17 June 2025: Articles 
Twenty Years of Continuous Bisphosphonate Use Leading to Atypical Bilateral Femoral Fractures: A Case Report
Unusual clinical course, Challenging differential diagnosis, Diagnostic / therapeutic accidents, Adverse events of drug therapy, Clinical situation which can not be reproduced for ethical reasons
Anna Maria Monachino ABDEF 1*, Massimo BerdiniDOI: 10.12659/AJCR.946435
Am J Case Rep 2025; 26:e946435






Abstract
BACKGROUND: Osteoporosis is a skeletal disorder characterized by an impairment of bone strength that predisposes people to an increased risk of fracture. It is a major public health problem as one of the causes of fragility fractures in older people, placing a significant burden on healthcare systems. Bisphosphonates (BPs) have historically been the cornerstone of osteoporosis therapy and remain the most widely used drug today. Prolonged use of bisphosphonates has been demonstrated to be associated with atypical femoral fractures (AFFs).
CASE REPORT: Our case report presents a rare case in terms of duration of continuous treatment with osteoporosis drugs (approximately 20 years) in a woman who developed an atypical bilateral femoral fracture. She was treated surgically with bilateral long-nailing of the femurs in one-stage surgery. Surgical treatment resulted in osteosynthesis of the fracture and improvement of pain-related symptoms. One month after the treatment, she was able to walk with full weight bearing. At 6 months, her femoral fractures showed radiographic signs of healing.
CONCLUSIONS: This case highlights a rare complication of the widespread use of BPs, which remain the cornerstone of osteoporosis treatment and prevention of fragility fractures. It focuses on the necessity of a correct and prompt diagnosis for management of AFFs, including adherence to the proper dosing schedule of BPs.
Keywords: alendronate, Fracture Fixation, Intramedullary, Fractures, Spontaneous, Osteoporosis, Humans, Female, Femoral Fractures, Bone Density Conservation Agents, Diphosphonates, Aged
Introduction
The World Health Organization (WHO) defines osteoporosis as a “progressive systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptivity to fracture”. It is possible to quantify the mineralization loss of bone tissue through dual-energy X-ray absorptiometry (DEXA), which calculates bone mineral density (BMD). The clinical relevance of osteoporosis lies in the increased risk of fracture; consequently, according to recent UK NOGG guidelines, a T-score below −2.5 SD must be considered an important element in fracture risk assessment, together to other clinical factors such as body mass index, previous fractures, long-term corticosteroids treatment, and fall-related risk factors [1,2].
Osteoporosis is a major public health problem, as it is one of the leading causes of fragility fractures in older people, placing a significant burden on healthcare systems [3].
The International Osteoporosis Foundation (IOF) estimates that osteoporosis affects 6.3% of men and 21.2% of women over the age of 50, which means about 500 million individuals are affected worldwide [4]. In Italy, recent data from the Instituto Nazionale di Statistica (Istat) show that 8.1% of the total population have osteoporosis, with a prevalence of 13.5% among women and 2.3% in men, increasing at 47% for women and 10.3% for men among those over age 74 [5].
The first-line approach to osteoporosis management emphasizes the importance of fracture risk assessment, a healthy lifestyle with increased exercise and dietary changes, and pharmacotherapy [1,6].
Historically, bisphosphonates have been the cornerstone of osteoporosis therapy and they remain the most widely used osteoporosis drug today [1,7]. Despite their efficacy, it is widely accepted that prolonged use of bisphosphonates is associated with the development of atypical femoral fractures (AFFs), which were first described in 2005 by Odvina et al [8] and further characterized by the American Society for Bone and Mineral Research (ASBMR) diagnostic criteria for specific morphological features. The incidence of these fractures rise according to the length of bisphosphonates use, ranging from 1.8: 100 000 cases per year up to 113: 100 000 if treatment lasts less than 2 years or more than 8–9 years [9–10] (Table 1).
The effect of bisphosphonates in reducing bone turnover and the physiological flexibility of this tissue increases the susceptibility to accumulation of microlesions, even after minimal trauma, which can cause microfractures, leading to complete fractures, as in the case of an AFF [11].
This case report describes a case of bilateral AFFs associated with extensive bisphosphonate use, correlated with characteristic radiological findings and clinical history.
