06 May 2025: Articles 
Miliary Patterns on Computerized Tomography Imaging of Chest in Immunocompromised Patient: Unveiling Disseminated Histoplasmosis
Challenging differential diagnosis
Sravani Kamatam E 1*, Anusha Akepati B 1, Divya Shivakumar EF 2DOI: 10.12659/AJCR.946631
Am J Case Rep 2025; 26:e946631






Abstract
BACKGROUND: Disseminated histoplasmosis is a rare fungal infection caused by dimorphic fungus Histoplasma capsulatum. Immunocompetent patients are usually asymptomatic or have self-limiting disease; however, immunocompromised patients present as disseminated infection. Our case report includes an immunocompromised host with atypical presentation and imaging findings consistent with a miliary pattern that did not fit the classical clinical picture of disseminated histoplasmosis, causing a delay in the diagnosis.
CASE REPORT: We report a case of a patient who presented with shortness of breath, nonproductive cough, low-grade fevers, and weight loss, who received a diagnosis of disseminated histoplasmosis, with an underlying immunocompromised state. Due to the ineffectiveness of initial management with empiric antibiotics, imaging with computed tomography (CT) of the chest was done, revealing miliary disease, and tuberculosis was first in the differential diagnosis. She had a positive histoplasma urine antigen, and bronchial alveolar lavage fluid tested positive for histoplasma antigen, confirming miliary histoplasmosis. Her CT of the abdomen/pelvis showed multiple lesions in the spleen and adrenal glands bilaterally, concerning for disseminated histoplasmosis, which was treated with amphotericin B, followed by itraconazole.
CONCLUSIONS: Disseminated histoplasmosis is a rare and challenging diagnosis; there should be a low suspicion for histoplasmosis in patients treated with tumor necrosis factor inhibitors, as mortality is high in such cases. Despite the inability to detect antibodies in immunocompromised patients, definitive diagnostic tests must be considered through culture and histopathology, the criterion standard tests, before excluding infectious causes. This case highlights the challenges faced in diagnosing and treating miliary histoplasmosis in immunocompromised patients.
Keywords: Histoplasmosis, Immunocompromised Host, Tuberculosis, Humans, Tomography, X-Ray Computed, Female, Middle Aged, Diagnosis, Differential, Antifungal Agents, Histoplasma
Introduction
One granulomatous disease that relentlessly progresses and mimics many other granulomatous diseases, including tuberculosis, especially in immunocompromised patients, is disseminated histoplasmosis. Histoplasmosis is caused by
Case Report
An 81-year-old woman with a past medical history of rheumatoid arthritis presented to the hospital for shortness of breath for about 2 to 3 weeks and an associated non-productive cough. She also had associated low-grade fever, decreased appetite, and weight loss. The patient had been following up with the rheumatology clinic for her rheumatoid arthritis, and her active treatment for rheumatoid arthritis included denosumab, ibuprofen, methotrexate, folic acid, and intravenous (i.v.) golimumab. Before this, she was on i.v. infliximab and abatacept, which did not help her much. She was afebrile, saturating well on room air, and hemodynamically stable on admission. On physical examination, she had new-onset mild crackles in both lung fields, but the examination was otherwise unremarkable. Initial laboratory work-up showed a white blood cell count of 6.07×103/mcL, hemoglobin of 14 g/dL, elevated liver enzymes with aspartate transaminase level of 40 U/L, alkaline phosphatase level of 152 U/L, mild hyponatremia with sodium level of 128 mmol/L, and elevated lactate dehydrogenase level of 417 U/L. The initial chest radiograph showed chronic-appearing coarse lung opacities bilaterally, with no other acute cardiopulmonary abnormality. She was started on empiric treatment for community-acquired pneumonia, given her symptoms. Despite this, her shortness of breath did not improve, and given her immunocompromised state, a CT of the chest without contrast was ordered on day 3 of admission, which showed multiple bilateral pulmonary nodules and miliary disease throughout the lungs, as shown in Figure 1, with yellow arrows depicting the miliary nodules. Differential diagnoses included tuberculosis, fungal infections, metastases, sarcoidosis, pneumoconiosis, hypersensitivity pneumonitis, and Langerhans cell histiocytosis. Miliary tuberculosis was first in the differential, given the classic distribution of the nodules in a miliary pattern. She was placed under droplet isolation, and 3 sputum acid-fast bacilli cultures were collected and sent. The Pulmonology Department was consulted because the chest CT findings were concerning for miliary tuberculosis. The case was discussed with the Infectious Disease Department, which recommended to order a fungal antibody panel and fungitell and urine histoplasma antigen, given the symptoms, immunosuppression, and miliary