06 April 2025: Articles 
Delayed Diagnosis of Peritoneal Mesothelioma in Recurrent Ascites: A Case Report
Challenging differential diagnosis
Hafiz Javed ABEF 1, Arfa Ahmad ADEF 1, Abdul RehmanDOI: 10.12659/AJCR.946777
Am J Case Rep 2025; 26:e946777






Abstract
BACKGROUND: Ascites is a common clinical sign noted in 3% to 4% of hospitalized medical patients. Nearly 94% of patients with ascites have non-malignant etiologies, with the most common being chronic liver disease. Peritoneal mesothelioma is an exceedingly rare malignancy associated with asbestos exposure. Here, we report the case of an elderly man who presented with recurrent loculated ascites and received a diagnosis of peritoneal mesothelioma after a delay of approximately 10 weeks.
CASE REPORT: A 67-year-old man with a history of asbestos exposure presented with abdominal distension and muscle wasting for 1 month. Initial abdominal CT was notable for smooth liver contour and massive ascites. Ascitic fluid analysis was consistent with low serum albumin-ascites gradient but showed negative cytology for malignant cells. Upper and lower endoscopies did not reveal lesions. Due to recurring ascites, serial abdominal paracenteses were performed, although cytology was negative for malignant cells. Repeat abdominal CT performed after 6 weeks showed worsening loculated ascites, with possible peritoneal carcinomatosis. At this point, percutaneous omental biopsy was performed, which established the diagnosis of peritoneal mesothelioma (75 days after initial presentation).
CONCLUSIONS: In patients presenting with recurrent ascites and a history of asbestos exposure, it is important to consider the diagnosis of peritoneal mesothelioma. While 94% of patients with ascites have non-malignant etiologies, a small proportion of patients can have malignant ascites. In patients in which the first set of ascitic fluid studies are inconclusive, repeat abdominal paracentesis and omental biopsy or diagnostic laparoscopy should be expedited to avoid delays in diagnosis.
Keywords: asbestosis, Ascites, Mesothelioma, Peritoneal Neoplasms, Humans, Male, Aged, delayed diagnosis, Mesothelioma, Malignant, Recurrence, Tomography, X-Ray Computed, lung neoplasms
Introduction
Ascites, the presence of an excess amount of fluid within the peritoneal cavity, is a common sign of chronic liver disease and can be noted in about 3% to 4% of hospitalized patients on general medical wards [1]. While close to 94% of patients with ascites have non-malignant etiologies of ascites, a small proportion of patients can have malignant ascites [1,2]. Diagnostic work-up of new-onset ascites requires an abdominal paracentesis for ascitic fluid analysis. The serum albumin-ascites gradient (SAAG) is an important quantitative measure that helps to differentiate between portal hypertension-related ascites (SAAG >1.1 g/dL) and ascites due to other causes (SAAG <1.1 g/dL), with high accuracy [1–3]. Among the causes of low-SAAG ascites, malignancy, infections (especially tuberculosis), nephrotic syndrome, acute pancreatitis, and perforated viscus are commonly implicated [4]. Peritoneal mesothelioma, a malignant tumor arising from the serosal lining of the peritoneum, is an exceptionally rare cause of ascites [5].
Mesothelioma is an exceedingly rare malignancy that is notoriously difficult to diagnose [5] and responsible for 26 278 deaths globally, with the greatest number of deaths occurring in the United States [6]. Mesothelioma occurs in the pleural cavity in 90% of cases [5]. Asbestos, classified as a group 1 carcinogen by the World Health Organization (WHO), is strongly implicated in the pathogenesis of mesothelioma [6]. Peritoneal mesothelioma often presents with vague clinical symptoms, including bloating, weight loss, night sweats, and abdominal distension. Moreover, the diagnosis is complicated by the fact that ascitic fluid cytology yield for malignant cells is only about 50% [7]. In such cases, diagnostic laparoscopy with biopsy is necessary to establish the diagnosis [2]. The interpretation of the biopsy itself requires experienced pathologists as well as a combination of immunohistochemical stains and cytogenetic testing [5,7]. Given the difficulties faced in the diagnosis of peritoneal mesothelioma, a delay in diagnosis can lead to increased patient morbidity and mortality [8].
