30 June 2025: Articles 
A 64-Year-Old Woman with Diabetes Mellitus Associated with Increased Urinary Oxalate Excretion Presenting with Acute Kidney Injury Due to Acute Oxalate Nephropathy
Unusual clinical course, Challenging differential diagnosis, Educational Purpose (only if useful for a systematic review or synthesis)
Krutika Mahendra GohilDOI: 10.12659/AJCR.946526
Am J Case Rep 2025; 26:e946526






Abstract
BACKGROUND: Acute oxalate nephropathy (AON) is a rare complication of diabetes mellitus (DM), resulting in kidney damage. This report describes the case of a 64-year-old woman with DM associated with increased urinary oxalate excretion presenting with acute kidney injury (AKI) due to AON.
CASE REPORT: A 64-year-old woman with recently diagnosed diabetes mellitus and hypertension presented to the hospital with right-sided flank pain. Initial renal function tests (RFTs) indicated a blood urea nitrogen (BUN) level of 68.6 mg/dL and a serum creatinine of 9.0 mg/dL, up from a serum creatinine of 1.5 mg/dL recorded a month earlier. Due to further deterioration of her metabolic panel and worsening anuria, hemodialysis was commenced. A biopsy was performed to establish the cause, which revealed diabetic nephrosclerosis and calcium oxalate crystals in the tubules. A detailed review of the patient’s medical history was conducted, yet no definitive factor emerged. We inferred that diabetes triggered acute oxalate nephropathy due to increased oxalate excretion, which subsequently progressed to end-stage renal disease. The patient’s renal function did not recover, leading to maintenance hemodialysis use for end-stage renal failure.
CONCLUSIONS: This observation underscores the necessity for assessing oxalate nephropathy in unexplained renal failure, as prompt detection and treatment could improve outcomes. This report highlights a rare but important complication of DM, and that patients who present with AKI should be investigated for the presence of AON.
Keywords: Diabetes Mellitus, Type 2, Gastrointestinal Transit, Oxalates, Renal Dialysis, Humans, Female, Middle Aged, Acute Kidney Injury, Diabetic Nephropathies, Calcium Oxalate
Introduction
Acute oxalate nephropathy (AON) is an uncommon condition distinguished by the excessive accumulation of calcium oxalate crystals in the renal tubules, resulting in compromised renal function. Disturbances at any stage of the oxalate pathway, including increased production, increased absorption, decreased degradation, and diminished renal excretion, contribute to a disruption in oxalate homeostasis. Oxalate crystals supersaturate, precipitate, aggregate, and deposit within tubule interstitium [1]. Hyperoxaluria can progress to the development of nephrocalcinosis, nephrolithiasis, or oxalate nephropathy [2]. This can clinically manifest as acute kidney injury (AKI), chronic kidney disease (CKD), or end-stage renal disease (ESRD) [3]. A large majority of the cases reported have been due to increased intake of oxalate-containing foods. AON as a consequence of diabetes mellitus (DM) is rare. This report describes the case of a 64-year-old woman with DM associated with increased urinary oxalate excretion presenting with AKI due to AON.
Case Report
A 64-year-old woman with a medical history of recently diagnosed diabetes mellitus, hypertension on amlodipine and losartan-hydrochlorothiazide, presented to the hospital with a 4-day history of right-sided flank pain, anuria, nausea, and vomiting. She additionally experienced an episode of emesis followed by transient right-sided chest pain. She reported having no urine output in the past 2 days and noted accompanying shortness of breath. She weighed 94 kg and was 160 cm tall. Her body temperature was 37.3°C (99.1°F), blood pressure was 170/71 mmHg, and all other vital signs were within normal limits. Systemic examination was unremarkable except for right-sided flank tenderness and bilateral non-pitting pedal edema. There was no past medical history of celiac disease, Crohn disease, chronic pancreatitis, or
Dietary causes of hyperoxaluria were ruled out by inquiring about the consumption of several oxalate-rich dietary sources, including rhubarb, spinach, starfish fruit, black tea, chocolate, peanuts, and chaga mushrooms, all of which have been associated with elevated oxalate levels. Additionally, we considered asking about orlistat consumption, as it can interfere with fat absorption and increase the oxalate absorption from the gastrointestinal tract. Diabetes can lead to increased oxalate excretion. Given her history of DM and absence of other gastrointestinal causes, we thought that increased gastrointestinal transit time, as a result of diabetic gastroparesis, could have further precipitated AON by increasing oxalate absorption. Hence, we conducted a gastric emptying scintigraphy (Figure 3), which confirmed delayed emptying (Table 1). Her renal function did not improve thereafter, and she was placed on maintenance hemodialysis for end-stage renal failure.