pattern on imaging findings. The patient had a positive histoplasma urine antigen of 0.9 ng/mL, and the reportable range for this assay is 0.2 to 25 ng/mL. She underwent bronchoscopy, which showed mucosal pallor throughout, with no endobronchial lesions and minimal, thin, and white secretions present in the trachea, main carina, left lung, and right lung, as shown in Figure 2A–2C, marked with red arrows. Secretions were easily removed by therapeutic aspiration, and the airway was cleared. Bronchoalveolar lavage was performed 1 time in the right middle lobe, with 120 mL of saline instilled and a total return of 60 mL. The fluid appeared clear, as shown in Figure 2D, marked with a red arrow. Bronchoalveolar lavage samples were sent for acid-fast bacilli and fungal cultures. All initial cultures were negative, and later, bronchial alveolar lavage fluid tested positive for the histoplasma antigen, further confirming miliary histoplasmosis. A GeneXpert test was non-detectable for
Discussion
Miliary pattern is the presence of diffuse lung nodules on chest imaging that resemble millet seeds and occur due to lymphohematogenous dissemination and ineffective response of cellular defense mechanisms or an underlying infiltrative process that spreads through the lung interstitium [5]. It is an uncommon presentation but is increasingly seen in clinical practice, given the rise of the immunocompromised and immunosuppressed patient population. The miliary pattern is a characteristic radiological manifestation of micronodular lung disease, and the common entities causing this pattern are infectious, immune or inflammatory, pneumoconiosis, and malignancy. This pattern, when seen, is characteristically interpreted as miliary tuberculosis [8]. However, given the increase in the population of immunocompromised patients, other causes, such as disseminated fungal infections, need to be evaluated to increase diagnostic accuracy and early treatment. Histoplasmosis has become the most common fungal infection among patients treated with TNF antagonists for rheumatoid arthritis, inflammatory bowel disease, and dermatological disease [9]. Immunocompromised hosts are more likely to have severe disease than are immunocompetent hosts, and disseminated infection is a more common clinical picture among immunocompromised hosts [10]. Radiological investigations in disseminated histoplasmosis show characteristic signs of fibrosing mediastinitis compressing major vessels, and other organ involvement typically seen is acromegaly, hepatosplenomegaly, and mediastinal and abdominal lymphadenopathy [11]. CT findings of pulmonary histoplasmosis are varied and nonspecific, with acute cases showing diffuse bilateral opacities, subacute cases presenting focal opacities that may calcify, and severe cases, especially in immunosuppressed patients, leading to extrapulmonary dissemination with pericarditis, hepatosplenomegaly, skin changes, and rheumatologic disorders. Pulmonary histoplasmosis commonly presents as solitary or multiple nodules, often mimicking malignancy, while CT findings in acute cases can show irregular consolidation resembling bacterial pneumonia, organizing pneumonia, or neoplasia. Chronic cavitary histoplasmosis, which is rare and typically seen in patients with chronic obstructive pulmonary disease, presents as upper lobe consolidation with progressive cavitation, volume loss, and pleural thickening, resembling tuberculosis. Disseminated histoplasmosis, primarily in immunocompromised patients, manifests as diffuse pulmonary micronodules or airspace opacities, often mimicking miliary tuberculosis or metastatic disease [12].
Miliary histoplasmosis is seen in immunocompromised patients and is caused by
Histopathology and culture are criterion standards for the diagnosis of histoplasmosis. Given the sensitivity of histopathology and cultures, diagnosis is delayed, as there is a need for invasive procedures for sample collection and a delay in the growth of organisms [18]. Diagnosis is made by visualizing yeast on histopathology, isolating organisms from sputum culture, or detecting histoplasma antigens. Detection of yeast in cultures and DNA probes can take around 4 weeks, delaying the diagnosis. Also, there is a high chance of cross-reactivity of the histoplasma antigen with other fungal antigens, leading to misdiagnosis, as seen in a case report in which fungal antigen was positive for coccidioidomycosis antigen in an HIV-positive patient, but ultimately, the culture was positive for histoplasmosis [19]. Histoplasmosis is generally treated with antifungal medications, such as azoles. Itraconazole was the preferred choice, but with central nervous system involvement, as per IDSA guidelines, voriconazole, posaconazole, isavuconazole, and fluconazole can be given as the treatment of choice [20]. Some studies show that fungal burden clearance in disseminated histoplasmosis was better with amphotericin B, and this drug is also widely used in the treatment of disseminated histoplasmosis [21].