Previously reported cases of peritoneal mesothelioma have documented its rare clinical manifestations and described novel treatment strategies in specific clinical scenarios [8–11]. However, delayed diagnosis of peritoneal mesothelioma in a patient with recurring ascites has not been highlighted before. The present case report is about a 67-year-old man who had a history of significant occupational asbestos exposure and presented with low-SAAG ascites. He underwent multiple abdominal paracenteses as well as upper and lower endoscopies before the diagnosis was finally established by an omental biopsy, after a delay of approximately 10 weeks. This case highlights the challenges faced in establishing a diagnosis of peritoneal mesothelioma and the delay caused by not considering this diagnosis earlier. The present case highlights the importance of considering this diagnosis in patients with a history of asbestos exposure and suggestive symptoms. Moreover, it reminds clinicians to recognize that a single ascitic fluid analysis can be insufficient for making a diagnosis of peritoneal mesothelioma. Additionally, it underscores the importance of pursuing omental biopsy and/or laparoscopy in patients with loculated ascites when the diagnosis remains unclear after initial testing and ascitic fluid analysis.
Case Report
A 67-year-old man with a past medical history of occupational asbestos exposure presented to the Emergency Department of our hospital in June 2024 with concerns of weight loss and abdominal distention for 4 weeks. The patient reported that he had been well prior to the onset of these symptoms. He denied any alterations in bowel habits, melena, hematochezia, abdominal pain, nausea, vomiting, dysphagia, and odynophagia. He did endorse having loss of appetite and had lost 8.2 kg over the 4 weeks prior to the current presentation. He denied any prior history of tuberculosis or contact with anyone known to have tuberculosis. He was born in the United States and had been exposed to asbestos while working for a shipbuilding company. He denied any history of cigarette smoking or exposure to organic dusts. He had a pet dog but denied any history of exposure to pet birds or other exotic pets. He was not taking any regular medications; however, he had not seen a physician for about 2 years prior to the current presentation. There was no reported history of any drug allergies. Although his family history was notable for coronary artery disease, there was no known history of cancers in his parents or siblings.
On initial presentation, his vital signs were within normal limits. His physical examination was remarkable for bitemporal wasting, conjunctival pallor, and shifting dullness, suggestive of ascites. His laboratory investigations were remarkable for normochromic normocytic anemia (hemoglobin 11.8 g/dL with mean corpuscular volume 85 fL) and hypoalbuminemia (serum albumin 2.1 g/dL). His results of liver function tests, serum creatinine, and electrolyte levels were within the reference range. On presentation, computed tomography (CT) of the abdomen and pelvis (with contrast) was notable for massive ascites, smooth contour of liver, and a large nodule in the left lower lobe of lung, along with central calcification (Figure 1). At this point, the diagnostic considerations included all etiologies of new-onset ascites in an elderly man, such as chronic liver disease, right-sided heart failure, peritoneal tuberculosis, and malignant ascites. Given that chronic liver disease is the most common cause of ascites, an abdominal paracentesis and abdominal ultrasonography with Doppler studies were ordered.
