mutations account for nearly 20% of cases, the incidence of this condition ranges from approximately 1 in 10 000 to 1 in 15 000 individuals within the population. The clinical manifestations of hemophilia A exhibit considerable variability, with the severity closely tied to the degree of factor VIII deficiency [1]. Hemophilia A entails a deficiency of coagulation factors leading to compromised hemostasis [1]. Consequently, spontaneous bleeding occurs, varying in frequency and severity based on the plasma level of factor VIII, as follows: (1) Mild deficiency (5–40% FVIII activity) typically manifests as bleeding post-surgical procedures; (2) moderate deficiency (1–5% FVIII activity) presents with intermediate bleeding tendencies; and (3) severe deficiency (<1% FVIII activity) is marked by frequent spontaneous bleeding, often causing progressive joint damage.
Inherited bleeding disorders, such as hemophilia A and B, are characterized by deficiencies in factor VIII and factor IX, respectively. Patients with severe forms of these conditions, in which levels of endogenous clotting factors drop below 1%, have a high risk of experiencing hemorrhaging in different parts of the body, including the joints, muscles, soft tissues, central nervous system, or genitourinary tract [1,2]. Numerous risk factors contribute to the development of hemophilia A, such as mutations in the FVIII gene. Predominant errors in severe hemophilia A involve intron 22 and intron 1 inversions, found in 30% to 50% and 2% to 5% of severe cases, respectively. Additionally, a family history of inhibitors suggests a shared mutation among affected family members [3]. Recent studies have explored environmental factors influencing inhibitor formation in hemophilia A. Variables such as the type of FVIII product, age at initial treatment, treatment intensity, and signals from surgeries, severe bleeding, vaccinations, and infections have been scrutinized to understand their impact on inhibitor development risk [4]. Severe joint bleeding stands out as the most common symptom in individuals affected by hemophilia A. Essential management involves replacement therapy with FVIII or FIX to effectively control bleeding episodes [1,2].
Retroperitoneal hemorrhage involves blood accumulation in the retroperitoneal area and is a rare and challenging condition to precisely gauge, due to its diverse causes and presentations [5,6]. Spontaneous retroperitoneal hemorrhage, although infrequent, can be associated with congenital coagulation disorders such as von Willebrand disease and type A and type B hemophilia, yet it remains understudied [7,8]. The diagnosis can be delayed because the retroperitoneum serves as a noncompressible area where a large amount of blood can accumulate rapidly without causing obvious stigmata of an underlying expanding hematoma [9]. Diagnosing retroperitoneal hematoma is particularly tricky after abdominal blunt trauma, necessitating suspicion in patients exhibiting signs of hemorrhagic shock without an apparent bleeding source [10]. Early symptoms often include nausea, anorexia, and generalized abdominal pain, with signs of hypovolemic shock manifesting later [7]. Traumatic retroperitoneal hematoma rates range widely, from 18% to 60%, following pelvic or abdominal trauma [8]. Other causes encompass ruptures of retroperito-neal organs, drug-related bleeding tendencies, tumors in the kidneys or adrenal glands, and vascular aneurysms, as well as iatrogenic and idiopathic origins [11,12].
In severe hemophilia cases, activities such as coughing can trigger retroperitoneal bleeding due to intra-abdominal muscle sheath strain [13–15]. Notably, about 23% to 33% of patients with severe type A hemophilia develop significant inhibitor levels after multiple coagulation factor VIII replacement therapies [16,17]. The treatment of hemophilia patients with inhibitors focuses on controlling bleeding and neutralizing inhibitors. Recombinant factor VIIa (rFVIIa), which stimulates thrombin generation and stable fibrin clot formation, has emerged as a pivotal treatment in recent years, especially in severe type A hemophilia with inhibitors [16,18]. Typical doses of active rFVIIa range from 90 µg/kg every 2 to 4 h, while a single high dose of 270 µg/kg is also considered effective and safe during bleeding episodes in hemophilia A or B [19,20].
Case Report
A 38-year-old man with a known history of hemophilia A since birth, currently on factor VII replacement therapy (3000 IU every 12 h during bleeding episodes), presented to the Emergency Department with acute abdominal pain. The pain, which started abruptly, localized to the right lower quadrant, had a cramping nature, and was rated as highly intense, at 9/10. It was exacerbated by motion, particularly when lying supine, failed to subside with any interventions, and had no relationship to food intake. The patient experienced no concurrent symptoms, such as vomiting, nausea, changes in bowel habits, flank pain, dysuria, or abdominal distension. It was noteworthy that there were no external signs of bruising, ecchymosis, hematemesis, melena, hemarthrosis, or recurrent hematoma formation, nor any indications of bleeding from the oral mucosa or epistaxis. No recent trauma or history of anticoagulant or antiplatelet use was reported. His surgical history was notable for an appendectomy 15 years prior, in which factor VIII was administered. Since then, factor VIII use was limited to instances of severe illness, dental work, crush injuries, or trauma. The patient had no drug or food allergies and no history of blood transfusion or chronic drug use.
