27 June 2025: Articles 
Combining Retroperitoneal Laparoscopic Ureterolithotomy and Flexible Ureteroscopy for Effective Removal of a Large Ureteral Stone: A Case Report
Unusual or unexpected effect of treatment
Ru-Nan Dong BEF 1, Kristine Joy Shan Joy Shan KwanDOI: 10.12659/AJCR.947262
Am J Case Rep 2025; 26:e947262






Abstract
BACKGROUND: Large ureteral stones (LUSs) pose significant health risks, including chronic obstruction and renal impairment. Timely intervention is critical to preserve kidney function. While the optimal treatment for LUS is debated, retroperitoneal laparoscopic ureterolithotomy (RLU) is often preferred over percutaneous nephrolithotomy (PCNL), ureteroscopy, or extracorporeal shockwave lithotripsy due to its effectiveness. Combining RLU with antegrade flexible ureteroscopy (aFURS) can enhance stone clearance rates, addressing the challenges of intrarenal access and guidewire passage.
CASE REPORT: We report the case of a 65-year-old woman with a large proximal left ureteral stone (15×15×42 mm), renal atrophy, and severe hydronephrosis, presenting with persistent lumbar pain and intermittent hematuria. An urgent percutaneous nephrostomy (PCN) improved her renal function, yet left renal GFR was low at 10.62 ml/min. Forty-seven days post-PCN, she underwent a combined procedure of RPLU and aFURS through the PCN tract. This approach ensured complete stone removal while minimizing ureteral trauma. The stone was successfully fragmented and removed, followed by antegrade double-J stenting. The patient experienced an uneventful recovery and was symptom-free at the 3-month follow-up. Imaging confirmed the absence of residual stones and strictures.
CONCLUSIONS: This case underscores the effectiveness and safety of combining RPLU and aFURS for large ureteral stone removal in a single session. It highlights the importance of a multidisciplinary approach and surgical expertise in managing complex stone cases, offering insights into optimizing patient outcomes and minimizing complications.
Keywords: Laparoscopy, Minimally Invasive Surgical Procedures, Ureteral Obstruction, ureterolithiasis, Ureteroscopy, Humans, Female, Aged, Ureteral Calculi, Retroperitoneal Space
Introduction
The reported mean diameter of ureteral stones ranges from 3.7 mm to 6.7 mm [1,2]. In most cases, ureteral stones smaller than ~5 mm pass spontaneously [3]. However, when the stone size exceeds approximately 11–22% of the ureter’s inner diameter, obstruction and associated complications may occur, rendering conservative treatment ineffective [4]. According to the 2024 European Association of Urology (EAU) guidelines, ureteroscopy (URS; antegrade or retrograde) and shockwave lithotripsy (SWL) are recommended for ureteral stones >10 mm [5]. However, the stone-free rate for SWL decreases significantly for stones >20 mm [6]. Increasing stone size and severe hydronephrosis can lead to stone impaction, making guidewire placement and flexible ureteroscopy (FURS) difficult or impossible [7]. Consequently, the optimal treatment for large ureteral stones (LUSs) remains a topic of debate. Retroperitoneal laparoscopic ureterolithotomy (RLU) is considered a feasible alternative when URS and SWL fail to remove LUS. However, RLU is associated with longer operative times, extended hospital stays, and higher complication rates [8]. Here, we present a successful case of RLU combined with antegrade flexible ureteroscopy (aFURS), performed through a previously established percutaneous nephrostomy (PCN) tract, to achieve complete LUS removal in a single procedure.
Case Report
A 65-year-old woman with a 6-month history of persistent left flank pain and intermittent hematuria was referred to our institute. Computed tomography (CT) identified an LUS as the underlying cause. Upon admission, her vital signs were stable. Contrast-enhanced CT revealed a left bullet-shaped LUS measuring approximately 50 mm in diameter (mean CT value: 1342.7 HU; max CT value: 1803.0 HU; Figure 1A, 1D) accompanied by ipsilateral renal atrophy and significant hydronephrosis. Biochemicals showed elevated creatinine levels (98 μmol/L).
Urgent PCN was performed for decompression. Under ultrasound guidance, a nephrostomy puncture was made through the 11th intercostal space into the middle calyx, and a 14-Fr nephrostomy tube was placed, yielding 70–90 mL of dark red fluid. The patient remained stable postoperatively and was discharged on the third day to recover renal function at home.