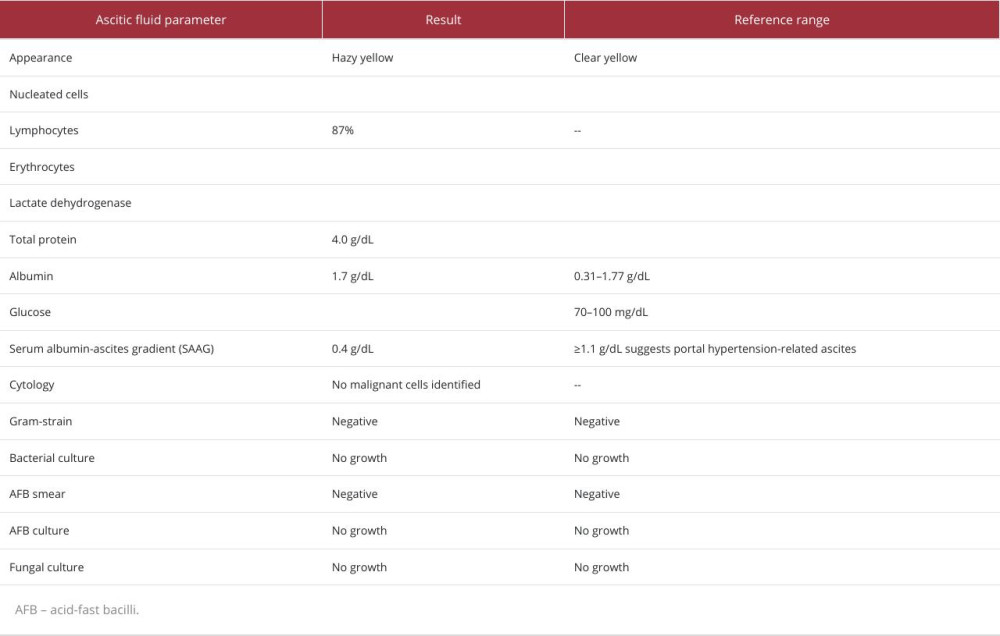
The patient was admitted to the medicine service, and abdominal paracentesis was performed with ultrasound guidance. A total of 14.7 L of hazy yellow ascitic fluid was drained. Ascitic fluid analysis was consistent with an exudative process and a SAAG of 0.8 g/dL (details in Table 1). The urine protein-to-creatinine ratio was suggestive of trace proteinuria (equivalent to <300 mg/day). Transthoracic echocardiography revealed normal indices of right ventricular function and a normal left ventricular ejection fraction. Ultrasonography of the liver revealed smooth liver margins, with normal echotexture.
The portal vein size and Doppler indices were within normal limits. The spleen was not enlarged on ultrasonography. A serum FibroTest-ActiTest (BioPredictive, Inc; Paris, France) was also performed, which was suggestive of no hepatic fibrosis (F0-F1 by FibroTest-ActiTest score). Given the constellation of a low SAAG and absence of findings of portal hypertension, differential diagnosis was narrowed to causes of ascites with a low SAAG. In view of this, further ascitic fluid investigations were ordered on the previously collected fluid, including cytology, gram-stain and culture, acid-fast bacilli (AFB) smear and culture, and fungal culture. A Quantiferon-TB Gold test was also performed, which was negative. As part of work-up for malignant ascites, serum tumor markers (carcinoembryonic agent, alpha-fetoprotein, and carbohydrate antigen 19-9) were sent to screen for any occult gastrointestinal or pancreato-hepato-biliary malignancy. Serum tumor markers were within normal limits, although this alone was not sufficient to exclude a diagnosis of peritoneal carcinomatosis. Given that the ascitic fluid investigations would take several days to result, the patient was discharged home with a plan for outpatient follow-up with primary care, gastroenterology, and pulmonology.
The patient followed up with his primary care physician 1 week after discharge, and he was noted to have recurrence of ascites. At this time, peritoneal fluid cytology had resulted and was negative for any malignant cells, but showed only reactive mesothelial cells. Ascitic fluid gram-stain and culture, AFB smear and culture, and fungal smear and culture were all negative as well. At this point, the differential diagnosis had been narrowed down to exudative causes of low-SAAG ascites, chiefly malignant ascites versus chronic indolent infections (mycobacterial or fungal infections). The patient’s primary care physician referred the patient to the Interventional Radiology Department for therapeutic abdominal paracentesis but did not order any repeat ascitic fluid studies. Moreover, the patient already had an appointment in the pulmonary and gastroenterology clinics, but these appointments were scheduled for more than 7 weeks later. Till the patient’s next follow-up visit, he underwent a total of 4 abdominal paracentesis on days 14, 23, 31, and 46 after his initial presentation (timeline in Figure 2). Unfortunately, no cytology specimens or additional fluid analyses were ordered on the fluid drained.