Discussion
We have described the case of a 64-year-old woman with diabetes mellitus associated with increased urinary oxalate excretion presenting with acute kidney injury due to acute oxalate nephropathy. The clinical spectrum of oxalate nephropathy ranges from AKI, AKI on CKD, to CKD requiring hemodialysis [4]. Enzymatic defects in the glyoxylate cycle can lead to primary hyperoxaluria, which is characterized by an hyperoxaluric state [5]. Secondary causes of hyperoxaluria encompass increased intake of dietary oxalate or precursors and conditions that result in increased intestinal oxalate absorption. These include: Crohn’s disease, celiac disease, diabetic gastroenteropathy, small bowel resection, orlistat use, Roux-en-Y gastric bypass, and cystic fibrosis [6]. For every 100 mg of dietary oxalate ingested, there is a 1.7 mg rise in 24-hour urinary oxalate [7]. Green leafy vegetables like rhubarb and spinach are oxalate-rich dietary sources. In people eating a normal serving of spinach daily, their intake could surpass 1000 mg per day [8]. Vitamin C is a precursor to oxalate and can potentially convert into it. Consuming more than 1000 mg daily is considered as a risk factor [9]. Hyperoxaluria has also been linked to decreased intestine bacterial oxalate breakdown brought on by antibiotic use [10]. Acute dehydration, renin-angiotensin system inhibitor use, nonsteroidal anti-inflammatory medicines (NSAIDs), and diuretics can act as triggers for an underlying hyperoxaluria, which can progress to renal failure [11]. All of these contributing factors were excluded in our patient.
Our patient with underlying diabetes presented with acute oxalate nephropathy, ultimately precipitating end-stage renal disease. Diabetes has been linked to higher oxalate excretion, probably due to elevated levels of oxalate precursors like glyoxylate and glyoxal, as observed in diabetic individuals [9,12]. Additionally, diabetes can cause gastroparesis [13], increasing the risk of volume depletion and calcium oxalate supersaturation [14]. The Chronic Renal Insufficiency Cohort (CRIC) study reported that diabetic individuals had 11% higher 24-hour urinary oxalate than non-diabetic individuals [15]. Janga et al documented a case of oxalate nephropathy in a patient with long-standing diabetes, where renal hypoperfusion from diabetes ketoacidosis triggered renal failure [16]. Polarizable calcium crystals in tubular lumen, tubular epithelial cells, and infrequently in the interstitium, are the main pathological findings in cases of oxalate nephropathy. In addition to underlying glomerulosclerosis, different degrees of acute tubular injury with necrosis, interstitial nephritis, and fibrosis are observed [6].
Secondary hyperoxaluria is usually managed with: (a) low-oxalate and high-calcium diet, and (b) increasing fluid intake (>3 L/1.73 m2), (c) supplemented with bile acid sequestrants and calcium or other oxalate binders to reduce oxalate permeability in the intestines, and (d) consuming probiotics that include oxalate-degrading bacteria [17]. Although uncommon, secondary oxalate nephropathy can be fatal. Over half of such patients need renal replacement therapy, and most still depend on dialysis [4].
Conclusions
This report highlights a rare but important complication of DM and that patients who present with AKI should be investigated for the presence of AON. In individuals with inexplicable renal failure, it is critical to rule out oxalate nephropathy since early detection and treatment may improve prognosis. AON presents a significant risk, leading to both acute and chronic renal failure. It is crucial to evaluate predisposing factors in patients experiencing sudden and persistent renal failure, and a renal biopsy should be promptly done in such cases. In cases where AON is secondary to another systemic disease, addressing the primary disorder is paramount to prevent irreversible renal damage. The outcome of AON depends on the underlying cause, the oxalate burden, and the expediency of the intervention.