Case Report
In November 2022, a 73-year-old woman was admitted to our Emergency Department with a left subtrochanteric femoral fracture (32A3AO-OTAArbeitsgemeinschaft für Osteosynthesefragen – Orthopedic Trauma Classification) with no reported traumatic event. Her medical history included recurrent low back pain, osteoporosis, and a thyroidectomy performed in 2001. Osteoporosis was diagnosed in the late 1990s, leading to the patient being started on bisphosphonate therapy, specifically ibandronate 150 mg once a month, a treatment that was maintained continuously for approximately 20 years, until October 2022.
From May 2022, the patient reported a painless limp with a progressive decline in ambulatory function. After an unsuccessful rehabilitation program focused on strengthening the muscles of the lower extremities under the guidance of a physiotherapist, she was examined by a neurologist to explore a possible neurological origin of her problems and a possible relationship with her persistent back pain. This led to an electromyography being carried out, which showed no pathological findings.
From July 2022, she had worsening symptoms and increased limping, requiring a crutch for walking. She patient underwent pelvic and hip X-rays due to persistent symptoms, which showed no fractures (Figure 1). A magnetic resonance imaging (MRI) scan of the lower limb was performed in October 2022 to better characterize the pain described by the patient, to exclude that the pain was originating from the lumbar spine, and to examine the pelvic region and proximal femurs. MRI revealed bone edema associated with an incomplete fracture line in the left femoral cortical shaft (Figure 2). It also showed bone edema and a periosteal reaction – lateral cortical irregular thickness – in the contralateral (right) femoral shaft, which was clinically asymptomatic.
Approximately 1 week later, she patient had sudden onset of pain in left thigh, with loss of lower-extremity function and pain on active loading. Radiological examination in the Emergency Department revealed a transverse-subtrochanteric fracture of the left femur (32A3AO-OTAClassification) (Figure 3) and 2 cortical irregularities within the right femoral shaft (Figure 4).
Based on these data, as well as the clinical characteristics and features of the reported fracture, this was classified as an atypical fragility fracture of the femur according to the criteria established by ASBMR (Table 1).
Following diagnosis by the orthopedic consultant, a CT scan was requested to further define the cortical irregularities found in the right femur. The patient underwent surgery approximately 12 hours after diagnosis. During the waiting period, a skin traction was applied to the left lower extremity to keep the fractured limb in axis and to prevent potential soft-tissue complications due to the nature of the fracture.
Based on these findings and the patient’s medical history, the decision was made to proceed with bilateral femoral nailing. A single-stage surgical procedure was performed using an intramedullary approach with 2 long femoral locking nails (Gamma3® Locking Nailing System-Stryker) for osteosynthesis of the displaced fracture of the left femur and prophylactic osteosynthesis to prevent progression of cortical irregularities of the right femur. A diaphyseal cortical anomaly shown on a preoperative CT scan was confirmed on the postoperative X-ray as a true fracture. This was probably due to nailing of the femoral canal during surgery (Figure 5).
Full weight bearing was regained on the first postoperative day with the aid of crutches and physiotherapist assistance. The patient was discharged 5 days after surgery.
Clinical follow-up was performed at 15 days and at 1, 2, and 6 months after surgery, and radiographs were taken at 1, 2, and 6 months. She had a progressive decrease in pain and limping at 15 days. Follow-up radiographs showed adequate bone healing; tricortical bone healing was achieved at 6 months, along with improvement in walking ability and limb functionality from the first month (Figure 6).
Discussion
Osteoporosis is defined as a disease characterized by low bone density, deterioration of bone tissue, disrupted bone microarchitecture, compromised bone strength, and fracture [12].
Bisphosphonates (BPs) are often the first pharmacological intervention used due to their bone-antiresorptive capacity, which involves inhibition of osteoclast activity, thereby reducing the depletion of inorganic bone constituents such as calcium and phosphate. Importantly, our patient had been taking ibandronate, a third-generation BPs with nitrogen-enriched R2 side chains, for about 23 years. When absorbed by osteoclasts, this compound binds to and inhibits farnesyl-pyrophosphate-synthase, a key enzyme in the mevalonate pathway, and its inhibition results in reduced bone resorption [13]. The most common and well-known adverse effects of BPs are gastrointestinal disorders, musculoskeletal weakness, and osteonecrosis of the jaw. Recently, atypical femoral fractures (AFFs) have also been recognized. AFFs are considered rare and account for a small proportion (1–2%) of all femoral fractures [14].