Almost 8 weeks after initial presentation, the gastroenterology team evaluated the patient in the clinic and scheduled him for upper and lower endoscopies to assess for any occult malignancy. Although the patient had negative tumor markers, peritoneal carcinomatosis in men is most commonly caused by occult malignancies of the gastrointestinal tract; this was the rationale for pursuing esophagogastroduodenoscopy and colonoscopy. Moreover, the gastroenterology team ordered peritoneal fluid cytology to be sent again with the next abdominal paracentesis. Repeat sampling of ascitic fluid was ordered, as multiple samples can increase the yield of cytology as well as AFB culture. Additionally, the patient was referred to the general surgery clinic for further work-up, including a diagnostic laparoscopy. The rationale for this was that the most definitive, albeit invasive, modality to establish a diagnosis in cases of low-SAAG exudative ascites is laparoscopy with targeted biopsies. A follow-up CT scan of the abdomen and pelvis with contrast was also ordered to assist in planning for laparoscopy with peritoneal biopsy. At this point, the patient was also seen in the pulmonary clinic for his large calcified pulmonary nodule, which was believed to be a benign lesion – given that macro-calcifications within a pulmonary nodule are consistent with dystrophic (benign) calcification. In view of a negative Quantiferon-TB Gold test and no obvious risk factors for peritoneal tuberculosis, malignant ascites was considered the most likely diagnosis at this time.
Repeat CT of the abdomen and pelvis with contrast (Figure 3) showed findings of loculated ascites, omental caking, and a large left-sided pleural effusion. The patient underwent upper and lower endoscopies, which did not reveal any malignant lesions. Although peritoneal carcinomatosis and malignant ascites was still a consideration, occult gastrointestinal tract malignancies were deemed less likely in view of the findings of the endoscopies. The patient was evaluated in the general surgery clinic at this point (2 months after initial presentation), and diagnostic laparoscopy was deemed to be too risky because of probable peritoneal carcinomatosis with omen-tal caking. The general surgery team recommended hospital admission for further evaluation and possible percutaneous omental biopsy. The patient underwent abdominal paracentesis for repeat cytology as well as a percutaneous omental biopsy. Ascitic fluid cytology revealed atypical mesothelial cells that were positive for CK5/6, D2-40 (podoplanin), and calretinin and negative for MOC-31. Omental biopsy revealed epithelioid tumor cells with an infiltrative pattern and cellular atypia (Figure 4), which were positive for AE1/3, CK5/6, CK7, calretinin, D2-40, WT1, and BAP1 but negative for MOC31, synaptophysin, chromogranin, TTF-1, CDX2, and CK20. Based on the histopathological features, a diagnosis of peritoneal epithelioid mesothelioma was made, 75 days after the patient’s initial presentation. Tuberculosis or other infectious etiologies of ascites were definitively excluded by the results of omental biopsy. Moreover, immunohistochemical staining was instrumental in excluding peritoneal carcinomatosis or metastases from gastrointestinal carcinomas as the cause of malignant ascites. The interventional pulmonary team also performed a left-sided thoracentesis, with the insertion of an indwelling pleural catheter for palliation. Pleural fluid cytology was also positive for malignant cells, with identical markers confirming that this was a malignant pleural effusion associated with the peritoneal mesothelioma.
After the diagnosis of peritoneal mesothelioma was established, the oncology team was consulted, and magnetic resonance imaging (MRI) of the abdomen and pelvis without and with contrast was performed. MRI re-demonstrated findings of loculated ascites, and omental thickening and enhancement concerning for peritoneal carcinomatosis (Figure 3). The oncology team offered the option of cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy (HIPEC) to the patient. The patient reported that he was living with his wife, who also had medical problems of her own, and the patient did not want to become a burden on his wife. He felt that he had already lived a happy and fulfilling life. He valued independence and quality of life over prolonging life at the cost of invasive interventions. In view of his values and preferences, he opted for hospice care and wished to spend the rest of his life with his wife at home. The patient subsequently died 4 months after his initial presentation.
