30 June 2025: Articles 
Incidental Pelvic Ectopic Kidney Discovery During Pre-TAVR Imaging: Implications for Surgical Planning
Congenital defects / diseases
Prem Patel ACDEF 1*, Irina Radu CDE 2, Nikolaos KakourosDOI: 10.12659/AJCR.947068
Am J Case Rep 2025; 26:e947068






Abstract
BACKGROUND: Renal ectopia (RE) is a congenital malformation in which one or both kidneys fail to reach their normal anatomical position. Most cases are asymptomatic, but they can occasionally lead to complications. This case report presents the incidental finding of a pelvic ectopic kidney during a pre-transcatheter aortic valve replacement (TAVR) evaluation, showing the importance of recognizing anatomical variations in surgical planning for vascular access.
CASE REPORT: A 68-year-old man undergoing evaluation for severe symptomatic aortic stenosis was incidentally found to have a left pelvic kidney on computed tomography (CT) angiography. The CT scan revealed a dual arterial supply, with one artery entering the kidney medially and an accessory artery wrapping laterally around the kidney, which may have contributed to the failure of its ascent during embryological development. He had no urinary symptoms, and renal function was normal, so no further intervention was required. The identification of this vascular anomaly emphasizes the need for proper preoperative imaging to avoid complications.
CONCLUSIONS: Recognizing anatomical variations like renal ectopia can help optimize complex vascular procedure planning and prevent complications. Additionally, this case highlights the association between multiple renal arteries and renal ectopia, suggesting further research is needed to understand these correlations.
Keywords: Congenital Abnormalities, Transcatheter Aortic Valve Replacement, Renal Circulation, Renal Artery, Humans, Male, Aged, Incidental Findings, kidney, computed tomography angiography, Aortic Valve Stenosis
Introduction
Renal ectopia (RE) is a congenital abnormality in which one or both kidneys are located outside their usual anatomic location in the renal fossa. This malformation typically occurs due to disruption of the kidney’s normal ascent during the embryological development. Kidneys normally start their ascent from the sacral level, completing it near the first lumbar vertebra [1]. Typically, kidneys are located retroperitoneally, flanking the spine and bordered by muscles such as the diaphragm, psoas major, and quadratus lumborum. In cases of renal ectopia, the kidneys may be found in the pelvic region, lower abdomen, or even on the opposite side of the body (crossed renal ectopia) [2–5]. Left-sided pelvic renal ectopic is the most common form [6]. Although most cases are asymptomatic and discovered incidentally during imaging, renal ectopia can occasionally lead to complications such as urinary obstruction, infection, or stone formation [7]. In this report, we present a case of an incidental pelvic ectopic kidney discovered during pre-transcatheter aortic valve replacement (TAVR) evaluation.
Case Report
A 68-year-old man with severe symptomatic aortic stenosis, mild non-obstructive coronary artery disease, hypertension, hyperlipidemia, type 2 diabetes mellitus, and obesity (body mass index 41 kg/m2) was referred for TAVR evaluation. Vital signs included blood pressure 131/70 mmHg, heart rate 95 beats per minute, and oxygen saturation 92% on room air. His cardiovascular physical examination revealed a grade III/VI late-peaking systolic murmur at the right upper sternal border, radiating throughout the precordium. The laboratory results were unremarkable – renal function was normal, with estimated GFR >90 mL/min/1.73 m2 by CKD-EPI equation. There was no family history of congenital kidney disease or valvular disease. He had a 30-pack-year history of smoking and did not drink alcohol.
As part of the TAVR work-up, a computed tomography (CT) angiography scan of the chest, abdomen, and pelvis was performed, which incidentally revealed a left pelvic kidney (Figure 1, Video 1). Additionally, the CT scan demonstrated a dual arterial supply to the left kidney, with one artery entering medially at the hilum and an accessory artery wrapping around the lateral side of the kidney. This accessory artery may have contributed to the kidney’s failure to ascent during development. In this case, the right common femoral access site selected for the large-bore delivery sheath. We were cognizant of the anomalous renal artery arising from the very proximal right common iliac (effectively at the aortic bifurcation) and ensured all wires were advanced under fluoroscopy. The TAVR was performed successfully and without complications. Given the absence of symptoms and normal renal function, no further intervention was deemed necessary, and routine follow-up was advised.