The histo-morphometric analysis performed by Odvina et al in 2005 is often cited as the landmark study describing the specific pattern of femoral fractures associated with long-term use of bisphosphonates, particularly alendronate [9]. Their study of iliac crest bone biopsies revealed a significant imbalance in bone cell turnover, characterized by complete suppression of osteoblast activity and a markedly reduced presence of osteoclasts. These findings were confirmed by subsequent histo-morphometric studies [10,15].
Such changes in bone cell metabolism have biomechanical consequences: on the one hand, there is reduction in bone resorption, leading to hyper-mineralization; on the other hand, there is reduction in bone remodeling and the bone tissue capacity to repair the micro-damage that accumulates. Biomechanically, this results in an increase in the bone’s Young’s modulus, which reduces its tensile strength [15]. Even femoral geometry can affect the pathogenesis and location of AFFs. A larger femoral bowing angle changes stress/strain distribution on the femur, a high angle can determine a diaphyseal fracture, while a low angle is correlated with subtrochanteric fracture. Asians’ femurs commonly have these features, which can be a reason for the higher incidence of AFFs in this population [16]. Finally, AFFs can be explained as “insufficiency fractures” caused by cyclic loading from normal walking [17].
It can be difficult to identify atypical femoral fractures (AFFs). In 2010, the American Society for Bone and Mineral Research (ASBMR) defined radiological and clinical criteria for the diagnosis of AFFs, specifying 5 major and 7 minor criteria (Table 1). The diagnosis requires the contemporary presence of 4 major criteria, even in the absence of any minor criteria. Exclusion criteria include femoral neck, intertrochanteric, peri-prosthetic, and pathological fractures.
In 2013, the ASMBR itself revised and modified the criteria for diagnosis of atypical femoral fractures, slightly changing 3 of 5 major criteria and 1 minor criterion (Table 1). The use of these newer criteria showed a slight underestimation of the diagnosis of AFF in a community setting compared with the use of the 2010 criteria, which were less defined, as shown in a study by Leblanc et al [20]. An interesting finding of that study was the demographics of the patients diagnosed with an atypical hip fracture; in fact, as reported by the authors, these patients were younger, predominantly female, and had a higher rate of exposure to bisphosphonates than patients diagnosed with an atypical femoral fracture using the 2010 criteria. The higher rate of exposure to bisphosphonate therapy correlates strongly with our patient [9,11,18].
Our patient met all major criteria for diagnosis as defined by the ASBMR, as well as 4 minor criteria, including prodromal pain, lateral periosteal cortical reaction, and widespread diaphyseal cortical thickening (Figure 3). Prolonged use of bisphosphonates was a major risk factor in our patient’s history. Short people have a higher risk of developing AFFs, and our patient was 156 cm tall. Fortunately, she had no history of recent glucocorticosteroid therapy [19].
The lack of definitive guidelines for the prevention and management of AFFs underscores the importance of vigilant monitoring for thigh pain in patients with a history of prolonged bisphosphonate therapy. Prompt use of plain radiography (pelvic or segmental femoral radiography) is essential for early detection of impending fractures, which, if neglected, can progress to complete fractures. Impending fractures are generally asymptomatic; therefore, it is crucial to perform bilateral radiographic imaging of the limbs when a patient is symptomatic and at risk of AFFs. Magnetic resonance imaging (MRI) can provide important insight into the structure of the bone and is therefore considered more sensitive than computed tomography (CT) in identifying fracture lines and edema (sensitivity 87% vs 79%) (Figure 2) [20]. The US Food and Drug Administration approved a scan mode and software program to analyze the characteristics of AFFs on DEXA, which can allow AFF diagnosis before symptoms occur [21].
Once an atypical fracture has been diagnosed, discontinuation of bisphosphonate treatment is mandatory, as this significantly reduces the likelihood of a contralateral complete fracture, from 50% to 20%, as evidenced by data from the Kaiser Permanente Northwest (KPNW) database [22]. Conservative management, including partial weight bearing and cessation of bisphosphonate use, is generally recognized to have limited long-term efficacy. In the absence of specific guidelines, femoral cephalomedullary long-nailing is widely accepted as the initial management strategy. This technique has good load-bearing mechanical properties due to on-axis fixation and co-linear loading. Compared with plate fixation, it is associated with lower revision rates and shorter hospital stays, establishing cephalomedullary nailing as the criterion standard for surgical management of both existing and impending AFFs [23].