Discussion
DIAGNOSTIC CONSIDERATIONS:
Peritoneal mesothelioma can present with a variety of symptoms and signs [9]. As in the present case, patients can present with vague constitutional symptoms and be found to have a low-SAAG exudative ascites, suggestive of a peritoneal malignancy. Additionally, patients can be found to have an incidental peritoneal nodule or mass on imaging requiring further evaluation. In the literature, there have been rare case reports of patients presenting with mesothelioma in situ, a precursor lesion to mesothelioma recognized in the WHO Classification of Thoracic Tumors, 2021 [12]. Moreover, in 1 case, a patient received a diagnosis of malignant mesothelioma at the time of liver transplant surgery, which precluded the patient’s transplant candidacy [8]. In patients who present with a peritoneal nodule or mass, a biopsy of the lesion is recommended, if feasible, as it can provide adequate tissue for confirmation of a pathological diagnosis. Moreover, a rare variety of peritoneal mesothelioma – called localized mesothelioma [13] – can present with a single peritoneal nodule. Localized mesothelioma, as opposed to diffuse mesothelioma, is associated with the same histopathological features as those of diffuse mesothelioma but affords a substantially better prognosis. On the other hand, in patients who present with ascites (similar to our case), the initial work-up of ascites with abdominal paracentesis and ascitic fluid analysis is mandatory. If the ascitic fluid analysis reveals an exudative process with low SAAG, cytology should be performed to look for any evidence of malignant cells. While the yield of ascitic fluid cytology is only about 50%, the diagnosis can be established with 80% sensitivity if an adequate number of malignant cells are present. In cases in which cytology is negative or inconclusive, diagnostic laparoscopy is the preferred next step. Laparoscopy by an experienced surgeon would be able to identify subtle signs of peritoneal nodularity, peritoneal carcinomatosis, or other lesions. Moreover, a biopsy specimen can be obtained at the same time, which can provide tissue confirmation of the diagnosis. In rare cases, omental biopsy or exploratory laparotomy can be needed to establish the diagnosis. In the present case, peritoneal cytology was positive for malignant cells on the second specimen, while omental biopsy was conclusive for establishing the diagnosis of epithelioid diffuse mesothelioma.
DIFFERENTIAL DIAGNOSIS:
In patients presenting with new-onset ascites, common etiologies of non-malignant ascites should be considered first. Chronic liver disease is by far the most common cause of ascites and should be considered in all patients with new-onset ascites. SAAG >1.1 g/dL has been shown in earlier studies to have an accuracy of close to 96% for differentiating portal hypertension-related ascites from other causes of ascites [3]. In patients with a SAAG >1.1 g/dL, the first step for the evaluation of chronic liver disease should include liver ultrasonography, including Doppler studies of the portal vein. If overt signs of cirrhosis are not apparent on ultrasonography, further evaluation with liver elastography or even liver biopsy may be needed. Moreover, the criterion standard for diagnosis of portal hypertension is measurement of the portal pressure gradient, although this is rarely performed in clinical practice. A diagnosis of liver cirrhosis along with other manifestations of portal hypertension, such as splenomegaly, presence of portosystemic collaterals or varices, abnormal portal vein Doppler study, and ascites with a SAAG >1.1 g/dL, are sufficient for establishing this diagnosis. In the present case, SAAG was <1.1 g/dL on ascitic fluid analysis and radiographic findings of portal hypertension or liver cirrhosis were absent. These clinical features together with the results of other ascitic fluid studies were considered sufficient to exclude portal hypertension-related ascites.
Among patients with ascites and a SAAG of <1.1 g/dL, “exudative” causes of ascites including chronic infections, such as tuberculosis, and malignancy are considered most likely. An important cause of “transudative” ascites leading to a SAAG <1.1 g/dL is nephrotic syndrome. However, nephrotic syndrome was effectively excluded in this patient with a spot urine protein-to-creatinine ratio, which revealed the equivalent of <300 mg/ day proteinuria. On the other hand, the distinction between malignant ascites and peritoneal tuberculosis can be challenging to make on clinical grounds.