She was followed up 47 days after PCN. A repeat CT scan showed improvement in left hydronephrosis and revealed an insignificant stone in the right kidney (Figure 1B, 1E). 99mTc-DTPA renal dynamic imaging indicated significantly reduced perfusion of the left kidney, with a split renal function percentage of 18.02% (compared to 81.98% on the right) and a glomerular filtration rate of 10.62 mL/min (compared to 48.30 mL/min on the right; Figure 2). Due to the severity of the LUS burden, elective surgery was planned to achieve complete stone clearance using RLU combined with aFURS.
Under general anesthesia, the patient was initially placed in the supine position, and a 16-Fr Foley catheter was inserted. She was then carefully repositioned to the right lateral decubitus position. The PCN tube was trimmed and the area disinfected. A 10-mm trocar was inserted at the mid-axillary line above the iliac crest for the camera port, with working ports placed below the 12th rib at the posterior axillary line (10-mm trocar) and at the subcostal anterior axillary line (5-mm trocar).
Under laparoscopic guidance, the dilated left proximal ureter was identified (Figure 3). A grasper was used to clamp the ureter just above the impacted stone to prevent migration. A full-thickness ureteral incision approximately 3 cm in length was made over the stone. The stone (15×15×42 mm), which was firmly adhered to the mucosa, split into 2 pieces during removal.
To ensure complete stone clearance and assess for potential ureteral injury, a guidewire was introduced through the PCN tract, and a 16-Fr peel-away sheath was placed. The flexible ureteroscope was inserted, continuous fluid irrigation (approximately 60 ml/minute flow rate) was performed to ensure a clear visual field, and confirmed there were no residual stones on the ureter mucosa or significant ureteral injury. The flexible ureteroscope was withdrawn. A 5-Fr Marflow ureteral stent was then inserted, and a new 14-Fr nephrostomy tube was retained. The ureteral incision was closed in an interrupted manner using 4-0 Vicryl® sutures, and a 14-Fr drainage tube was placed. The total operative time was 165 minutes, with negligible blood loss.
The patient had an uneventful recovery. Her postoperative creatinine level improved to 73 μmol/L. The Foley catheter, drainage tube, and PCN tube were removed on the second, third, and fifth postoperative days, respectively, and she was discharged with oral antibiotics.
She returned to the outpatient clinic 1 month postoperatively for ureteral stent removal. A follow-up CT scan confirmed complete left stone clearance, and the intact stent was retrieved without complications (Figure 1C, 1F). At her 3-month follow-up, she remained asymptomatic, and ultrasound evaluation confirmed no evidence of ureteric stricture.
Discussion
The management of large ureteral stones (LUS) in this patient posed significant challenges, including compromised renal function, hydronephrosis, stone impaction with strong adherence to the ureteral mucosa, and the risk of iatrogenic ureteric stricture. Due to the stone burden, a retrograde approach for ureteral stent placement was not feasible; therefore, percutaneous nephrostomy (PCN) was performed to provide urgent decompression of the obstructed collecting system. The small volume of dark red drainage fluid was likely due to the release of retained blood. Her creatinine levels and urine output were closely monitored in the outpatient setting, and preoperative evaluation of the left kidney was conducted radiographically before proceeding to stone removal.
The ideal stone management procedure should achieve a high stone clearance rate, be completed in a single session, and remain minimally invasive. Flexible ureteroscopy (FURS) is increasingly utilized as a first-line treatment for urolithiasis; however, reported stone-free rates show significant variability, ranging from 52.2% to 90.2% in real-world data [8,9]. In contrast, shockwave lithotripsy (SWL) often requires multiple sessions (an average of 1.5 sessions) depending on factors such as stone size and patient age [10]. The stone-free rate for SWL after a single session can be as low as 46.7% for ureteral stones but may increase to 90.0% after 3 sessions [11]. Comparatively, studies indicate that FURS achieves significantly higher stone-free rates than SWL, with rates of 89.5% versus 72.7%, respectively (
RLU combined with aFURS proved to be a safe and effective approach for managing LUS in a single session, with no complications. Advancements in endourological techniques, such as URS and percutaneous nephrolithotomy, have significantly reduced the need for open or laparoscopic stone surgeries. However, the role of RLU for LUS removal remains underexplored, despite studies reporting a >95% treatment success rate [13]. Notably, the EAU guidelines recommend RLU in cases where surgical expertise is available, emphasizing the importance of surgeon proficiency in endourological instrumentation and laparoscopic techniques.
Previous studies have described the combined use of RLU and retrograde FURS for removing residual ureteropelvic junction stones alongside multiple renal stones, with the scope introduced through a third working port for ureterostomy [14]. In this case, introducing the scope through the existing PCN tract provided greater accuracy in access and potentially minimized the risk of injury to nearby organs.