In the present case, bilateral nailing was performed for a complete fracture of the left femur and as a prophylactic measure for the right femur due to initial constant pain in the right thigh and radiographic evidence of impending fracture involving more than 50% of the lateral cortex. Recent studies suggest that prophylactic contralateral nailing is cost-effective [24].
Suppression of bone turnover resulting from prolonged use of bisphosphonates (BPs) can lead to delayed union or non-union. Prasarn et al reported that one-third of AFFs have delayed union or non-union, with significantly longer ossification times in patients who had been taking BPs compared to controls: 6.5 versus 4.8 months [25].
These observations raise legitimate concerns about prescribing bisphosphonate and its potential consequences, but epidemiological evidence classifies AFFs as rare, with an absolute risk of only 3.2 to 50 cases per 100 000 patients per year [26]. Therefore, despite an established association between AFFs and bisphosphonate therapy, the risk-benefit analysis remains in favor of administering the antiresorptive agents to patients at high risk of fragility fractures [27]. To minimize the risk of developing AFFs, there is a consensus in clinical practice that long-term continuous bisphosphonate use should be interrupted by a “drug holiday” [28]. It is advisable to reassess the risk of fragility fractures and bone mineral density (BMD) after 5 years of bisphosphonate (BP) therapy in patients at high risk, and after 10 years in patients at very high risk. In the absence of additional clinical risk factors and if the T-score is >−2.5, BP therapy may be discontinued for 1.5 to 3 years, after which re-evaluation is recommended [1]. In our patient, following surgery, discontinuation of bisphosphonate therapy and a subsequent DEXA scan to assess current BMD were warranted. To prevent refracture, it is essential to estimate the 10-year probability of a major osteoporotic fracture (MOF) using tools like FRAX assessment thresholds [29]. The European Calcified Tissue Society suggests the use of teriparatide in patients who have undergone surgery for AFFs, as this anabolic agent appears to promote bone healing [30].
The present case appears to be rare in terms of duration of continuous treatment with osteoporosis drugs (approximately 20 years) in a patient who developed an atypical bilateral femur fracture.
As a case report, this study has obvious limitations. The data collection was based on patient-reported data on the management of home therapy for osteoporosis, and it is not known why the duration of therapy was so long, probably due to loss to follow-up by the general practitioner.
Informed consent was obtained for the collection and publication of anonymous clinical case data in accordance with the ethical standards of the Declaration of Helsinki of 1964 and its subsequent amendments or comparable ethical standards [31].
Conclusions
Atypical femoral fractures(AFFs) are a rare but recognized complication of the prolonged use of bisphosphonates (BPs), which, despite this complication, remain the cornerstone of osteoporosis management and fragility fracture prevention. Proper management of patients with osteoporosis treated with BPs by the prescribing consultant is of utmost importance. Complications associated with the use of these drugs can be reduced by correct administration schedules, dosage and duration of treatment with these drugs, and by observing “drug holidays”. This case report shows the importance of early suspicion and diagnosis of potential AFFs in patients on long-term BPs therapy who present with symptoms of thigh pain and worsening gait. Patient treatment adherence and regular follow-up must be at the center of specific screening strategies. Guidelines focus on the importance of re-assessing fracture risk at least after 5 years of BPs therapy or, previously, whether clinical risk factors change. A repeat DEXA may be useful, as BPs during follow-up can aid to checking AFFs features in advance, leading clinicians to prescribe further examinations and considering interrupting or changing administration of BPs.
There are increasing numbers of guidelines focusing on the prevention and management of AFFs, highlighting the need for a multidisciplinary strategy to develop more precise risk assessment methodologies and formulate individualized treatment protocols.
Figures
 Figure 1. Left-hip X-rays taken 2 months before diagnosis of the atypical fracture of the left femur. The image shows no macroscopic alterations.