Peritoneal tuberculosis should be considered in all patients with risk factors for tuberculosis, such as residence in a tuberculosis endemic country, history of HIV infection, malnutrition, and exposure to contacts with known tuberculosis. Peritoneal tuberculosis can cause prominent constitutional symptoms, which mimic those caused by peritoneal carcinomatosis and peritoneal mesothelioma. Moreover, peritoneal tuberculosis can cause an elevated ascitic fluid LDH level, low ascitic fluid glucose level, and markedly elevated ascitic fluid protein level. Additionally, an elevated ascitic fluid adenosine deaminase level has been demonstrated to have sensitivity and specificity of >90% for the diagnosis of peritoneal tuberculosis [14], although elevated adenosine deaminase can also be seen in cases of peritoneal mesothelioma. Furthermore, radiographic findings of peritoneal nodularity, omental caking, and peritoneal enhancement can suggest the presence of peritoneal tuberculosis, although all of these findings can also be seen in peritoneal carcinomatosis or mesothelioma. Recent studies have shown that CT-based texture analysis incorporating a radiomics approach can allow differentiation of peritoneal tuberculosis from peritoneal carcinomatosis [15], although this approach is yet to be validated in larger, prospective cohorts. While ascitic fluid smear and culture for AFB is highly specific for peritoneal tuberculosis, the combined sensitivity of ascitic fluid AFB smear and culture are less than 20% [14]. In the present case, a diagnosis of peritoneal mesothelioma was made based on the results of percutaneous omental biopsy along with peritoneal fluid cytology – although the cytology testing on initial ascitic fluid was negative. In previously reported cases of peritoneal mesothelioma, diagnosis was mostly based on results of ascitic fluid cytology, laparoscopy with peritoneal biopsy, and/or exploratory laparotomy with peritoneal biopsy [8–10,16,17]. A review of previously published cases suggests that a history of asbestos exposure significantly increases the pretest likelihood of peritoneal mesothelioma in the presence of loculated ascites [6,8,16].
HISTOPATHOLOGIC FEATURES:
In the 2021 WHO classification of mesothelioma, the term “mesothelioma” was strictly meant to refer to malignant mesothelial neoplasms. Another important point that bears mentioning is that 99% of mesothelioma are “diffuse” mesotheliomas, in that they diffusely involve the lining of the serosal cavity from which they arise. However, in 1% of cases, a single, discrete, well-circumscribed malignant lesion involves a localized area of the lining of the serosal cavity; this is termed “localized” mesothelioma and has a much better prognosis than diffuse mesothelioma. Generally speaking, whenever the term “mesothelioma” is used without any qualifiers, this refers to diffuse mesothelioma unless otherwise specified. In the present case, the patient had diffuse involvement of the serosal lining of the peritoneal cavity as well as a left-sided malignant pleural effusion, which was consistent with diffuse mesothelioma.
Histopathologically, mesothelioma can have 3 major histologic subtypes: epithelioid, biphasic, and sarcomatoid. Moreover, within the epithelioid and sarcomatoid subtypes, tumors can have additional variations in appearance based on neoplastic cell cytoplasmic and nuclear features, presence of necrosis, varying degrees of infiltration or architectural distortion, stromal invasion pattern, degree of desmoplastic reaction, and surrounding mesothelial reaction [5]. In the present case, the patient had an epithelioid mesothelioma with infiltrative features and no evidence of desmoplastic reaction or necrosis. The marked variation in the histopathologic appearance of mesothelioma can make it challenging to establish the diagnosis with confidence and differentiate it from secondary peritoneal carcinomatosis.
Immunohistochemical staining for mesothelial and epithelial markers should be routinely performed in all ascitic fluid cytology specimens, as it assists in establishing mesothelial lineage and establishing an accurate diagnosis of mesothelioma [5]. Establishment of mesothelial lineage is essential for differentiating secondary peritoneal carcinomatosis from primary peritoneal mesothelioma, as was the case in our patient. Moreover, loss of BAP1 expression and MTAP immunohistochemistry can help in differentiating between benign mesothelial proliferation and mesothelioma. In the present case, tumor cells were positive for AE1/3, CK5/6, CK7, calretinin, D2-40, and WT1, which was consistent with a mesothelial origin of neoplastic cells. Although BAP1 expression was retained in tumor cells, nuclear and cellular atypia, as well as infiltrative features on microscopy, were unequivocal for malignancy. Although not used in our case, cytogenetic analyses using fluorescent in situ hybridization techniques can provide valuable evidence in patients when the distinction between benign mesothelial proliferation and malignant neoplasia is challenging to make on microscopy alone [18,19].
