20 December 2025: Articles 
Ethambutol-Associated Thrombocytopenia: A Rare Case Report of Drug-Induced Platelet Decline in Tuberculosis Treatment
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Adverse events of drug therapy
Ugo FrançoiseDOI: 10.12659/AJCR.945090
Am J Case Rep 2025; 26:e945090






Abstract
BACKGROUND: Ethambutol is a first-line treatment for tuberculosis and a cornerstone of treatment for atypical mycobacteria. It is considered to have a low incidence of adverse drug reactions, compared with that of other anti-tuberculosis drugs. Apart from causing optic neuropathies, ethambutol is rarely implicated in the adverse effects of tuberculosis treatment.
CASE REPORT: We report the case of a 41-year-old man treated for cervical lymph node tuberculosis who developed ethambutol-induced thrombocytopenia. We reviewed the patient’s medical history to reconstruct the chronology of his treatment and to assess the causal relationship between ethambutol and the adverse event. Isolated thrombocytopenia was noticed 10 days after the start of antituberculous treatment, motivating the discontinuation of ethambutol, as the Mycobacterium tuberculosis strain had no resistance to other first-line antituberculosis drugs. The platelet count nadir of 72×10⁹/L was observed 48 hours after ethambutol discontinuation, after 3 weeks of treatment. Discontinuation of ethambutol alone led to a rapid recovery of the platelet count within 5 days. Despite the absence of drug reintroduction, the Naranjo causality score was +6, indicating that ethambutol was probably responsible for the adverse event. We discussed this case in relation to previously reported cases, and our findings were consistent with the only 2 cases documented in the literature.
CONCLUSIONS: Ethambutol can cause thrombocytopenia, which occurs within 2 weeks of its introduction and disappears within days of its discontinuation.
Keywords: Drug-Related Side Effects and Adverse Reactions, Ethambutol, Mycobacterium tuberculosis, Thrombocytopenia, Humans, Male, adult, Antitubercular Agents, Tuberculosis, Lymph Node, Platelet Count
Introduction
Ethambutol (EMB), in combination with isoniazid, rifampin, and pyrazinamide, is recommended during the initial treatment of tuberculosis (TB) pending susceptibility results, particularly to limit the selection of isoniazid-resistant bacteria in cases of rifampin-resistant strains [1]. EMB is also a cornerstone for the treatment of atypical mycobacteria and is considered the best companion drug for preventing the emergence of macrolide resistance [2]. Apart from ocular and occasional cutaneous reactions, EMB is seldom associated with toxicity [3]. We report a case of EMB-induced thrombocytopenia in a patient with lymph node TB requiring discontinuation of the drug.
Case Report
A 41-year-old man presented to Cayenne Hospital in July 2023 with a progressive enlargement of cervical lymph nodes that had been present since April. He arrived in French Guiana in January 2023, following a 2-year migration from Afghanistan. His medical history included pulmonary TB, treated for only 2 months, 20 years earlier, without any reported adverse effects. He also had hypertension, renal colic, and stage 5 chronic kidney disease (CKD) [4]. He did not report any drug allergy. His treatment consisted of darbepoetin alfa 100 μg subcutaneously once weekly, amlodipine 10 mg/day, pantoprazole 40 mg twice daily, sevelamer 800 mg 3 times daily, folic acid, polystyrene sulfonates, ferrous sulfate, calcium, and sodium bicarbonate. Physical examination revealed bilateral basilar cervical lymph nodes that were soft, tender to palpation, up to 6 cm in maximum diameter, and not adherent to the skin or deep tissues.
During follow-up on August 31 (DantiTB 12), a significant reduction in cervical lymph nodes was noted, confirming good treatment compliance. The patient reported the onset of pruritic papules on the lateral surfaces of the fingers beginning August 26 (DantiTB 7). He self-medicated with cetirizine and prednisone (1 mg/kg) on August 30. Dyshidrotic eczema was considered the most likely diagnosis, and systemic corticosteroids and cetirizine were discontinued. Blood test results on August 28 (DantiTB 10) were stable. On September 8 (DantiTB 20), the patient reported improvement of his skin lesions and good compliance and clinical tolerability of the anti-TB treatment. However, on September 4 (DantiTB 16), he developed thrombocytopenia, with a platelet count 120×109/L, confirmed by blood smear and a second blood test performed on September 6 showing a platelet count of 86×109/L. He did not report headache, fever, or other concomitant events suggesting a concomitant viral infection. Therefore, given the patient’s geography and good clinical outcome after 3 weeks of appropriate treatment, our estimate of the probability of isoniazid resistance was low. Given the described, albeit rare, cases of EMB-induced thrombocytopenia, we decided to stop EMB on September 9 (DantiTB 21, Dstop 0) but maintain the same regimen otherwise. In September, the patient presented to the Emergency Department with hypertensive pulmonary edema and suspected acute coronary syndrome, due to chest pain, elevated troponin levels, and electrocardiographic abnormalities. He was admitted to the Intensive Care Unit and received isosorbide dinitrate, furosemide, and lercanidipine for pulmonary edema, and aspirin, clopidogrel, and unfractionated heparin for suspected coronary syndrome. Thrombocytopenia stabilized between 72 and 108×109/L on September 11 (DantiTB 23, Dstop 2). Coronary syndrome was eventually ruled out, and the final diagnosis was acute pulmonary edema secondary to hypervolemia with ion imbalance. On September 14 (DantiTB 26, Dstop 5), the patient had a platelet count of 131×109/L. He was eventually discharged from the hospital on September 26 with a platelet count of 274×109/L, which had been maintained through the last follow-up on January 31, 2024.