Among his siblings, 3 out of 5 sisters were carriers of hemophilia A, whereas he was the only brother affected by the condition. There was no reported family history of malignancy. The patient was a father to 2 daughters, who were both carriers of hemophilia A, with no consanguinity noted within the family. The patient abstained from smoking and alcohol.
On physical examination at admission, the patient was conscious, alert, and oriented. He showed physical signs of pallor in the palmar creases and conjunctiva, but no jaundice or cyanosis was present. His body weight was 85 kg, and his height was 179 cm, giving him a body mass index of 26.5 kg/m2. He appeared comfortable when resting in bed and was already connected to an intravenous (i.v.) line. Vital signs showed stability: blood pressure was 118/78 mm Hg with no orthostatic changes, pulse rate was 92 beats/min, respiratory rate was 18 breaths/min, temperature was normal at 37°C, and oxygen saturation remained at 96% while breathing room air.
Laboratory values upon presentation to the Emergency Department, 7 h after admission, and after transfusion are displayed in Tables 1–3, respectively.
The abdominal examination revealed no distension; however, ecchymosis was observed at the right iliac fossa. Palpation and percussion identified tenderness in the right lower quadrant, without any signs of abdominal wall venous distention, internal bleeding indicated by a Cullen or Grey Turner sign, or abnormal fluid accumulation suggestive of ascites. Bowel sounds remained normal. A complete blood count upon admission indicated a white blood cell count of 10.8×109/L, hemoglobin level of 12.0 g/dL, mean corpuscular volume of 84.9 fL, mean corpuscular hemoglobin of 29.4 pg, hematocrit of 34.7%, and a platelet count of 266×109/L. The severe abdominal pain necessitated a delay in the initial plan for an urgent computed tomography (CT) scan of the abdomen and pelvis with contrast. Analgesic management included i.v. paracetamol (1 g), tramadol (100 mg), and a loading dose of factor VIII (3400 IU). The subsequent CT scan identified a right-sided retroperitoneal mass lesion, measuring approximately 8.5×13×15 cm, displacing the caecum and right kidney medially (Figure 1). Contrast extravasation observed during the venous phase suggested active bleeding. Additionally, fluid collections in the pelvic, perinephric, peritoneal reflection, and perihepatic regions indicated a probable retroperitoneal hematoma with ongoing hemorrhage.
After the patient was transferred to the regular ward, maintenance dosing of factor VIII (1700 IU every 12 h) and i.v. Ringer lactate (60 mL/h) were commenced. With a decline in vital signs and hematological parameters, the factor VIII dosage was escalated to 4400 IU i.v. every 8 h, with a concurrent increase of the Ringer lactate infusion to 100 mL/h. Transfusions of 6 units of packed red blood cells, 4 units of fresh frozen plasma, and 4 units of platelets were administered due to the falling hemoglobin levels and platelet count. Surgical consultation deemed acute intervention unnecessary, and the patient was transferred to the Intensive Care Unit. There, a stat dose of recombinant factor VIIa (5 mg i.v. infusion) was given. Subsequent ultrasound assessments at 5 and 12 days after admission revealed a heterogeneous retroperitoneal hematoma with minimal displacement of the right kidney. Initially, the hematoma measured 12×10×12 cm, and upon later examination, it measured 14×9×9 cm (Figure 2). These findings led to a reduction in the factor VIII dosage. Because arterial embolization was unavailable at our facility, a transfer to a higher level center was considered if the patient’s condition failed to stabilize with medical management. Following 2 days of stable clinical and laboratory findings in the Intensive Care Unit, the patient was transferred to the general ward. There, he received factor VIII (3000 IU every 12 h for 5 days), i.v. paracetamol at a dosage of 1 g 3 times daily (subsequently switched to oral administration), and omeprazole 20 mg orally once daily. After a 10-day stay in the general ward, marked by considerable clinical improvement, the patient was discharged home. He was given a follow-up appointment within 1 week and instructions to seek immediate emergency care should he experience new abdominal pain or bleeding from any site.