Figure 1. Left-hip X-rays taken 2 months before diagnosis of the atypical fracture of the left femur. The image shows no macroscopic alterations. 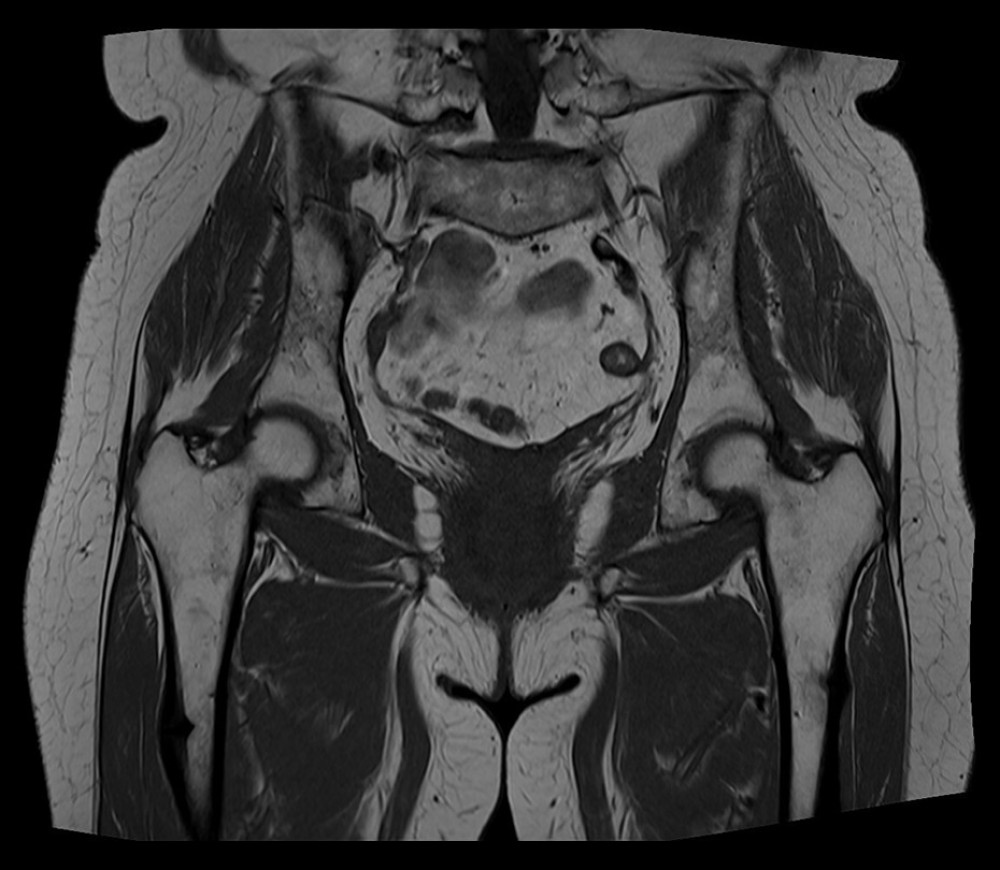 Figure 2. Magnetic resonance imaging (MRI) scan of the pelvis, hips, and proximal femurs 1 month before appearance of the proximal left femoral fracture.
Figure 2. Magnetic resonance imaging (MRI) scan of the pelvis, hips, and proximal femurs 1 month before appearance of the proximal left femoral fracture.  Figure 3. X-ray of pelvis at admission.
Figure 3. X-ray of pelvis at admission.  Figure 4. X-ray of right femur at admission.