The challenges of stone impaction and adherence to the ureteral mucosa made extraction difficult. While preoperative CT imaging provided essential diagnostic details such as stone size and location, intraoperative evaluation through RLU and FURS enabled a comprehensive assessment of the ureter’s inner and outer condition. This approach avoided the need for open surgery and minimized the risk of iatrogenic complications, including ureteral perforation, stricture, or leakage [15]. While barbed sutures secured with Hem-o-locks are used during partial nephrectomy to avoid knot tying and speed the suture placement, we advise against using this for closing the ureter as it can inadvertently irritate the ureter [16]. Additional measures, such as avoiding clamping of the ureteral wall, using non-electrosurgical tools for incisions, and performing longitudinal ureteral incisions closed with transverse suturing techniques (similar to the Heineke-Mikulicz technique), were employed to reduce the risk of ureteral stricture formation. Other specialized visualization techniques, such as intra-ureteral injection of indocyanine green and visualization under near-infrared fluorescence or narrow-band imaging could also provide better visualization of the ureteral stricture [17,18]. However, given that the surgical team was more proficient at endourological stone removal, these techniques were not applied. At the 3-month follow-up, the patient remained asymptomatic, and no postoperative complications were observed.
In summary, the early establishment of a PCN tract created favorable conditions for the subsequent combined procedure by allowing additional irrigation and surveillance, which facilitated enhanced stone clearance and surgical success. However, the positive outcome was also largely attributed to the surgeon’s proficiency in laparoscopic techniques, which minimized ureteral injury. While RLU and FURS are efficient, the ultimate success of such procedures depends on the surgeon’s extensive experience and expertise.
Conclusions
RLU combined with aFURS offers a viable treatment option for LUS when conventional approaches such as URS and SWL are not feasible. This case reinforces the need for a multidisciplinary approach and surgical proficiency to achieve optimal outcomes in patients with challenging stone burdens.
Figures
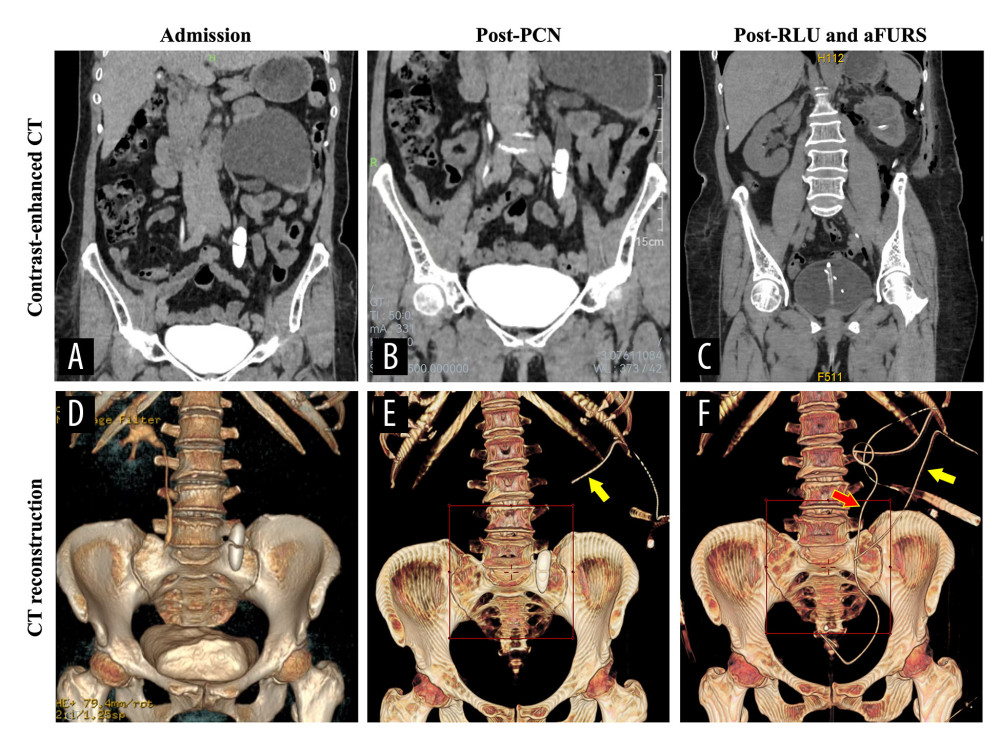 Figure 1. Contrast-enhanced computed tomography scans of the patient (A) upon admission, (B) 1 month after percutaneous nephrostomy, and (C) 5 days after retroperitoneal laparoscopic ureterolithotomy and antegrade flexible ureteroscopy. Reconstructed computed tomography images (D) upon admission, (E) 1 month after percutaneous nephrostomy where the tube (yellow arrow) is visible, and (F) 5 days after retroperitoneal laparoscopic ureterolithotomy and antegrade flexible ureteroscopy prior removal of the nephrostomy tube (yellow arrow) and an intact ureteral stent (red arrow).