Figures
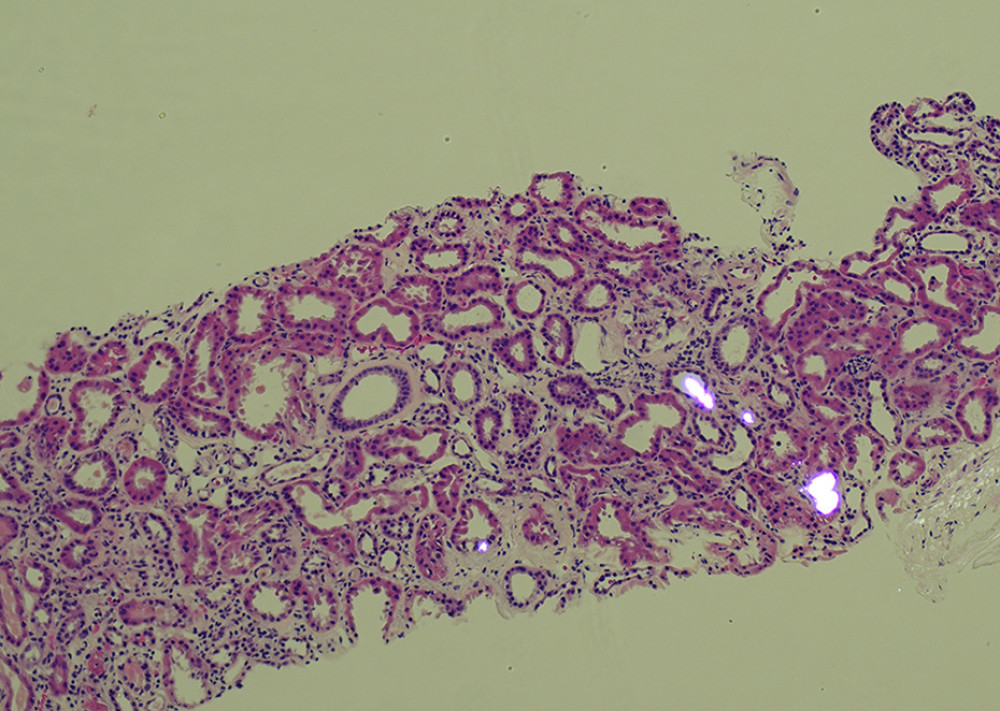 Figure 1. Calcium oxalate crystals accumulated in kidney tubules under polarizing lightA photomicrograph of the kidney biopsy from a 64-year-old woman with diabetes mellitus (DM) associated with acute kidney injury (AKI) due to acute oxalate nephropathy (AON). The light microscopy combines polarized light microscopy to show that some dilated renal tubules contain polygonal calcium oxalate crystals. Hematoxylin and eosin (H&E). Magnification ×20.
Figure 1. Calcium oxalate crystals accumulated in kidney tubules under polarizing lightA photomicrograph of the kidney biopsy from a 64-year-old woman with diabetes mellitus (DM) associated with acute kidney injury (AKI) due to acute oxalate nephropathy (AON). The light microscopy combines polarized light microscopy to show that some dilated renal tubules contain polygonal calcium oxalate crystals. Hematoxylin and eosin (H&E). Magnification ×20. 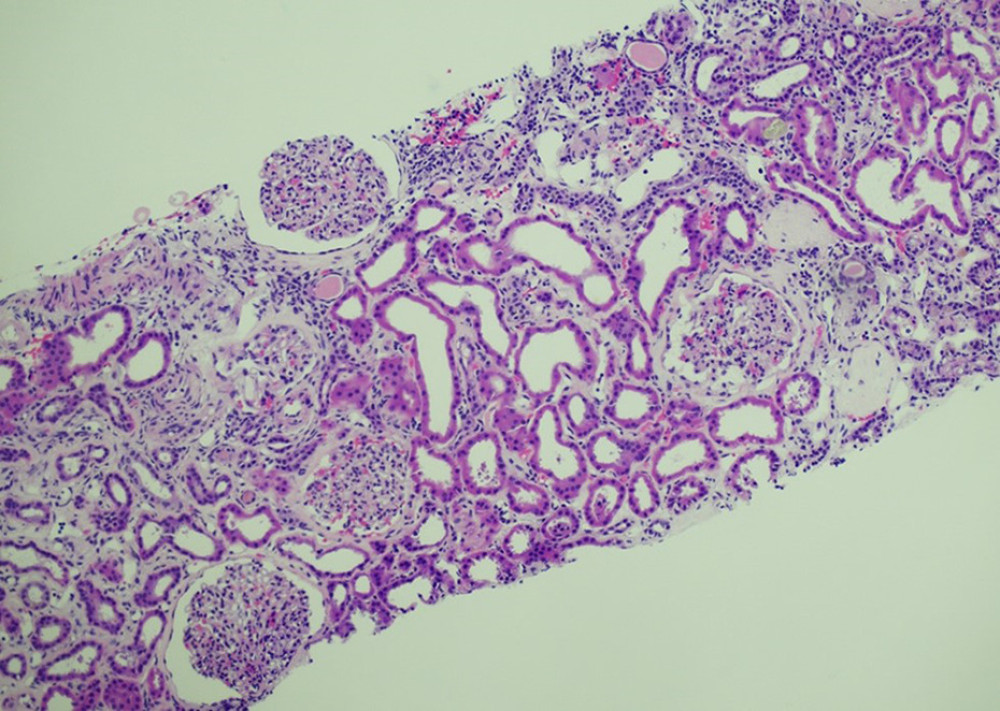 Figure 2. Diabetic nephrosclerosis and oxalate nephropathy leading to acute tubular injuryThe section shows characteristic changes of diabetic nephrosclerosis, including thickened glomerular basement membranes and nodular glomerulosclerosis. Additionally, calcium oxalate crystals are observed within the lumen of kidney tubules.