Figure 4. X-ray of right femur at admission. 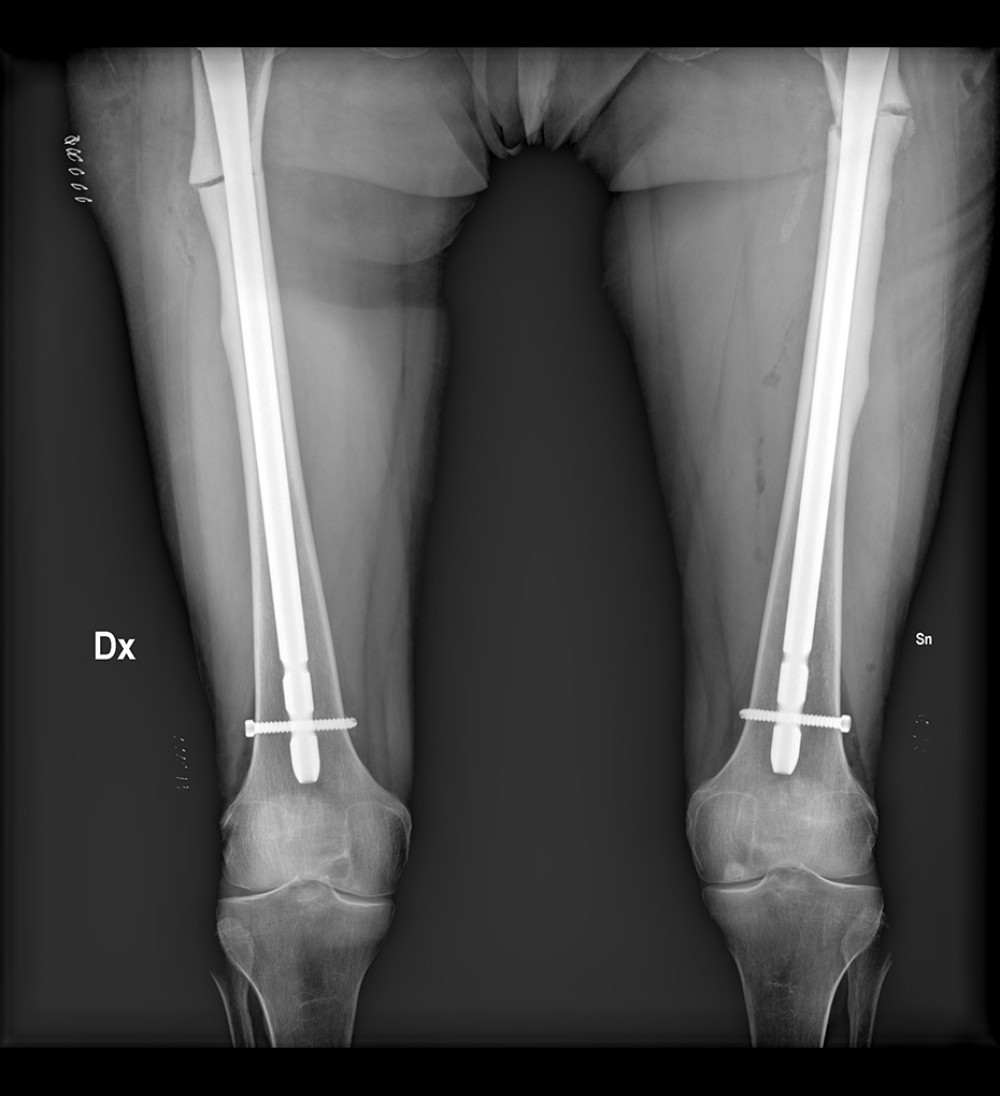 Figure 5. X-ray of osteosynthesis of the displaced fracture of the left femur and prophylactic osteosynthesis of the right femur.
Figure 5. X-ray of osteosynthesis of the displaced fracture of the left femur and prophylactic osteosynthesis of the right femur. 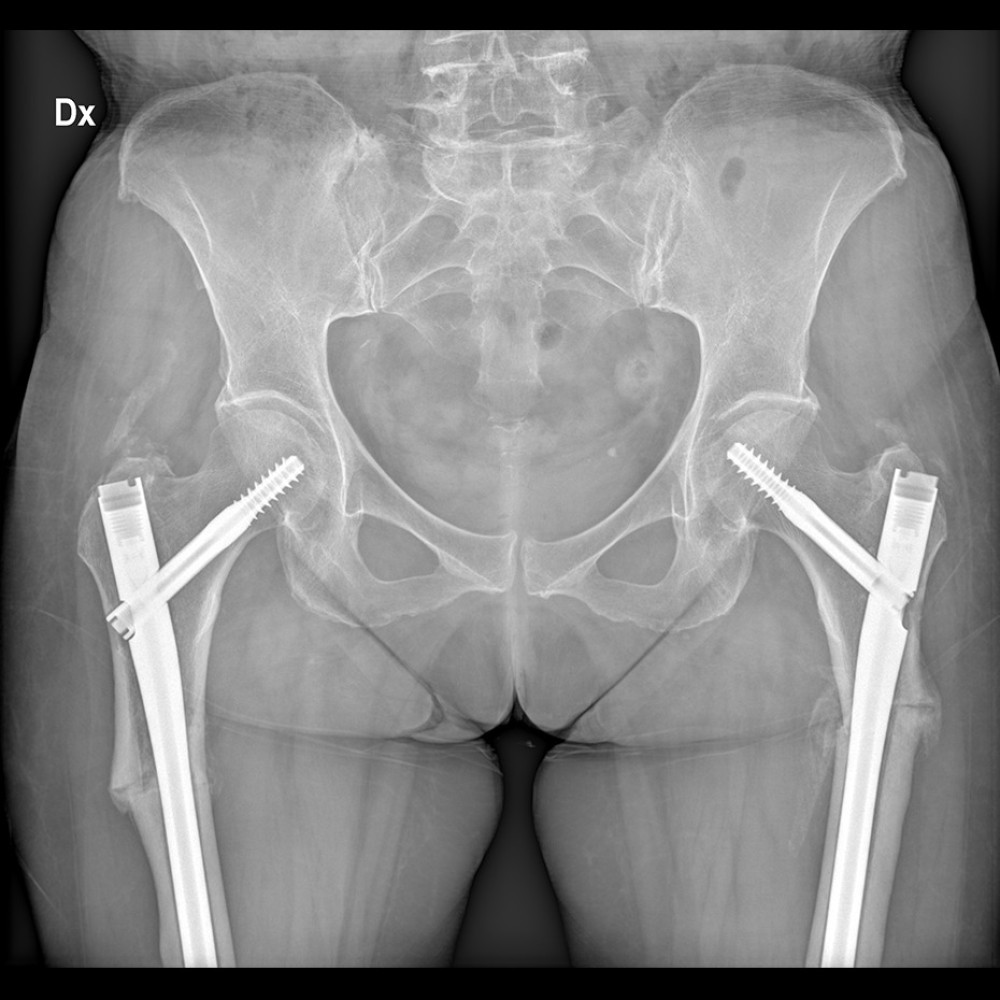 Figure 6. X-ray of the pelvis and bilateral proximal femur at 1-month follow-up.
Figure 6. X-ray of the pelvis and bilateral proximal femur at 1-month follow-up. 
References
1. Gregson CL, Armstrong DJ, Bowden J, UK clinical guideline for the prevention and treatment of osteoporosis: Arch Osteoporos, 2022; 17(1); 58 [Erratum in: Arch Osteoporos. 2022;17(1):80]
2. NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy: JAMA, 2001; 285(6); 785-95
3. Kanis JAon behalf of the World Health Organization Scientific Group, Assessment of Osteoporosis at the Primary Health Care Level: Technical Report, 2007, UK, WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield
4. Hernlund E, Svedbom A, Ivergård M, Osteoporosis in the European Union: Medical management, epidemiology and economic burden: A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA): Arch Osteoporos, 2013; 8(1); 136
5. Farchi GOsteoporosis the size of the problem in Italy, 2001 [in Italian]https://www.epicentro.iss.it/focus/osteoporosi/FARCHI%20osteoporosi.pdf
6. National Institute for Health and Care Excellence (NICE), 2019 https://www.nice.org.uk/
7. Maraka S, Kennel KA, Bisphosphonates for the prevention and treatment of osteoporosis: BMJ, 2015; 351; 3783
8. Odvina CV, Zerwekh JE, Rao DS, Severely suppressed bone turnover: A potential complication of alendronate therapy: J Clin Endocrinol Metab, 2005; 90; 1294-301
9. Shane E, Atypical subtrochanteric and diaphyseal femoral fractures: Second report of a Task Force of the American Society for Bone and Mineral Research: J Bone Miner Res, 2014; 29; 1-23
10. Ma S, Long-term effects of bisphosphonate therapy: Perforations, microcracks and mechanical properties: Sci Rep, 2017; 7; 43399
11. LeBoff MS, Greenspan SL, Insogna KL, The clinician’s guide to prevention and treatment of osteoporosis: Osteoporos Int, 2022; 33(10); 2049-102 [Erratum in: Osteoporos Int. 2022;33(10):2243]