Radiographic improvement in histoplasmosis varies with disease severity and patient immune status. In acute pulmonary histoplasmosis, chest radiographs often show patchy pneumonia in one or more lobes, with enlarged hilar and mediastinal lymph nodes. Improvement is prompt in most cases, with treatment showing disappearance or decrease in the miliary nodules; however, in some patients, clinically, fatigue can linger for several months [22]. In chronic pulmonary histoplasmosis, chest radiographs often reveal emphysematous lungs, with apical bullae surrounded by segmental airspace disease. Progressive thickening of cavity walls and retraction of adjacent lung tissue occurs over time [23]. Overall, radiographic improvement depends on the histoplasmosis form, disease severity, and patient’s immune status. Monitoring radiographic changes is essential for assessing treatment response and disease progression, and our patient showed a clear radiographic improvement on the 3-month follow-up after initiation of treatment.
Conclusions
This case highlights the challenges faced in diagnosing and treating miliary histoplasmosis in immunocompromised patients. Miliary nodules in the lung can be seen in a host of other infectious conditions other than miliary tuberculosis and need to be considered in patients with miliary pulmonary nodules. As clinical presentation is similar in all these infectious conditions, careful history regarding exposure and immunocompromised states should be considered. Despite the inability to detect antibodies in immunocompromised patients, definitive diagnostic tests need to be considered before the exclusion of other infectious causes, through culture and histopathology, which are the criterion standard tests. There should be a low suspicion for histoplasmosis in patients treated with TNF inhibitors, as mortality is reportedly high in such cases and early diagnosis and appropriate antifungal therapy initiation will have a good response.
Figures