Discussion
To the best of our knowledge, only 2 cases of thrombocytopenia secondary to EMB have been published [5,6]. In both reports, an isolated thrombocytopenia occurred within the first week of treatment, with no evidence of overdose. Discontinuation of EMB resulted in normalization of platelet levels within 1 week, which strongly supports drug toxicity caused solely by EMB. In the present case, given the antibiogram results, no EMB reintroduction test was performed. The Naranjo causality score was +6 (Figure 2), indicating that EMB was probably responsible for the adverse reaction [7]. In a reported case in which reintroduction was attempted, a rapid relapse occurred [6]. The mechanism of thrombocytopenia remains unknown. In 1 case [5], the authors suggested an immune mechanism. However, the rapid onset and normalization of thrombocytopenia suggests a toxic mechanism. Nevertheless, it is important to note that rifampin remains the most common cause of anti-TB treatment-related thrombocytopenia and should be the first consideration in cases of thrombocytopenia [8]. In our case, we suspected a sensitive strain (later confirmed by antibiogram) that does not require EMB in regions where drug-resistant TB is not endemic [9]. This allowed easy identification of EMB involvement without the need for sequential reintroduction. Of note, the dyshidrotic eczema may have been secondary to EMB, as its association with EMB has been suggested previously [10].
Conclusions
Although rare, EMB-induced thrombocytopenia appears to be a real phenomenon, occurring within the first 2 weeks of treatment and resolving rapidly after EMB discontinuation.
Figures
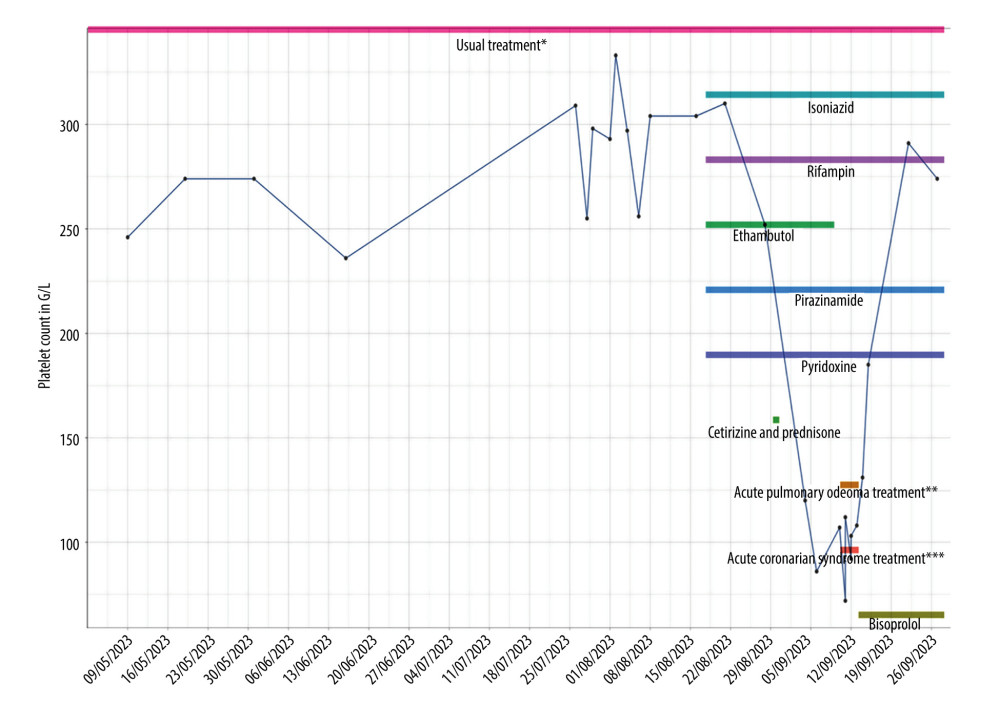 Figure 1. Medication and platelet count evolution. * Darbepoetin alfa, amlodipine, calcium, folic acid, pantoprazole, sodium bicarbonate, sevelamer, polystyrene sulfonates, and iron sulfate; ** Isosorbide dinitrate, furosemide, and lercanidipine; *** Aspirin, clopidogrel, and unfractionated heparin. G/L=×109/L.