Discussion
Renal ascent during embryonic development is a complex and not fully understood process. The reported incidence of renal ectopia varies with the diagnostic modality, ultrasound studies reporting an incidence of approximately 1/900 [8]. While most patients with renal ectopia are asymptomatic, some develop symptoms such as flank pain, hematuria, or recurrent urinary tract infections if complications arise. Symptomatic presentations are more common in children due to the increased risk of urinary stasis and infection. Diagnosis is typically made via imaging studies, including abdominal ultrasound, CT, or magnetic resonance imaging (MRI). In this case, the ectopic kidney was discovered incidentally during a pre-TAVR CT angiography. The incidence of symptomatic versus asymptomatic RE has not been well-studied, although one study reported hydronephrosis in 56% of patients with RE [9].
During early embryonic development, the kidneys are positioned in the pelvis with their hila oriented anteriorly. By the fourth week, the kidneys migrate upward, diverge, and rotate medially, with the hila ultimately facing anteromedially [10]. One driving force underlying this ascent is the straightening of the body, which involves the rapid longitudinal growth of the lumbosacral vertebrae and a reduction of the flexion at the lumbar level [1]. Although the mechanism underlying the failure of renal ascent remains unclear, factors such as vascular anomalies, genetic mutations, or physical obstructions (eg, abnormal spinal curvature) are thought to play a role. In our case, the presence of a dual arterial supply, with an accessory artery encircling the kidney, may have acted as an anatomical physical barrier preventing its ascent. Some studies have suggested an association between multiple renal arteries and renal ectopia or other renal anomalies [11–13].
Although a pelvic kidney is often benign, its presence requires considerations for surgical and interventional planning. Altered anatomy can complicate catheter navigation, vascular access, or other intraoperative maneuvers. The incidental finding of a pelvic kidney during a pre-TAVR evaluation is critical. During TAVR, it is routine to obtain bilateral femoral artery access and advance hydrophilic and stiff wires up the aorta. Mapping the location of the kidney and – more importantly – the renal arteries is important to avoid complications such as renal parenchymal hematoma or renal artery injury by advancement of the wires. The presence of an ectopic kidney needs to be reported as a significant finding in radiology reports and interventionalists may need to consider its presence during vascular access.
