14 June 2025: Articles 
Low Antigen Titre Disseminated Cryptococcosis in Immunocompromised Hosts: Two Challenging Case Reports
Unusual clinical course, Challenging differential diagnosis
Srishty AgarwalDOI: 10.12659/AJCR.946589
Am J Case Rep 2025; 26:e946589






Abstract
BACKGROUND: Cryptococcus is a yeast-like fungus commonly found in soil and typically causes disease in immunocompromised individuals due to impaired cell-mediated immunity. While the central nervous system (CNS) and lungs are most frequently affected, disseminated disease can involve multiple organs, including the skin, liver, spleen, kidneys, and bone marrow. Symptoms such as headache, fever, and altered mental status often require extensive diagnostic evaluation.
CASE REPORT: We present 2 unusual cases of cryptococcal growth in the blood without meningoencephalitis, with low cryptococcal antigen titres (1: 80 in both cases). The first case involves a post-kidney transplant patient with respiratory symptoms who underwent bronchoalveolar lavage (BAL), revealing Cryptococcus growth. A subsequent positive blood culture confirmed disseminated cryptococcosis, and the patient was treated with antifungal therapy. The second case is of a patient with HIV, non-adherent to treatment, who developed a complicated infection course. The cryptococcal antigen was positive in the serum, prompting treatment with a high-dose antifungal regimen. Despite negative results in BAL and cerebrospinal fluid, the blood culture was positive for Cryptococcus, necessitating intensive antifungal therapy according to protocolized guidelines.
CONCLUSIONS: These cases highlight the unusual presentation of disseminated cryptococcal infection with low serum antigen titres (1: 80) and positive blood culture, indicating disseminated infection even without CNS involvement. This emphasizes the importance of considering disseminated cryptococcosis in the differential diagnosis of immunocompromised patients, even with low antigen titres in serum. It suggests that clinicians should order blood cultures to alter management strategies, particularly in patients with atypical presentations.
Keywords: Cryptococcosis, Fungemia, HIV, Transplants, Humans, Antifungal Agents, Antigens, Fungal, Cryptococcus, Immunocompromised Host, Kidney Transplantation
Introduction
Cryptococcosis is a systemic fungal infection caused by the invasive fungus
This infection most commonly occurs in individuals with conditions such as HIV, diabetes, chronic renal disease, chronic liver disease, prolonged steroid use, and organ transplantation. In the United States, cryptococcal antigenemia is observed in 2.9% of HIV-infected patients with CD4 counts <100 cells/μL and in 4.3% of those with CD4 counts <50 cells/μL [1]. Additionally, 20% to 60% of cryptococcosis cases in HIV-negative patients occur in organ transplant recipients [3]. These statistics highlight the high prevalence of cryptococcal infections among immunocompromised populations, yet bloodstream infections without CNS involvement remain an atypical presentation. Such cases challenge traditional diagnostic and management strategies, as clinicians often prioritize CNS symptoms when suspecting cryptococcal infections.
This report presents 2 cases of cryptococcal bloodstream infection without CNS involvement, underscoring the diagnostic challenges and clinical implications of these atypical presentations. These cases highlight the importance of vigilance in recognizing disseminated cryptococcal infections and suggest the need for adjustments in antifungal therapy to effectively manage these unusual presentations.
Case Reports
CASE 1:
A 43-year-old man with a history of end-stage renal disease secondary to type 2 diabetes mellitus underwent an unrelated kidney transplant in 2022 and was maintained on tacrolimus monotherapy for immunosuppression. Two years after transplant, he presented with acute kidney injury and generalized fatigue. Because kidney rejection was suspected, he was empirically treated with intravenous (i.v.) methylprednisolone; however, biopsy findings ruled out rejection, prompting an infectious workup. Urine cultures were negative for cytomegalovirus (CMV) and BK polyomavirus virus, and a respiratory panel was also unremarkable. A chest computed tomography scan revealed multifocal bronchopneumonia with scattered lung nodules, leading to a bronchoalveolar lavage (BAL), which returned positive for
Ten days after discharge, the patient returned with minimal symptoms of generalized fatigue; however, blood cultures grew
At the 1-month follow-up, the patient showed clinical improvement and was advised to continue fluconazole therapy for 1 year to prevent recurrence.