12. Shane E, Atypical subtrochanteric and diaphyseal femoral fractures: Report of a task force of the American Society for Bone and Mineral Research: J Bone Miner Res, 2010; 25; 2267-94
13. Gárgyán I, Dózsai D, Csonka I, Bisphosphonate therapy associated with bilateral atypical femoral fractureand delayed union: Jt Dis Relat Surg, 2022; 33; 24-32
14. Somford MP, Draijer FW, Thomassen BJ, Bilateral fractures of the femur diaphysis in a patient with rheumatoid arthritis on long-term treatment with alendronate: Clues to the mechanism of increased bone fragility: J Bone Miner Res, 2009; 24; 1736-74
15. Ural A, Biomechanical mechanisms of atypical femoral fracture: J Mech Behav Biomed Mater, 2021; 124; 104803
16. Ettinger B, Burr DB, Ritchie RO, Proposed pathogenesis for atypical femoral fractures: lessons from materials research: Bone, 2013; 55(2); 495-500
17. Allen M, Rand Burr DB, Bisphosphonate effects on bone turnover, microdamage and mechanical properties: What we think we know and what we know that we don’t know: Bone, 2011; 49; 56-65
18. Meier RP, Perneger TV, Stern R, Increasing occurrence of atypical femoral fractures associated with bisphosphonate use: Arch Intern Med, 2012; 12; 930-36
19. Jiang SY, Kaufman DJ, Chien BY, Prophylactic fixation can be cost-effective in preventing a contralateral bisphosphonate-associated femur fracture: Clin OrthopRelat Res, 2019; 477; 480-90
20. LeBlanc ES, Evaluating atypical features of femur fractures: How change in radiological criteria influenced incidence and demography of atypical femur fractures in a community setting: J Bone Miner Res, 2017; 32; 2304-14
21. Khan AA, Leslie WD, Lentle B, Atypical femoral fractures. A teaching perspective: Can Assoc Radiol J, 2015; 66(2); 102-7
22. Rudran B, Current concepts in the management of bisphosphonate associated atypical femoral fractures: World J Orthop, 2021; 12; 660-71
23. Haj Mirzaian A, Use of advanced imaging for radiographically occult hip fracture in elderly patients: A systematic review and meta-analysis: Radiology, 2020; 296; 521-31
24. Feldstein AC, Incidence and demography of femur fractures with and without atypical features: J BoneMiner Res, 2012; 27; 977-86