 Figure 1. Axial plane view of computed tomography of the chest without contrast showing multiple bilateral pulmonary nodules and miliary disease throughout the lungs. Yellow arrows show miliary nodules.
Figure 1. Axial plane view of computed tomography of the chest without contrast showing multiple bilateral pulmonary nodules and miliary disease throughout the lungs. Yellow arrows show miliary nodules.  Figure 2. (A–D) Bronchoscopy images showing minimal, thin, and white secretions marked with a red arrow in the trachea, main carina, left lung, and right lung. Bronchoalveolar lavage was performed in the right middle lobe.
Figure 2. (A–D) Bronchoscopy images showing minimal, thin, and white secretions marked with a red arrow in the trachea, main carina, left lung, and right lung. Bronchoalveolar lavage was performed in the right middle lobe. 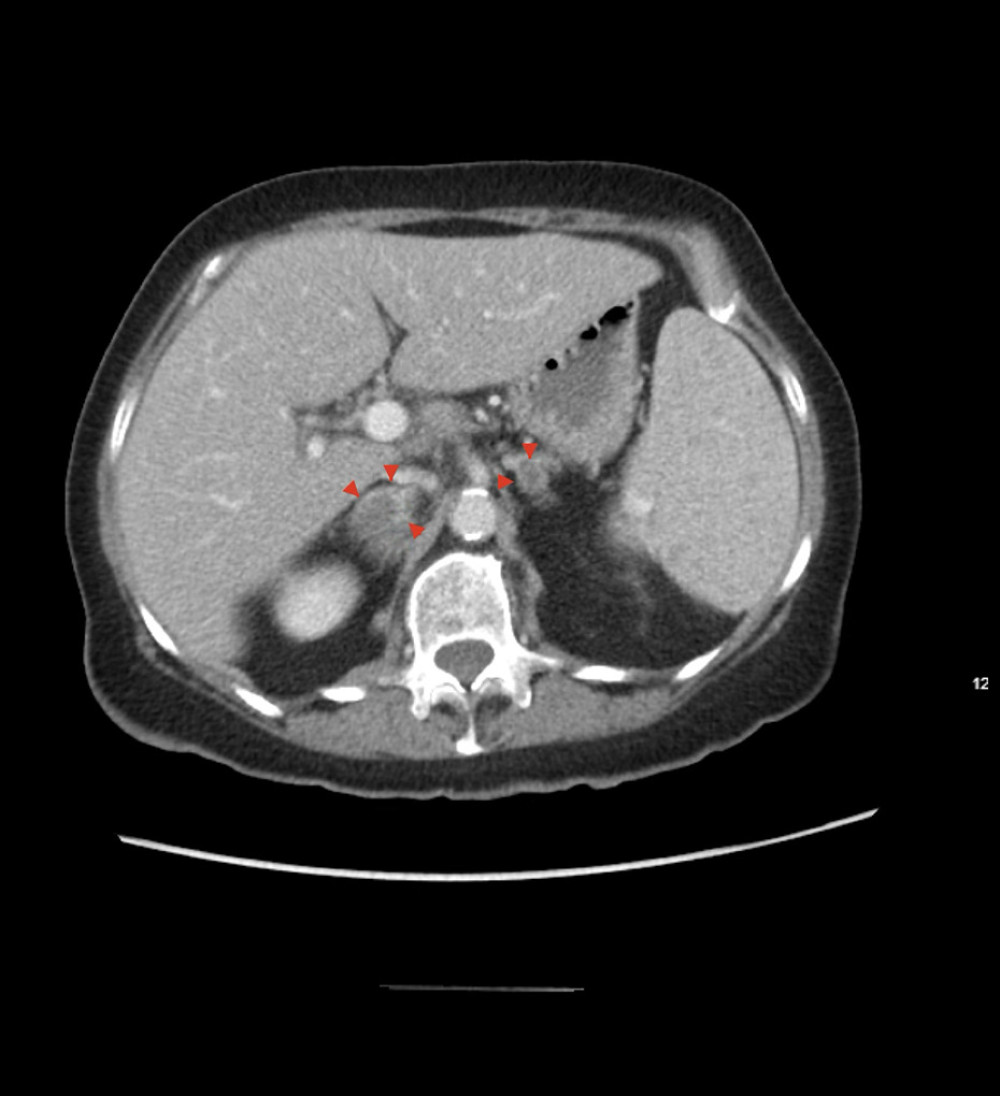 Figure 3. Axial plane view of computed tomography of the abdomen and pelvis with contrast image showing bilateral adrenal nodules. Red arrows depict right adrenal nodule measuring 3×1 cm and left adrenal nodule measuring 9 mm.
Figure 3. Axial plane view of computed tomography of the abdomen and pelvis with contrast image showing bilateral adrenal nodules. Red arrows depict right adrenal nodule measuring 3×1 cm and left adrenal nodule measuring 9 mm.  Figure 4. Axial plane view of computed tomography of the chest with contrast image showing a majority of the previously seen diffuse pulmonary nodules have resolved, compatible with inflammation/infection. Yellow arrows depict the same.
Figure 4. Axial plane view of computed tomography of the chest with contrast image showing a majority of the previously seen diffuse pulmonary nodules have resolved, compatible with inflammation/infection. Yellow arrows depict the same.  Figure 5. Axial plane view of computed tomography of the abdomen and pelvis with contrast image showing decreased size in the right adrenal nodule and stable left adrenal nodule, depicted with red arrows.