Symptomatic cases of renal ectopia may require surgical intervention for complications such as nephrolithiasis or obstruction. Treatment options include open pyelolithotomy, laparoscopic-assisted percutaneous nephrolithotomy, robot-assisted laparoscopic pyelolithotomy, or shock-wave lithotripsy [14]. Regular follow-up with renal function monitoring and imaging is recommended, particularly in patients with associated anomalies such as ureteropelvic junction obstruction or vesicoureteral reflux.
Conclusions
Comprehensive imaging and a multidisciplinary team approach are crucial to optimize procedural planning and prevent complications in patients with anatomical variations undergoing complex procedures such as TAVR. Renal ectopia is likely underreported due to limited imaging in certain populations. Furthermore, the association between accessory renal arteries and renal ectopia is unclear. As imaging technologies advance, the detection of renal ectopia and its correlation with vascular anomalies is expected to increase.
Figures
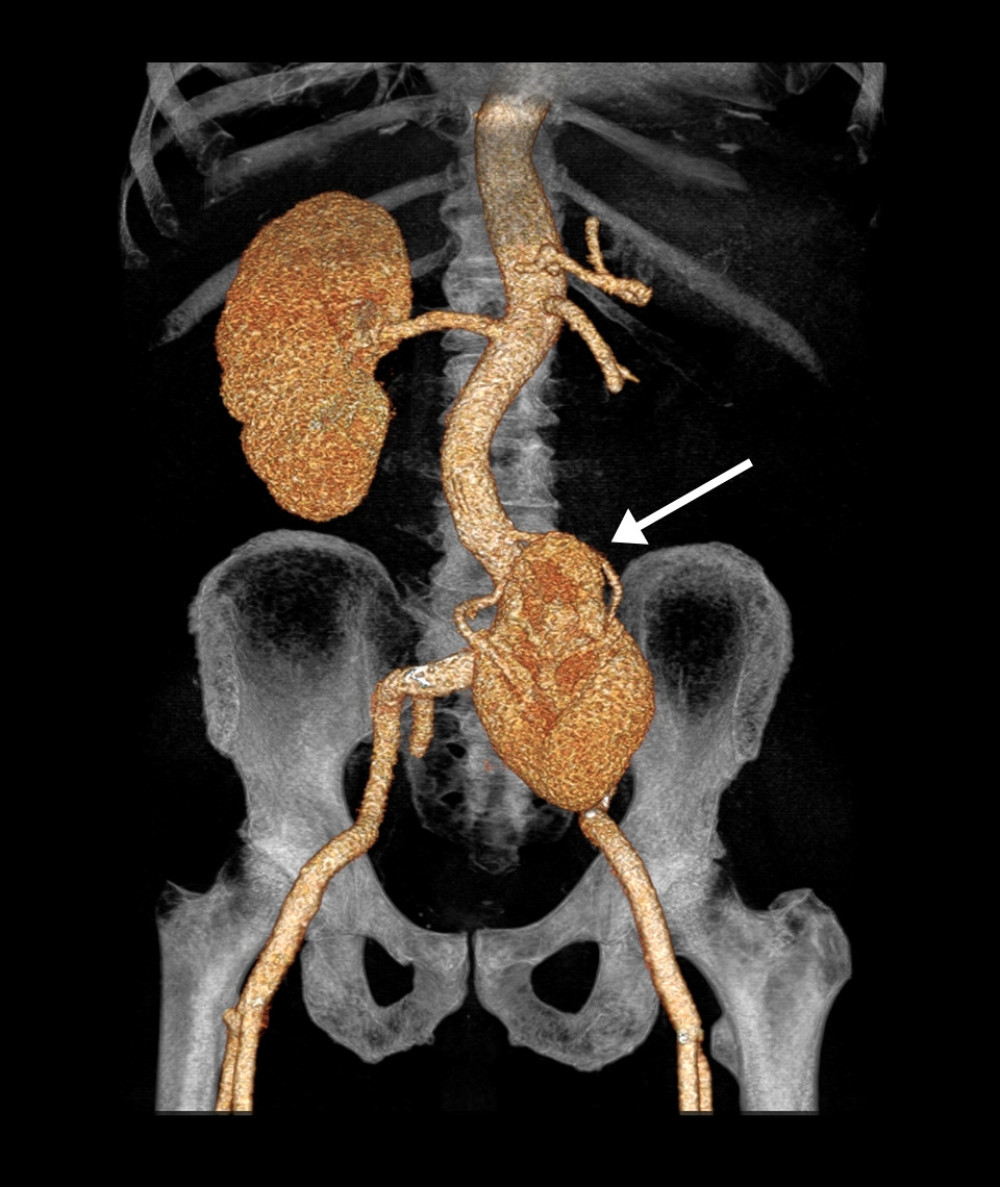 Figure 1. Three-dimensional reconstruction of the abdominal-pelvic region demonstrating pelvic ectopic kidney. The pelvic kidney is indicated by the white arrow.
Figure 1. Three-dimensional reconstruction of the abdominal-pelvic region demonstrating pelvic ectopic kidney. The pelvic kidney is indicated by the white arrow. 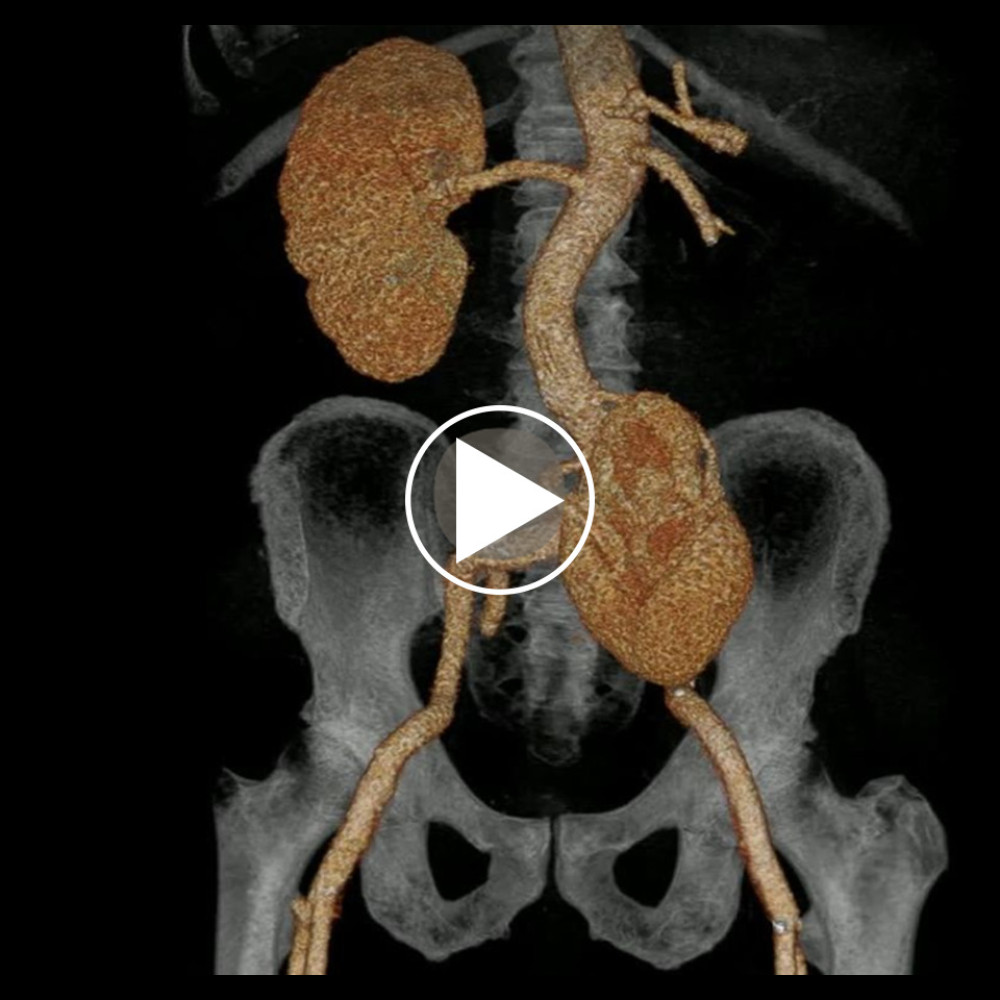 Video 1. Rotational video of three-dimensional CT reconstruction of the abdominal-pelvic region demonstrating pelvic ectopic kidney. The video displays the spatial and anatomic relationships of the ectopic kidney within the pelvic cavity.
Video 1. Rotational video of three-dimensional CT reconstruction of the abdominal-pelvic region demonstrating pelvic ectopic kidney. The video displays the spatial and anatomic relationships of the ectopic kidney within the pelvic cavity. References
1. Fukuoka K, Wilting J, Rodríguez-Vázquez JF, The embryonic ascent of the kidney revisited: Anat Rec, 2019; 302(2); 278-87