Figure 2. Diabetic nephrosclerosis and oxalate nephropathy leading to acute tubular injuryThe section shows characteristic changes of diabetic nephrosclerosis, including thickened glomerular basement membranes and nodular glomerulosclerosis. Additionally, calcium oxalate crystals are observed within the lumen of kidney tubules. 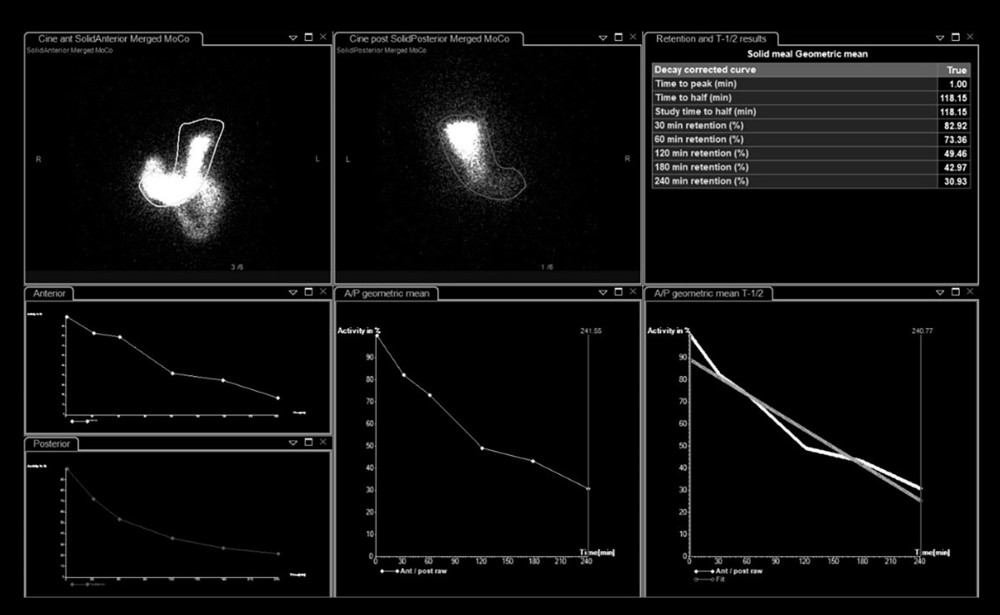 Figure 3. Gastric emptying scintigraphy, which is the criterion standard test for diagnosing gastric gastroenteropathyThe patient was diagnosed with gastroparesis, likely due to diabetes, after observing the 31% retention after 4 hours (normal value: less than 10% at 240 minutes), confirming delayed gastric emptying of a solid meal on the gastric emptying scintigraphy.
Figure 3. Gastric emptying scintigraphy, which is the criterion standard test for diagnosing gastric gastroenteropathyThe patient was diagnosed with gastroparesis, likely due to diabetes, after observing the 31% retention after 4 hours (normal value: less than 10% at 240 minutes), confirming delayed gastric emptying of a solid meal on the gastric emptying scintigraphy. 
