25 June 2025: Articles 
Colorectal Cancer with Ovarian Metastasis After Panitumumab and FOLFOX4: A Case Report
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents, Unexpected drug reaction
Agnieszka KoperDOI: 10.12659/AJCR.947300
Am J Case Rep 2025; 26:e947300






Abstract
BACKGROUND: Colorectal cancer is now one of the most common malignancies worldwide. Systemic treatment options for metastatic colorectal cancer (mCRC) are unsatisfactory, and the disease recurs despite the use of multiple drug combinations. Patients with mCRC and left-sided KRAS/NRAS/BRAF wild-type tumors may benefit from epidermal growth factor receptor (EGFR) inhibitors such as cetuximab or panitumumab in combination with chemotherapy. This report describes the case of a 67-year-old woman with advanced wild-type (WT) KRAS sigmoid colon adenocarcinoma in remission following treatment with panitumumab-FOLFOX4, presenting with ovarian metastases.
CASE REPORT: We present the case of a 67-year-old woman who was diagnosed with sigmoid colon cancer with metastasis to the periaortic lymph nodes. Due to the wild-type tumor subtype, targeted treatment with panitumumab and FOLFOX4 chemotherapy was implemented. Upon the third follow-up evaluating the effectiveness of therapy, complete remission (CR) was confirmed. During a routine follow-up at the gynecologist, a gynecologic ultrasound performed showed a questionable left adnexal mass, suspicious for primary ovarian cancer. Histopathological examination revealed metastatic adenocarcinoma of the colon. Imaging studies confirmed significant cancer progression. The chemotherapy regimen was changed to FOLFIRI. Imaging studies evaluating the effectiveness of therapy were performed every 3 months, confirming disease stabilization. The patient is still alive and continues to receive systemic therapy.
CONCLUSIONS: This case report supports previous studies, reports, and clinical trial data showing that treatment with panitumumab-FOLFOX4 can lead to a response in patients with advanced colonic adenocarcinoma and shows the importance of patient selection using molecular diagnostics, including KRAS mutation testing.
Keywords: Molecular Targeted Therapy, Neoplasms, Colorectal Neoplasms, Ovarian Neoplasms, Humans, Female, Aged, Antineoplastic Combined Chemotherapy Protocols, Panitumumab, leucovorin, Fluorouracil, Organoplatinum Compounds, Adenocarcinoma, Sigmoid Neoplasms
Introduction
Colorectal cancer (CRC) is one of the most common malignancies worldwide [1]. CRC is prone to distant metastasis to other sites, and the risk of recurrence is relatively high [1,2]. Systemic treatment options for mCRC are unsatisfactory, and the disease recurs despite the use of multiple drug combinations. Before starting treatment for mCRC, molecular diagnostics (to identify KRAS and NRAS gene exons and BRAF mutations) should be performed [1,3,4]. In metastatic disease, when radical surgical treatment is not possible, systemic therapy can improve survival rates. Patients with mCRC with left-sided KRAS/NRAS/BRAF wild-type tumors may benefit from EGFR inhibitors such as cetuximab or panitumumab in combination with chemotherapy [2,5]. This report describes a 67-year-old woman with advanced WT KRAS sigmoid colon adenocarcinoma in remission following treatment with panitumumab-FOLFOX4, presenting with ovarian metastases.
Case Report
A 67-year-old woman was referred to the Oncology Outpatient Clinic (23.09.2021) by her family doctor because of an abnormal finding on an abdominal ultrasound. The abnormalities included suspicious periaortic lymph nodes measuring up to 22 mm on the short axes. The patient had weight loss (3 kg in 2 months), night sweats, and abdominal pain. These symptoms prompted her to visit her primary care physician. During the visit to the Oncology Outpatient Clinic (23.09.2021), referrals were made for the following tests:
Genetic testing (FFPE Tissue DNA Kit, CatchGene FFPE Tissue DNA Kit, the center’s laboratory) (18.10.2021) found no mutations of the KRAS gene, NRAS gene, or BRAF gene in DNA isolated from tumor tissue. No MSI-H or d MMR was detected, and no HER2 overexpression was detected.
On 15.10.2021, at the meeting of the Interdisciplinary Team for Gastrointestinal Cancers, the case was considered unresectable, and the patient was qualified for palliative systemic treatment. On 19.10.2021, a vascular port was implanted for chemotherapy without complication. From 22.10.2021 to 16.08.2023, the patient received first-line treatment with panitumumab (6 mg/kg body weight) + FOLFOX4 in appropriate dosages. The patient was treated with this regimen for 22 months. After 12 cycles of chemotherapy according to the FOLFOX4 regimen with panitumumab, the dose of oxaliplatin was reduced to 65 mg/m2 due to symptoms of peripheral polyneuropathy (severity – grade 2 according to CTCAE). Of the complications during panitumumab treatment, a CTCAE grade 2 papulopustular rash was noted during the third cycle of systemic treatment, involving the face and trunk. Doxycycline 200 mg by mouth and intravenous hydrocortisone 1% were used, with good results.