Figure 5. Axial plane view of computed tomography of the abdomen and pelvis with contrast image showing decreased size in the right adrenal nodule and stable left adrenal nodule, depicted with red arrows. References
1. Chu JH, Feudtner C, Heydon K, Hospitalizations for endemic mycoses: A population-based national study: Clin Infect Dis, 2006; 42(6); 822-25
2. Agudelo CA, Restrepo CA, Molina DA, Tuberculosis and histoplasmosis co-infection in AIDS patients: Am J Trop Med Hyg, 2012; 87(6); 1094-98
3. Azar MM, Hage CA, Clinical perspectives in the diagnosis and management of histoplasmosis: Clin Chest Med, 2017; 38(3); 403-15
4. Muñoz C, Gómez BL, Tobón A, Validation and clinical application of a molecular method for identification of Histoplasma capsulatum in human specimens in Colombia, South America: Clin Vaccine Immunol, 2010; 17(1); 62-67
5. Sharma BB, Miliary nodules on chest radiographs: A diagnostic dilemma: Lung India, 2015; 32(5); 518-20
6. Lum J, Abidi ZM, McCollister B, Henao-Martínez AF, Miliary histoplasmosis in a patient with rheumatoid arthritis: Case Rep Med, 2018; 2018; 2723489
7. Hage CA, Ribes JA, Wengenack NL, A multicenter evaluation of tests for diagnosis of histoplasmosis: Clin Infect Dis, 2011; 53(5); 448-54
8. Furqan M, Butler J, Miliary pattern on chest radiography: TB or not TB?: Mayo Clin Proc, 2010; 85(2); 108
9. Crum NF, Lederman ER, Wallace MR, Infections associated with tumor necrosis factor-alpha antagonists: Medicine (Baltimore), 2005; 84(5); 291-302
10. Kauffman CA, Diagnosis of histoplasmosis in immunosuppressed patients: Curr Opin Infect Dis, 2008; 21(4); 421-25
11. Grover SB, Grover H, Antil N, Imaging approach to pulmonary infections in the immunocompromised patient: Indian J Radiol Imaging, 2022; 32(1); 81-112
12. Mango ALD, Gomes ACP, Hochhegger B, Computed tomography findings of pulmonary histoplasmosis: Pictorial essay: Radiol Bras, 2023; 56(3); 162-67
13. McKinsey DS, McKinsey JP, Pulmonary histoplasmosis: Semin Respir Crit Care Med, 2011; 32(6); 735-44
14. Wheat LJ, Approach to the diagnosis of the endemic mycoses: Clin Chest Med, 2009; 30(2); 379-89
15. Sharma SK, Mohan A, Sharma A, Challenges in the diagnosis & treatment of miliary tuberculosis: Indian J Med Res, 2012; 135(5); 703-30
16. Voloudaki AE, Tritou IN, Magkanas EG, HRCT in miliary lung disease: Acta Radiol, 1999; 40(4); 451-56
17. Gaillard F, Yu Y, Altadill A, Miliary opacities (lungs): Reference article, Radiopaedia.org Available from: https://doi.org/10.53347/rID-1679
18. Wheat LJ, Improvements in diagnosis of histoplasmosis: Expert Opin Biol Ther, 2006; 6(11); 1207-21
19. Myint T, Leedy N, Villacorta Cari E, Wheat LJ, HIV-associated histoplasmosis: Current perspectives: HIV AIDS (Auckl), 2020; 12; 113-25
20. Mazi PB, Arnold SR, Baddley JW, Management of histoplasmosis by infectious disease physicians: Open Forum Infect Dis, 2022; 9(7); ofac313
21. Wheat LJ, Cloud G, Johnson PCAIDS Clinical Trials Group; Mycoses Study Group of NIAID, Clearance of fungal burden during treatment of disseminated histoplasmosis with liposomal amphotericin B versus itraconazole: Antimicrob Agents Chemother, 2001; 45(8); 2354-57
22. Kauffman CA, Histoplasmosis: A clinical and laboratory update: Clin Microbiol Rev, 2007; 20(1); 115-32
23. Kurowski R, Ostapchuk M, Overview of histoplasmosis: Am Fam Physician, 2002; 66(12); 2247-52
Figures
Figure 1. Axial plane view of computed tomography of the chest without contrast showing multiple bilateral pulmonary nodules and miliary disease throughout the lungs. Yellow arrows show miliary nodules.Figure 2. (A–D) Bronchoscopy images showing minimal, thin, and white secretions marked with a red arrow in the trachea, main carina, left lung, and right lung. Bronchoalveolar lavage was performed in the right middle lobe.Figure 3. Axial plane view of computed tomography of the abdomen and pelvis with contrast image showing bilateral adrenal nodules. Red arrows depict right adrenal nodule measuring 3×1 cm and left adrenal nodule measuring 9 mm.Figure 4. Axial plane view of computed tomography of the chest with contrast image showing a majority of the previously seen diffuse pulmonary nodules have resolved, compatible with inflammation/infection. Yellow arrows depict the same.Figure 5. Axial plane view of computed tomography of the abdomen and pelvis with contrast image showing decreased size in the right adrenal nodule and stable left adrenal nodule, depicted with red arrows. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133