CASE 2:
A 44-year-old man with a known diagnosis of HIV and a history of non-adherence to antiretroviral therapy presented with worsening shortness of breath, high fever, and chills for 2 weeks. One week prior to admission, he had visited the Emergency Department with similar concerns and was discharged on levofloxacin. On current admission, the patient had hypoxia, prompting hospitalization.
On evaluation, laboratory investigations revealed a CD4 count of 9 cells/μL (reference range: 500–1500 cells/μL) and an HIV viral load in the millions. Chest X-ray showed diffuse alveolar and interstitial infiltrates, suggestive of
During his hospitalization, serum cryptococcal antigen returned positive, with a titer of 1: 80, prompting lumbar puncture to assess for CNS involvement. CSF analysis initially showed no growth, but a prozone effect was later ruled out through sample dilution. Blood cultures subsequently grew
The patient’s respiratory status deteriorated, necessitating intubation. A chest computed tomography scan demonstrated rapidly progressive multifocal pneumonitis and scattered lung nodules, complicated by pneumomediastinum. These findings, along with worsening hypoxia, raised concerns for superimposed cryptococcal pneumonia and possible immune reconstitution inflammatory syndrome. The patient was treated aggressively with amphotericin B, initially dosed at 5 mg/kg and increased to 10 mg/kg. However, amphotericin B was discontinued due to worsening renal function, and high-dose fluconazole (1200 mg daily) was continued. Concurrently, valganciclovir 450 mg daily was initiated for CMV viremia.
The hospital course was complicated by acute respiratory distress syndrome, requiring extracorporeal membrane oxygenation support. After a month of intensive multidisciplinary management, including treatment for PJP, cryptococcosis, and CMV, the patient’s condition stabilized. He was discharged on prednisone (tapered), trimethoprim-sulfamethoxazole (Bactrim DS) 1 tablet daily for PJP prophylaxis, fluconazole 400 mg daily for cryptococcal maintenance, valganciclovir 450 mg daily for CMV management, and Symtuza for HIV therapy.
At the 1-month follow-up, the patient showed significant clinical improvement, with stable respiratory status and improved overall condition. He was extensively counselled on strict medication adherence to prevent opportunistic infections and ensure effective HIV management.
Discussion
Here, we present 2 cases of disseminated cryptococcosis: one in a kidney transplant recipient on immunosuppressive therapy and the other in an HIV-positive patient who was non-adherent to treatment – both were at high risk for this infection. Despite being at high risk for opportunistic fungal infections, it is interesting to note that although both patients had a positive serum titer for cryptococcal antigen (1: 80), lumbar punctures excluded CNS involvement in both cases. Initially, both patients started treatment with fluconazole based on findings from BAL, clinical imaging, and high clinical suspicion of pulmonary cryptococcosis. Our first patient had a positive BAL and blood culture for
According to a 2023 study published in Open Forum Infectious Diseases, disseminated cryptococcosis affects 5% to 8% of HIV-positive individuals who are not on effective antiretroviral therapy. Similar rates are observed among non-HIV immunocompromised patients, including organ transplant recipients and patients with cancer; however, these rates can vary depending on the specific illness and geographic location [4]. A prospective study of 235 cases of proven
In immunocompromised patients, meningoencephalitis is the most common manifestation, even though the lungs are the primary entry site for
The CrAg lateral flow assay is highly sensitive and specific (approximately 95%). However, false-negative results can occur due to hemolysis or the postzone effect, which happens when antigen and antibody concentrations are not balanced. To minimize this, additional dilutions of the specimen are performed to achieve the zone of equivalency. Despite these measures, the CrAg test can still be negative in cases of low fungal burden or when the