Genomic alterations detected by next generation sequencing are evolving as important tools in the diagnosis, prognostication, and management of mesothelioma [20]. A study of mesothelioma based on next generation sequencing reported that peritoneal mesotheliomas harbor microsatellite instability in 47% of cases and mutations in BAP1, CDKN2A/B, NF2, and ATM genes in 32%, 16%, 16%, and 11% of cases, respectively [21]. In another study, a 48-gene signature was identified by Nair et al [22] using tumor (somatic) and germline whole-exome sequencing that predicted survival of patients with peritoneal mesothelioma. In our patient, next generation sequencing technologies were not used given that the diagnosis was established by omental biopsy and cytology on the second ascitic fluid sample. In the future, genomics and radiomics will likely become an integral tool in the diagnosis and management of patients with peritoneal mesothelioma [5]. Such novel technologies can prevent delays in diagnosis, which were unfortunately the case in our patient.
TREATMENT AND PROGNOSTICATION:
The most well-studied treatment for peritoneal mesothelioma is a combination of cytoreductive surgery and HIPEC. In a recent study of 118 patients with peritoneal mesothelioma from 5 different cancer centers, the median overall survival of patients who underwent perioperative chemotherapy along with cytoreductive surgery and HPIEC was 67 months [23]. Moreover, the adequacy of cytoreductive surgery, as reflected by the completeness of cytoreduction score, was strongly associated with survival. In the same study, worse prognosis was noted for patients who were not candidates for cytoreductive surgery with HIPEC, with a median overall survival of 12.6 months. Within this group of patients, poor performance status (hazard ratio: 5.3) and presence of ascites (hazard ratio: 6.0) were strong predictors of mortality. Additionally, recent case reports have demonstrated the feasibility of cytoreductive surgery combined with bidirectional chemotherapy using intraperitoneal cisplatin and intravenous ifosfamide among patients with peritoneal mesothelioma who had pre-existing renal impairment [10,11]. In our case, the patient had a poor pre-treatment performance status and opted for hospice care, in line with his preferences and personal values for spending time with his family at home, making him ineligible for cytoreductive surgery and HIPEC.
Conclusions
Peritoneal mesothelioma is a rare malignancy that is strongly associated with asbestos exposure and most frequently presents with vague constitutional symptoms. In patients with a history of asbestos exposure and suggestive symptoms, the diagnosis of mesothelioma should always be kept in mind, especially since the diagnosis is challenging to make. The present case also highlights the importance of considering the limited yield (approximately 50%) of ascitic fluid cytology and the need for omental biopsy (if needed) for making a diagnosis. In patients with loculated ascites with a SAAG <1.1 g/dL who have a negative peritoneal fluid cytology and no obvious omental caking, diagnostic laparoscopy is the most logical next step. As demonstrated by this case, in patients in which the first set of ascitic fluid studies are inconclusive, repeat abdominal paracentesis with omental biopsy or diagnostic laparoscopy should be expedited to avoid delays in diagnosis. Future research should focus on the role of ascitic fluid genomics, proteomics, and radiomics analyses in differentiating between peritoneal mesothelioma and peritoneal tuberculosis. Such novel investigations can help to improve the diagnostic accuracy of ascitic fluid analysis and. potentially, obviate the need for invasive biopsy procedures in selected patients.