Discussion
Hemophilia A and B are genetic disorders that impair the normal clotting function of blood, resulting in an increased tendency for prolonged and persistent bleeding. Individuals with these conditions face challenges in halting or managing bleeding events, due to deficiencies in specific clotting factors. These deficiencies can lead to significant complications, as even minor injuries can result in substantial and hard-to-control bleeding [1]. In our report, a patient with a known case of hereditary hemophilia A presented with acute abdominal pain and signs of active bleeding in the retroperitoneal region. This incident led to a significant drop in hemoglobin levels and hemodynamic instability. Despite the absence of acute surgical intervention, the patient received comprehensive treatment. The use of FVIII infusion, recombinant activated FVII therapy, and transfusions of packed fresh frozen plasma, red blood cells, and platelets collectively contributed to a successful conservative management approach, resulting in a favorable clinical outcome.
To manage bleeding episodes in individuals with hemophilia, it is necessary to use replacement therapy involving FVIII or FIX [1,2]. Gastrointestinal bleeding is a common complication in individuals with hemophilia, with an estimated occurrence rate ranging from 10% to 25%. The literature reports instances of intramural hematoma within the gastrointestinal tract, which primarily occurs in the small intestine, stomach, esophagus, and colon [21]. One predominant mechanism involves the potential rupture of terminal arteries, as they penetrate the muscle layer within the intestinal wall. This type of bleeding results in a separation between the muscularis mucosae and muscle layers while still maintaining viability of the mucosal lining [22].
Non-surgical medical interventions form the initial approach for managing intramural gastrointestinal hematomas. Surgical options are reserved for cases suspected to have complications such as intra-abdominal hemorrhage, perforation, intestinal ischemia, peritonitis, or untreatable obstruction [23]. Treatment strategies encompass intestinal rest, nasogastric decompression, correction of electrolyte imbalances, and maintaining factor VIII levels above 80% in the acute phase [24,25]. Studies such as the one by Tani et al report that transarterial embolization demonstrates effectiveness in achieving hemostasis in cases of spontaneous retroperitoneal hematoma [24].
Close monitoring and adjunctive therapy with recombinant factor VIIa aided in stabilizing the patient’s condition. Subsequent ultrasound examinations depicted a stationary course of the retroperitoneal hematoma size, prompting a gradual reduction in factor VIII dosage over the hospitalization course. Empirical embolization around the hematoma site, even when the bleeding origin is not identified, might effectively halt life-threatening bleeding [26]. In cases of intra-abdominal hemorrhage due to arterial bleeding, the mortality rate is reported at 8.6%. However, if the bleeding site remains unidentified, this rate could escalate to 50% [27].
Conclusions
This case underscores the complexity of treating retroperito-neal hematomas in individuals with hemophilia A, highlighting the necessity for treatment strategies tailored to the patient’s specific needs as well as meticulous monitoring to avert life-threatening complications from spontaneous bleeding events. Retroperitoneal hematoma in patients with hemophilia A represents a rare and critical emergency. In the present case, diagnosis hinged on the patient’s medical history, physical examination findings, and radiological evaluations, which enabled successful conservative treatment. Given the potential for high mortality associated with spontaneous retroperitoneal hematomas, systematic and thorough monitoring is essential for effective management and treatment.