2. Bhattar R, Maheshwari A, Tomar V, Yadav SS, Crossed fused ectopic kidney: A case report: J Clin Diagn Res, 2017; 11(8); PD11-12
3. Iseko KI, Iseko JBR, Ewuzie OC, Akpan CI, Bilateral, fused pelvic, ectopic, laterally rotated kidneys: A case report: Radiol Case Rep, 2020; 15(7); 841-45
4. Mudoni A, Caccetta F, Caroppo M, Crossed fused renal ectopia: Case report and review of the literature: J Ultrasound, 2017; 20(4); 333-37
5. Prasad S, Thomas J, Crossed unfused renal ectopia: BMJ Case Rep, 2014; 2014; bcr-2013-202960
6. Alvarez JC, Guerra Mieles AJ, Rivera-Escalante C, Pelvic renal ectopia: Unusual position abnormality: Cureus, 2021; 13(4); e14365
7. Alfaseh A, Ilaiwy A, RCC in cross ectopic kidney: A challenging diagnosis and management: BMJ Case Rep, 2018; 2018; bcr-2018-226879
8. Ramanathan S, Kumar D, Khanna M, Multi-modality imaging review of congenital abnormalities of kidney and upper urinary tract: World J Radiol, 2016; 8(2); 132-41
9. Gleason PE, Kelalis PP, Husmann DA, Kramer SA, Hydronephrosis in renal ectopia: Incidence, etiology and significance: J Urol, 1994; 151(6); 1660-61
10. Shapiro E, Upper urinary tract anomalies and perinatal renal tumors: Clin Perinatol, 2014; 41(3); 679-94
11. Poudiougo AM, Touré T, Ba B, Case report: bilateral renal ectopy with bilateral accessory renal artery and renal pelvis variations: Transl Res Anat, 2023; 30; 100236
12. Zagyapan R, Pelin C, Kürkçüoğlu A, A retrospective study on multiple renal arteries in the Turkish population: Anat (Int J Exp Clin Anat), 2009; 3; 35-39
13. Zahoi DE, Miclaus G, Aurora A, Ectopic kidney with malrotation and multiple bilateral arteries diagnosed by CT angiography: Rom J Morphol Embryol, 2010; 51(3); 589-92
14. Patandung R, Prapiska FF, Kadar DD, Open pyelolithotomy in an ectopic kidney: A case report: Urol Case Rep, 2020; 35; 101528
Figures
Figure 1. Three-dimensional reconstruction of the abdominal-pelvic region demonstrating pelvic ectopic kidney. The pelvic kidney is indicated by the white arrow.Video 1. Rotational video of three-dimensional CT reconstruction of the abdominal-pelvic region demonstrating pelvic ectopic kidney. The video displays the spatial and anatomic relationships of the ectopic kidney within the pelvic cavity. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133