Figure 1. Medication and platelet count evolution. * Darbepoetin alfa, amlodipine, calcium, folic acid, pantoprazole, sodium bicarbonate, sevelamer, polystyrene sulfonates, and iron sulfate; ** Isosorbide dinitrate, furosemide, and lercanidipine; *** Aspirin, clopidogrel, and unfractionated heparin. G/L=×109/L. 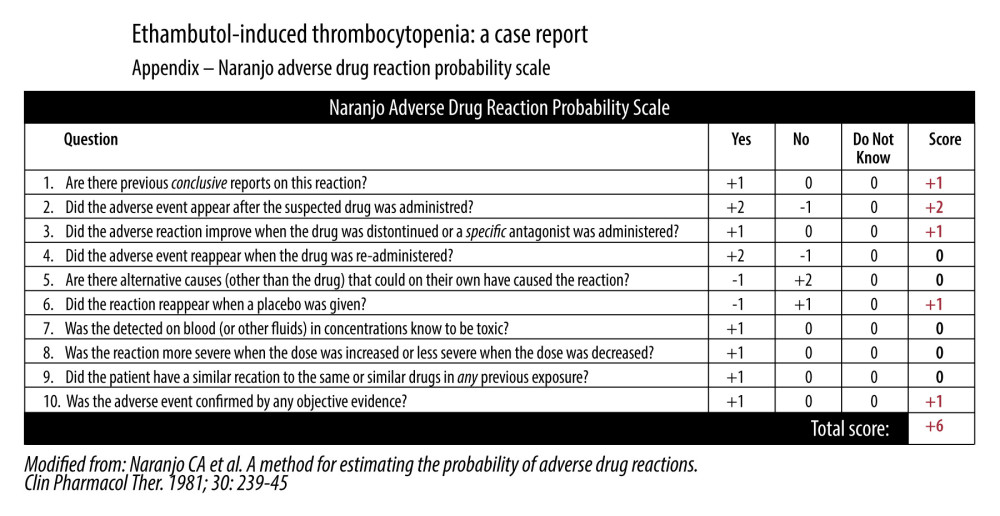 Figure 2. Naranjo adverse drug reaction probability scale.
Figure 2. Naranjo adverse drug reaction probability scale. References
1. : WHO consolidated guidelines on tuberculosis: Module 4: Treatment – Drug-susceptible tuberculosis treatment [Internet], 2022 Available from: https://pubmed.ncbi.nlm.nih.gov/35727905/
2. Daley CL, Iaccarino JM, Lange C, Treatment of nontuberculous mycobacterial pulmonary disease: An official ATS/ERS/ESCMID/IDSA clinical practice guideline: Eur Respir J, 2020; 56(1); 2000535
3. Forget EJ, Menzies D, Adverse reactions to first-line antituberculosis drugs: Expert Opin Drug Saf, 2006; 5(2); 231-49
4. Levey AS, Eckardt KU, Tsukamoto Y, Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO): Kidney Int, 2005; 67(6); 2089-100
5. Rabinovitz M, Pitlik SD, Halevy J, Rosenfeld JB, Ethambutol-induced thrombocytopenia: Chest, 1982; 81(6); 765-66
6. Prasad R, Mukerji PK, Ethambutol-induced thrombocytopaenia: Tubercle, 1989; 70(3); 211-12
7. Naranjo CA, Busto U, Sellers EM, A method for estimating the probability of adverse drug reactions: Clin Pharmacol Ther, 1981; 30(2); 239-45
8. Kaur A, Bhandari RK, Rohilla R, Anti-tubercular therapy (ATT) induced thrombocytopenia: A systematic review: Indian J Tuberc, 2023; 70(4); 489-96
9. De Castro N, Mechaï F, Bachelet DFAST TB Study Group, Treatment with a three-drug regimen for pulmonary tuberculosis based on rapid molecular detection of isoniazid resistance: A noninferiority randomized trial (FAST-TB): Open Forum Infect Dis, 2022; 9(8); ofac353 Erratum in: Open Forum Infect Dis. 2022;9(11):ofac589
10. Holdiness MR, Adverse cutaneous reactions to antituberculosis drugs: Int J Dermatol, 1985; 24(5); 280-85
Figures
Figure 1. Medication and platelet count evolution. * Darbepoetin alfa, amlodipine, calcium, folic acid, pantoprazole, sodium bicarbonate, sevelamer, polystyrene sulfonates, and iron sulfate; ** Isosorbide dinitrate, furosemide, and lercanidipine; *** Aspirin, clopidogrel, and unfractionated heparin. G/L=×109/L.Figure 2. Naranjo adverse drug reaction probability scale. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133