Figures
References:
1.. Delibegovic M, Alispahic A, Gazija J, Intramural haemorrhage and haematoma as the cause of ileus of the small intestine in a haemophiliac: Med Arch, 2015; 69(3); 206-7
2.. Ramadan KM, Lowry JP, Wilkinson A, Acute intestinal obstruction due to intramural haemorrhage in small intestine in a patient with severe haemophilia A and inhibitor: Eur J Haematol, 2005; 75(2); 164-66
3.. Ghosh K, Shetty S, Immune response to FVIII in hemophilia A: An overview of risk factors: Clin Rev Allergy Immunol, 2009; 37(2); 58-66
4.. Garagiola I, Palla R, Peyvandi F, Risk factors for inhibitor development in severe hemophilia A: Thromb Res, 2018; 168; 20-27
5.. Farouque HM, Tremmel JA, Raissi Shabari F, Risk factors for the development of retroperitoneal hematoma after percutaneous coronary intervention in the era of glycoprotein IIb/IIIa inhibitors and vascular closure devices: J Am Coll Cardiol, 2005; 45(3); 363-68
6.. Mondie C, Maguire NJ, Rentea RM, Retroperitoneal hematoma: StatPearls, 2023, Treasure Island (FL), StatPearls Publishing
7.. Selivanov V, Chi HS, Alverdy JC, Morris JA, Sheldon GF, Mortality in retroperitoneal hematoma: J Trauma, 1984; 24(12); 1022-27
8.. Wang F, Wang F, The diagnosis and treatment of traumatic retroperitoneal hematoma: Pak J Med Sci, 2013; 29(2); 573-76
9.. Sajnani N, Bogart DB, Retroperitoneal hemorrhage as a complication of percutaneous intervention: Report of 2 cases and review of the literature: Open Cardiovasc Med J, 2013; 7; 16-22
10.. Sharp KW, Spees EK, Selby LR, Diagnosis and management of retroperitoneal hematomas after femoral vein cannulation for hemodialysis: Surgery, 1984; 95(1); 90-95
11.. Monib S, Ritchie A, Thabet E, Idiopathic retroperitoneal hematoma: J Surg Tech Case Rep, 2011; 3(1); 49-51
12.. Won DY, Kim SD, Park SC, Abdominal compartment syndrome due to spontaneous retroperitoneal hemorrhage in a patient undergoing anticoagulation: Yonsei Med J, 2011; 52(2); 358-61
13.. Daliakopoulos SI, Bairaktaris A, Papadimitriou D, Pappas P, Gigantic retroperitoneal. hematoma as a complication of anticoagulation therapy with heparin in therapeutic doses: A case report: J Med Case Rep, 2008; 2; 162
14.. Ylmaz S, Oren H, Irken G, Life-threatening mediastinal-retroperito-neal hemorrhage in a child with moderate hemophilia A and high inhibitor titer: Successful management with recombinant activated factor VII: J Pediatr Hematol Oncol, 2005; 27(7); 400-2
15.. Aronstam A, McLellan DS, Turk P, Transfusion requirements of adolescents with severe haemophilia A: J Clin Pathol, 1979; 32(9); 927-30
16.. Wight J, Paisley S, The epidemiology of inhibitors in haemophilia A: A systematic review: Haemophilia, 2003; 9(4); 418-35
17.. White GC, Rosendaal F, Aledort LM, Definitions in hemophilia. Recommendation of the scientific subcommittee on factor VIII and factor IX of the scientific and standardization committee of the International Society on Thrombosis and Haemostasis: Thromb Haemost, 2001; 85(3); 560
18.. Lawrence JS, Johnson JB, The presence of a circulating anti-coagulant in a male member of a hemophiliac family: Trans Am Clin Climatol Assoc, 1941; 57; 223-31
19.. Craddock CG, Lawrence JS, Hemophilia; A report of the mechanism of the development and action of an anticoagulant in two cases: Blood, 1947; 2(6); 505-18
20.. Frommeyer WB, Epstein RD, Taylor FH, Refractoriness in hemophilia to coagulation-promoting agents: Whole blood and plasma derivatives: Blood, 1950; 5(5); 401-20
21.. Prieto HM, Perez CP, Bermejo JM, Intramural hematoma of the small intestine in a patient with severe hemophilia A. Case report and review of the literature: J Gastrointest Dig Syst, 2015; 5(363); 2
22.. Nakayama Y, Fukushima M, Sakai M, Intramural hematoma of the cecum as the lead point of intussusception in an elderly patient with hemophilia A: Report of a case: Surg Today, 2006; 36(6); 563-65
23.. Sorbello MP, Utiyama EM, Parreira JG, Spontaneous intramural small bowel hematoma induced by anticoagulant therapy: Review and case report: Clinics (Sao Paulo), 2007; 62(6); 785-90
24.. Kouides PA, Fogarty PF, How do we treat: Upper gastrointestinal bleeding in adults with haemophilia [published correction appears in Haemophilia.2010;16(2): 413]: Haemophilia, 2010; 16(2); 360-62
25.. Srivastava A, Brewer AK, Mauser-Bunschoten EP, Guidelines for the management of hemophilia: Haemophilia, 2013; 19(1); e1-e47
26.. Tani R, Sofue K, Sugimoto K, The utility of transarterial embolization and computed tomography for life-threatening spontaneous retroperito-neal hemorrhage: Jpn J Radiol, 2019; 37(4); 328-35
27.. Reilly EF, Blansfield JA, Zebley DM, Spontaneous colonic mesenteric hemorrhage: Report of an unusual case of abdominal apoplexy: Dis Colon Rectum, 2005; 48(7); 1484-86
Figures
Tables
 Table 1.. Laboratory findings upon admission to the Emergency Department.