In cases in which patients have CrAg-positive results but lack symptoms of meningitis, the challenge lies in interpreting negative CNS findings despite positive blood cultures. World Health Organization guidelines recommend a preemptive course of fluconazole (800 mg/day for 2 weeks, then 400 mg/day for 8 weeks, and finally 200 mg/day pending immune reconstitution with antiretroviral therapy) for CrAg-positive patients. However, studies, including that of Wake et al, show that CrAg-positive patients remain at risk for cryptococcal meningitis and related mortality. Their research indicates that a CrAg titer of 1: 160 is associated with CNS involvement, suggesting that such patients should be treated as if they have meningitis [10]. In our cases, both patients had CrAg titers of 1: 80 in BAL and serum, respectively. Despite negative lumbar punctures for CNS infection, positive blood cultures for
Our first patient was initially started on fluconazole after a negative lumbar puncture. However, based on the European Confederation for Medical Mycology/International Society for Human and Animal Mycology/American Society for Microbiology Global Guidelines for the Diagnosis and Management of Cryptococcosis [11], the treatment was escalated to standard induction therapy with amphotericin B and flucytosine. This decision was driven by the positive blood culture for
In contrast, our second patient, who was HIV-positive, presented with severe respiratory symptoms. Although the BAL was suggestive of PJP and negative for
Conclusions
These cases highlight rare presentations of disseminated cryptococcal infection without CNS involvement, characterized by low serum CrAg titers (1: 80) and positive blood cultures. They emphasize the importance of considering disseminated disease even when serum antigen levels are low and CNS symptoms are absent. Positive blood cultures were key to diagnosis and guided the need for aggressive antifungal therapy. These findings support greater clinical vigilance and the role of blood cultures in managing atypical cryptococcosis presentations. Factors such as strain variations, low fungal burden, and unique immune responses can contribute to these unusual findings. Future research should explore these mechanisms, evaluate current CrAg titer thresholds, and refine diagnostic and treatment protocols, to improve outcomes and inform clinical guidelines.
Figures
![Culture of Cryptococcus neoformans on Sabouraud dextrose agar and blood agar platesThis figure shows mucoid, creamy, smooth colonies characteristic of Cryptococcus neoformans on Sabouraud dextrose agar (culture plates A, B, D]) and blood agar (culture plate C) media. These colony morphologies are indicative of fungal growth.](https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e946589-g001.jpg&idArt=946589&w=1000) Figure 1. Culture of Cryptococcus neoformans on Sabouraud dextrose agar and blood agar platesThis figure shows mucoid, creamy, smooth colonies characteristic of Cryptococcus neoformans on Sabouraud dextrose agar (culture plates A, B, D]) and blood agar (culture plate C) media. These colony morphologies are indicative of fungal growth.
Figure 1. Culture of Cryptococcus neoformans on Sabouraud dextrose agar and blood agar platesThis figure shows mucoid, creamy, smooth colonies characteristic of Cryptococcus neoformans on Sabouraud dextrose agar (culture plates A, B, D]) and blood agar (culture plate C) media. These colony morphologies are indicative of fungal growth. 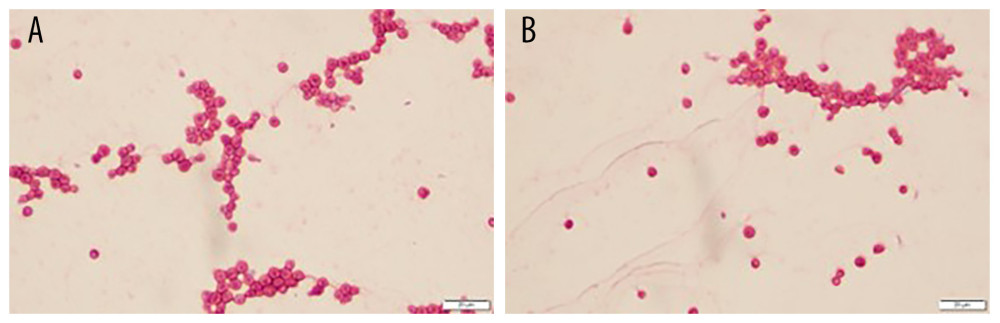 Figure 2. Gram stain of Cryptococcus neoformans from blood culture(A, B) These panels show Gram-stained images revealing narrow-based budding yeast forms consistent with Cryptococcus neoformans. The organisms appear as thin-walled, encapsulated yeast with varying sizes, seen in clusters.