Figure 1. Contrast-enhanced computed tomography scans of the patient (A) upon admission, (B) 1 month after percutaneous nephrostomy, and (C) 5 days after retroperitoneal laparoscopic ureterolithotomy and antegrade flexible ureteroscopy. Reconstructed computed tomography images (D) upon admission, (E) 1 month after percutaneous nephrostomy where the tube (yellow arrow) is visible, and (F) 5 days after retroperitoneal laparoscopic ureterolithotomy and antegrade flexible ureteroscopy prior removal of the nephrostomy tube (yellow arrow) and an intact ureteral stent (red arrow). 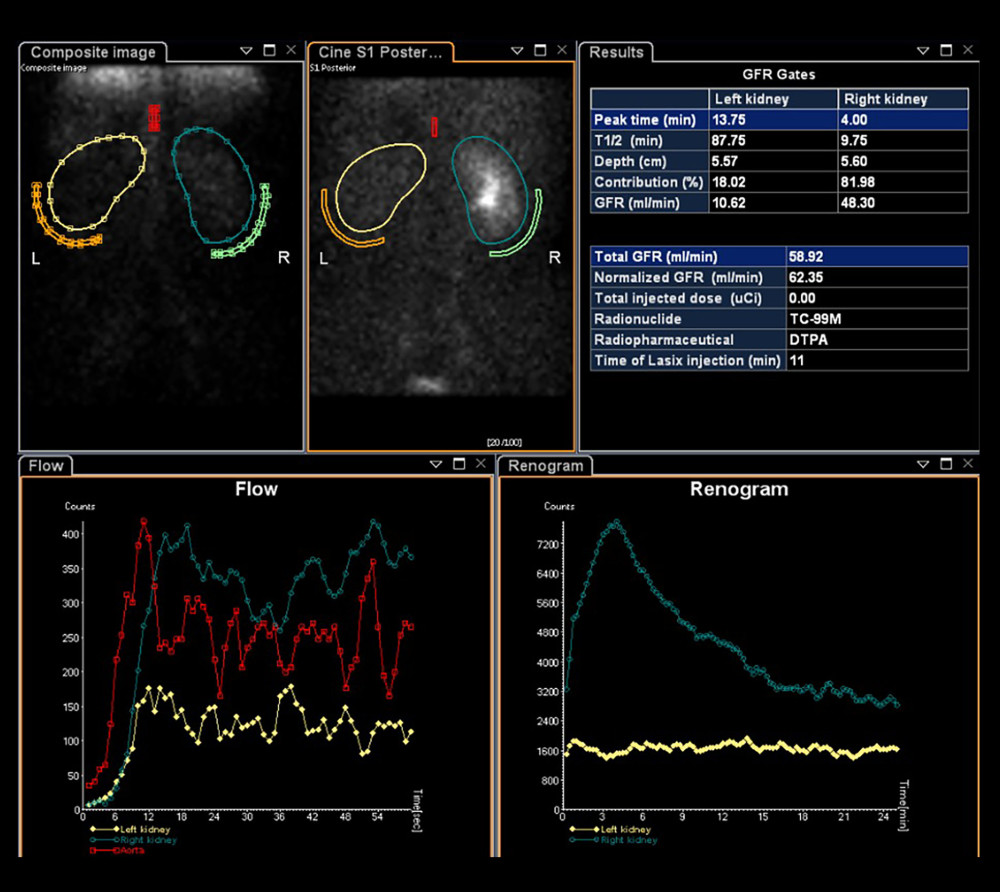 Figure 2. 99mTc-DTPA renal dynamic imaging results showing the split renal function of the patient’s kidneys.
Figure 2. 99mTc-DTPA renal dynamic imaging results showing the split renal function of the patient’s kidneys.  Figure 3. The operative setup showing the flexible ureteroscopy screen (B) and laparoscopic image (A) when the large ureteral stone is identified. The extracted bullet-shaped stone (square) measured 4.2×1.5×1.5 cm but split in half intraoperatively.