Table 1.. Laboratory findings upon admission to the Emergency Department.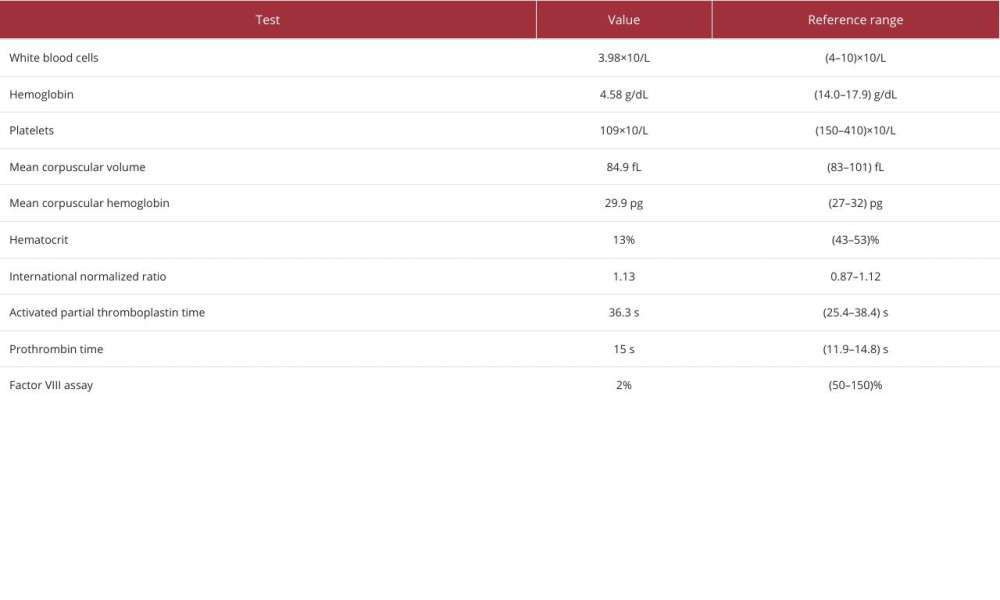 Table 2.. Laboratory findings 7 h after admission.
Table 2.. Laboratory findings 7 h after admission.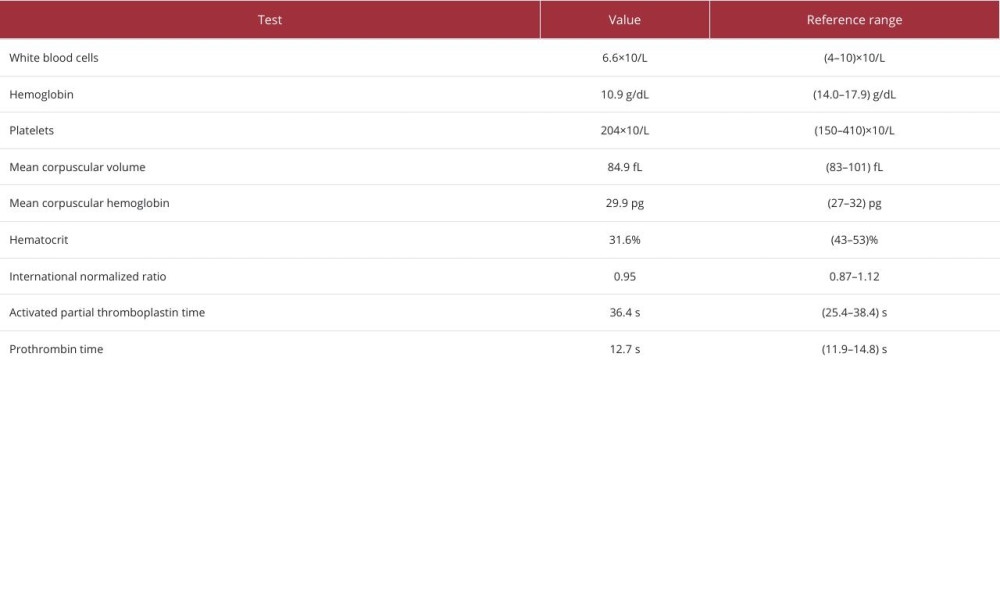 Table 3.. Laboratory findings after transfusion.Table 1.. Laboratory findings upon admission to the Emergency Department.Table 2.. Laboratory findings 7 h after admission.Table 3.. Laboratory findings after transfusion.
Table 3.. Laboratory findings after transfusion.Table 1.. Laboratory findings upon admission to the Emergency Department.Table 2.. Laboratory findings 7 h after admission.Table 3.. Laboratory findings after transfusion. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133