References
1. Geraghty R, Wood K, Sayer JA, Calcium oxalate crystal deposition in the kidney: Identification, causes and consequences: Urolithiasis, 2020; 48(5); 377-84
2. Karaolanis G, Lionaki S, Moris D, Secondary hyperoxaluria: A risk factor for kidney stone formation and renal failure in native kidneys and renal grafts: Transplant Rev (Orlando), 2014; 28(4); 182-87
3. Buysschaert B, Aydin S, Morelle J, Etiologies, clinical features, and outcome of oxalate nephropathy: Kidney Int Rep, 2020; 5(9); 1503-9
4. Lumlertgul N, Siribamrungwong M, Jaber BL, Susantitaphong P, Secondary oxalate nephropathy: A systematic review: Kidney Int Rep, 2018; 3(6); 1363-72
5. Cochat P, Rumsby G, Primary hyperoxaluria: N Engl J Med, 2013; 369(7); 649-58
6. Demoulin N, Aydin S, Gillion V, Pathophysiology and management of hyperoxaluria and oxalate nephropathy: A review: Am J Kidney Dis, 2022; 79(5); 717-27
7. Mitchell T, Kumar P, Reddy T, Dietary oxalate and kidney stone formation: Am J Physiol Renal Physiol, 2019; 316(3); F409-F13
8. Holmes RP, Kennedy M, Estimation of the oxalate content of foods and daily oxalate intake: Kidney Int, 2000; 57(4); 1662-67
9. Bao D, Wang Y, Zhao MH, Oxalate Nephropathy and the mechanism of oxalate-induced kidney injury: Kidney Dis (Basel), 2023; 9(6); 459-68
10. Joshi S, Goldfarb DS, The use of antibiotics and risk of kidney stones: Curr Opin Nephrol Hypertens, 2019; 28(4); 311-15
11. Mulay SR, Anders HJ, Crystallopathies: N Engl J Med, 2016; 374(25); 2465-76
12. Efe O, Verma A, Waikar SS, Urinary oxalate as a potential mediator of kidney disease in diabetes mellitus and obesity: Curr Opin Nephrol Hypertens, 2019; 28(4); 316-20
13. Krishnan B, Babu S, Walker J, Gastrointestinal complications of diabetes mellitus: World J Diabetes, 2013; 4(3); 51-63
14. Crook ED, Cook WJ, Bergman SM, Rapid renal deterioration secondary to oxalate in a patient with diabetic gastroenteropathy: Am J Kidney Dis, 1995; 26(1); 68-71
15. Waikar SS, Srivastava A, Palsson R, Association of urinary oxalate excretion with the risk of chronic kidney disease progression: JAMA Intern Med, 2019; 179(4); 542-51
16. Janga K, Jana K, Greenberg S, Acute kidney injury from acute oxalate nephropathy in diabetic ketoacidosis: A case report: Ann Intern Med Clin Cases, 2024; 3(1); e231068
17. Ermer T, Eckardt KU, Aronson PS, Knauf F, Oxalate, inflammasome, and progression of kidney disease: Curr Opin Nephrol Hypertens, 2016; 25(4); 363-71
Figures
Figure 1. Calcium oxalate crystals accumulated in kidney tubules under polarizing lightA photomicrograph of the kidney biopsy from a 64-year-old woman with diabetes mellitus (DM) associated with acute kidney injury (AKI) due to acute oxalate nephropathy (AON). The light microscopy combines polarized light microscopy to show that some dilated renal tubules contain polygonal calcium oxalate crystals. Hematoxylin and eosin (H&E). Magnification ×20.Figure 2. Diabetic nephrosclerosis and oxalate nephropathy leading to acute tubular injuryThe section shows characteristic changes of diabetic nephrosclerosis, including thickened glomerular basement membranes and nodular glomerulosclerosis. Additionally, calcium oxalate crystals are observed within the lumen of kidney tubules.Figure 3. Gastric emptying scintigraphy, which is the criterion standard test for diagnosing gastric gastroenteropathyThe patient was diagnosed with gastroparesis, likely due to diabetes, after observing the 31% retention after 4 hours (normal value: less than 10% at 240 minutes), confirming delayed gastric emptying of a solid meal on the gastric emptying scintigraphy. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133