25. Prasarn ML, Ahn J, Helfet DL, Bisphosphonate-associated femur fractures have high complication rates with operative fixation: Clin Orthop Relat Res, 2012; 470; 2295-301
26. Adams AL, Bisphosphonate drug holiday and fracture risk: A population-based cohort study: J Bone Miner Res, 2018; 33; 1252-59
27. Kanis JA, Johnell O, Oden A, FRAX and the assessment of fracture probability in men and women from the UK: Osteoporos Int, 2008; 19; 385-97
28. Reid I, Rand Billington EO, Drug therapy for osteoporosis in older adults: Lancet, 2022; 99; 1080-92
29. van de Laarschot DM, McKenna MJ, Abrahamsen B, Medical management of patients after atypical femur fractures: A systematic review and recommendations from the European Calcified Tissue Society: J Clin Endocrinol Metab, 2020; 105(5); 1682-99
30. Brown JP, Bisphosphonates for treatment of osteoporosis: Expected benefits, potential harms, and drug holidays: Can Fam Physician, 2014; 60; 324-33
31. World Medical Association: Declaration of Helsinki-Ethical Principles for Medical Research Involving Human Subjects https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human
Figures
Figure 1. Left-hip X-rays taken 2 months before diagnosis of the atypical fracture of the left femur. The image shows no macroscopic alterations.Figure 2. Magnetic resonance imaging (MRI) scan of the pelvis, hips, and proximal femurs 1 month before appearance of the proximal left femoral fracture.Figure 3. X-ray of pelvis at admission.Figure 4. X-ray of right femur at admission.Figure 5. X-ray of osteosynthesis of the displaced fracture of the left femur and prophylactic osteosynthesis of the right femur.Figure 6. X-ray of the pelvis and bilateral proximal femur at 1-month follow-up. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952989
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953049
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952567
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953259
Most Viewed Current Articles
07 Dec 2021 : Case report  22,744,454
22,744,454
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report
175,030
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,056
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,026
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133