Figure 3. The operative setup showing the flexible ureteroscopy screen (B) and laparoscopic image (A) when the large ureteral stone is identified. The extracted bullet-shaped stone (square) measured 4.2×1.5×1.5 cm but split in half intraoperatively. References
1. Jendeberg J, Geijer H, Alshamari M, Size matters: The width and location of a ureteral stone accurately predict the chance of spontaneous passage: Eur Radiol, 2017; 27(11); 4775-85
2. Soomro HU, Hammad Ather M, Salam B, Comparison of ureteric stone size, on bone window versus standard soft-tissue window settings, on multi-detector non-contrast computed tomography: Arab J Urol, 2016; 14(3); 198-202
3. Song HJ, Cho ST, Kim KK, Investigation of the location of the ureteral stone and diameter of the ureter in patients with renal colic: Korean J Urol, 2010; 51(3); 198-201
4. Liu Y, Li M, Qiang L, Critical size of kidney stone through ureter: A mechanical analysis: J Mech Behav Biomed Mater, 2022; 135; 105432
5. , EAU Guidelines. Edn
6. Khan M, Lal M, Par Kash D, Anatomical factors predicting lower calyceal stone clearance after extracorporeal shockwave lithotripsy: Afr J Urol, 2016; 22(2); 96-100
7. Yamashita S, Inoue T, Kohjimoto Y, Hara I, Comprehensive endoscopic management of impacted ureteral stones: Literature review and expert opinions: Int J Urol, 2022; 29(8); 799-806
8. Ghani KR, Wolf JS, What is the stone-free rate following flexible ureteroscopy for kidney stones?: Nat Rev Urol, 2015; 12(5); 281-88 [published correction appears in Nat Rev Urol. 2015;12(7):363]
9. Kim HJ, Daignault-Newton S, DiBianco JM, Real-world practice stone-free rates after ureteroscopy: Variation and outcomes in a surgical collaborative: Eur Urol Focus, 2023; 9(5); 773-80
10. Wagenius M, Oddason K, Utter M, Factors influencing stone-free rate of Extracorporeal Shock Wave Lithotripsy (ESWL); A cohort study: Scand J Urol, 2022; 56(3); 237-43
11. Yoon JH, Park S, Kim SC, Outcomes of extracorporeal shock wave lithotripsy for ureteral stones according to ESWL intensity: Transl Androl Urol, 2021; 10(4); 1588-95
12. Kezer C, Comparison of shock wave lithotripsy and flexible ureterorenoscopy in the treatment of 10–20 mm lower pole stone: prospective non-randomized study: Cureus, 2022; 14(12); e32452
13. Şahin S, Aras B, Ekşi M, Şener NC, Tugču; V, Laparoscopic ureterolithotomy: JSLS, 2016; 20(1); e2016.00004
14. Chou SF, Hsieh PF, Lin WC, Huang CP, Laparoscopic ureterolithotomy and retrograde flexible ureteroscopy-assisted transperitoneal laparoscopic ureteroureterostomy for a huge ureteropelvic junction stone and multiple small renal stones: A CARE-compliant case report: Medicine (Baltimore), 2021; 100(28); e26655
15. Burks FN, Santucci RA, Management of iatrogenic ureteral injury: Ther Adv Urol, 2014; 6(3); 115-24
16. Lin Y, Liao B, Lai S, The application of barbed suture during the partial nephrectomy may modify perioperative results: A systematic review and meta-analysis: BMC Urol, 2019; 19(1); 5
17. Zhu W, Xiong S, Wu Y, Indocyanine green fluorescence imaging for laparoscopic complex upper urinary tract reconstructions: A comparative study: Transl Androl Urol, 2021; 10(3); 1071-79
18. Hao YC, Xiao CL, Liu KApplication of narrow-band imaging flexible ureteroscopy in the diagnosis, treatment and follow-up of upper tract urothelial carcinomas: Zhonghua Wai Ke Za Zhi, 2018; 56(3); 222-26 [in Chinese]
Figures
Figure 1. Contrast-enhanced computed tomography scans of the patient (A) upon admission, (B) 1 month after percutaneous nephrostomy, and (C) 5 days after retroperitoneal laparoscopic ureterolithotomy and antegrade flexible ureteroscopy. Reconstructed computed tomography images (D) upon admission, (E) 1 month after percutaneous nephrostomy where the tube (yellow arrow) is visible, and (F) 5 days after retroperitoneal laparoscopic ureterolithotomy and antegrade flexible ureteroscopy prior removal of the nephrostomy tube (yellow arrow) and an intact ureteral stent (red arrow).Figure 2. 99mTc-DTPA renal dynamic imaging results showing the split renal function of the patient’s kidneys.Figure 3. The operative setup showing the flexible ureteroscopy screen (B) and laparoscopic image (A) when the large ureteral stone is identified. The extracted bullet-shaped stone (square) measured 4.2×1.5×1.5 cm but split in half intraoperatively. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133