Figure 2. Gram stain of Cryptococcus neoformans from blood culture(A, B) These panels show Gram-stained images revealing narrow-based budding yeast forms consistent with Cryptococcus neoformans. The organisms appear as thin-walled, encapsulated yeast with varying sizes, seen in clusters. References
1. Mada PK, Cryptococcosis: Medscape.com October 28, 2024 Available from: https://emedicine.medscape.com/article/1167389-overview
2. Mada PK, Jamil RT, Alam MU, Cryptococcus. [Updated 2023 Aug 7]: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing Available from: https://www.ncbi.nlm.nih.gov/books/NBK431060/
3. Vilchez RA, Fung J, Kusne S, Cryptococcosis in organ transplant recipients: An overview: Am J Transplant, 2002; 2(7); 575-80
4. Roman-Montes CM, Velez-Pintado M, Seoane-Hernandez L, 847. Cryptococcal disease in HIV and non-HIV-infected patients: Clinical features and outcome: Open Forum Infect Dis, 2023; 10(Suppl 2); ofad500.892
5. Davis JA, Horn DL, Marr KA, Fishman JA, Central nervous system involvement in cryptococcal infection in individuals after solid organ transplantation or with AIDS: Transpl Infect Dis, 2009; 11(5); 432-37
6. Meena P, Bhargava V, Singh K, Cryptococcosis in kidney transplant recipients: Current understanding and practices: World J Nephrol, 2023; 12(5); 120-31
7. Borba-Santos LP, Reis de Sá LF, Ramos JA: Front Microbiol, 2017; 8; 1759
8. Jean SS, Fang CT, Shau WY, Cryptococcaemia: Clinical features and prognostic factors: QJM, 2002; 95(8); 511-18
9. Misra A, Yetmar ZA, Milone AA, The brief case: The cryptic cryptococcus: J Clin Microbiol, 2023; 61(2); e0054822
10. Wake RM, Britz E, Sriruttan C, High cryptococcal antigen titers in blood are predictive of subclinical cryptococcal meningitis among human immunodeficiency virus-infected patients: Clin Infect Dis, 2018; 66(5); 686-92
11. Chang CC, Harrison TS, Bicanic TA, Global guideline for the diagnosis and management of cryptococcosis: An initiative of the ECMM and ISHAM in cooperation with the ASM: Lancet Infect Dis, 2024; 24(8); e495-e512 Erratum in: Lancet Infect Dis. 2024;24(8):e485
12. Subahi EA, Aljafar MS, Barjas HH: Clin Case Rep, 2021; 9(7); e04191
Figures
Figure 1. Culture of Cryptococcus neoformans on Sabouraud dextrose agar and blood agar platesThis figure shows mucoid, creamy, smooth colonies characteristic of Cryptococcus neoformans on Sabouraud dextrose agar (culture plates A, B, D]) and blood agar (culture plate C) media. These colony morphologies are indicative of fungal growth.Figure 2. Gram stain of Cryptococcus neoformans from blood culture(A, B) These panels show Gram-stained images revealing narrow-based budding yeast forms consistent with Cryptococcus neoformans. The organisms appear as thin-walled, encapsulated yeast with varying sizes, seen in clusters. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133