Figures
References:
1.. Patel YA, Muir AJ, Evaluation of new-onset ascites: JAMA, 2016; 316; 340-41
2.. Du L, Wei N, Maiwall R, Song Y, Differential diagnosis of ascites: Etiologies, ascitic fluid analysis, diagnostic algorithm: Clin Chem Lab Med, 2024; 62; 1266-76
3.. Runyon BA, Montano AA, Akriviadis EA, The serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites: Ann Intern Med, 1992; 117; 215-20
4.. Ikegami T, Ishiki H, Kadono T, Narrative review of malignant ascites: Epidemiology, pathophysiology, assessment, and treatment: Ann Palliat Med, 2024; 13; 842-57
5.. Husain AN, Chapel DB, Attanoos R, Guidelines for pathologic diagnosis of mesothelioma: 2023 update of the consensus statement from the International Mesothelioma Interest Group: Arch Pathol Lab Med, 2024; 148; 1251-71
6.. Chen Z, Cai Y, Ou T, Global burden of mesothelioma attributable to occupational asbestos exposure in 204 countries and territories: 1990–2019: J Cancer Res Clin Oncol., 2024; 150; 282
7.. Michael CW, The cytologic diagnosis of mesothelioma: Are we there yet?: J Am Soc Cytopathol, 2023; 12; 89-104
8.. Khan S, Malik A, Qureshi S, Incidental diagnosis of malignant peritoneal mesothelioma during liver transplantation surgery: A case report: Am J Case Rep, 2024; 25; e943787
9.. Altshuler PC, Newman AL, Garibay JA, Rapid progression of malignant peritoneal mesothelioma mimicking a postoperative complication in a young woman: A case report: Am J Case Rep, 2024; 25; e942948
10.. Alaswad M, ElKordy F, Jaamour H, A 51-year-old woman with advanced peritoneal mesothelioma and stage 3b chronic kidney disease treated with cytoreductive surgery and bidirectional intraperitoneal cisplatin and ifosfamide chemotherapy: A case report: Am J Case Rep, 2023; 24; e941726
11.. Almesned R, Azzam AZ, Aldeheshi A, Amin TM, Bidirectional intraoperative chemotherapy using cisplatin and ifosfamide for intraperitoneal mesothelioma in severe renal impairment: A case report: Am J Case Rep, 2023; 24; e938192
12.. Symes E, Tjota M, Cody B, Mesothelioma in situ of the peritoneum: Report of three cases and review of the literature: Histopathology, 2024; 84; 492-506
13.. Marchevsky AM, Khoor A, Walts AE, Localized malignant mesothelioma, an unusual and poorly characterized neoplasm of serosal origin: Best current evidence from the literature and the International Mesothelioma Panel: Mod Pathol, 2020; 33; 281-96
14.. Mahajan M, Prasad ML, Kumar P, An updated systematic review and meta-analysis for the diagnostic test accuracy of ascitic fluid adenosine deaminase in tuberculous peritonitis: Infect Chemother, 2023; 55; 264-77
15.. Awais M, Khan N, Khan AK, Rehman A, CT texture analysis for differentiating between peritoneal carcinomatosis and peritoneal tuberculosis: A cross-sectional study: Abdom Radiol (NY), 2024; 49; 857-67
16.. Frontario SC, Loveitt A, Goldenberg-Sandau A, Primary peritoneal mesothelioma resulting in small bowel obstruction: A case report and review of literature: Am J Case Rep, 2015; 16; 496-500
17.. Tentes AA, Zorbas G, Pallas N, Fiska A, Multicystic peritoneal mesothelioma: Am J Case Rep, 2012; 13; 262-64
18.. Girolami I, Lucenteforte E, Eccher A, Evidence-based diagnostic performance of novel biomarkers for the diagnosis of malignant mesothelioma in effusion cytology: Cancer Cytopathol, 2022; 130; 96-109
19.. Sa-Ngiamwibool P, Hamasaki M, Kinoshita Y, Usefulness of NF2 hemizygous loss detected by fluorescence in situ hybridization in diagnosing pleural mesothelioma in tissue and cytology material: A multi-institutional study: Lung Cancer, 2023; 175; 27-35
20.. Febres-Aldana CA, Fanaroff R, Offin M, Diffuse pleural mesothelioma: Advances in molecular pathogenesis, diagnosis, and treatment: Annu Rev Pathol, 2024; 19; 11-42
21.. van Kooten JP, Dietz MV, Dubbink HJ, Genomic characterization and detection of potential therapeutic targets for peritoneal mesothelioma in current practice: Clin Exp Med, 2024; 24; 80
22.. Nair NU, Jiang Q, Wei JS, Genomic and transcriptomic analyses identify a prognostic gene signature and predict response to therapy in pleural and peritoneal mesothelioma: Cell Rep Med, 2023; 4; 100938
23.. Yasar S, Yilmaz F, Utkan G, Analysis of treatment strategies and outcomes in malignant peritoneal mesothelioma: Insights from a multi-center study: Ann Surg Oncol, 2024; 31; 6228-36
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133