During a routine check-up with her gynecologist at the Gynecology Outpatient Clinic (18.08.2023), a gynecological ultrasound was performed, identifying a questionable lesion in the left adnexal cast, suspicious for primary ovarian cancer. The patient was qualified for surgery. On 20.09.2023, a modified radical uterine excision was performed, and histopathological examination revealed a left ovarian metastatic adenocarcinoma of the colon.
On the first evaluation (CT, computed tomography) of treatment efficacy (14.01.2022), partial regression (PR) of the disease according to RECIST 1.1 was achieved. On the second evaluation (CT, 8.04.2022), PR of the disease was also noted. On the third evaluation (CT, 01.07.2022), complete remission (CR) was confirmed (Figure 3). CR was further confirmed on the fourth (CT, 16.12.2022), fifth (CT, 15.03.2023), and sixth evaluations (CT, 02.06.2023). On the seventh evaluation assessing the effectiveness of therapy (CT, 22.08.2023), disease progression was identified, showing a new pelvic lesion of about 120×85 mm (Figure 4). Treatment with panitumumab and chemotherapy according to the FOLFOX4 regimen was terminated.
From 30.10.2023 until 12.11.2024 (the time of the present study), the patient underwent chemotherapy according to the FOLFIRI regimen. No MSI-H/dMMR or HER2 overexpression was detected in our patient’s tumor. Therefore, checkpoint inhibitors and HER2-targeted therapies have not been and will not be considered in this patient. Since she received anti-EGFR + FOLFOX4 therapy as the first-line systemic palliative treatment, we used chemotherapy according to the FOLFIRI regimen as the second-line therapy.
To date, no clinically significant adverse effects have been reported. At each doctor’s visit, the patient was asked about possible complications such as diarrhea or vomiting. In imaging studies evaluating the effectiveness of therapy performed every 3 months, disease stabilization has been maintained. The patient is still alive and continues to receive systemic therapy.
Discussion
This is a rare case of ovarian metastasis from colon cancer. The case is interesting because during the treatment with panitumumab + FOLFOX4, the patient achieved complete remission in imaging tests.
CRC is one of the most common malignancies worldwide [1]. Approximately 20–25% of patients were found to have distant metastases at the time of diagnosis. The primary systemic treatment for CRC is fluoropyrimidines [3]. Systemic therapy for mCRC is based on a combination of fluorouracil with oxaliplatin or irinotecan. When the tumor has wild-type RAS genes, an epidermal growth factor inhibitor (eg, cetuximab or panitumumab) can improve the treatment of mCRC [4]. EGFR, also known as human EGRF 1 (HER1) or ErbB1, is a member of the ErbB family of receptor tyrosine kinases. Panitumumab is a fully human monoclonal antibody against EGFR that is currently administered as monotherapy or in combination with chemotherapy for the treatment of mCRC [5]. EGFR is widely expressed in healthy human skin tissues, including epidermal basal cells, hair follicle outer sheath cells, sebaceous glands, and vascular smooth muscle cells [6].
The role of targeted therapies in mCRC is enormous. Determination of tumor gene status for KRAS/NRAS and BRAF mutations, as well as HER2 amplifications and MSI/MMR status, are recommended for patients with mCRC. Testing may be carried out for individual genes or as part of an NGS (next-generation sequencing) panel, with NGS being preferred [7]. MSI-H or dMMR occurs in 3.5–5% of colorectal tumors [8]. In such patients, the use of checkpoint inhibitors should be considered [9]. HER2 is rarely amplified/overexpressed in CRC. While RAS/BRAF-wild-type mutations are more common in tumors, HER2-targeted therapies are now recommended as subsequent therapy options in patients with tumors that have HER2 overexpression [10]. No MSI-H/dMMR or HER2 overexpression was detected in our patient’s tumor. Therefore, checkpoint inhibitors and HER2-targeted therapies have not been and will not be considered in this patient. The patient had primary mCRC and did not have an MSI-H/dMMR assessment before adjuvant treatment.
All patients with mCRC should be tested for RAS mutations. Patients with unknown or mutant RAS status should not receive an EGFR antagonist, as it may be ineffective. Presence of a BRAF mutation has been identified as a marker potentially predictive of resistance to EGFR antagonists [5]. Patients with a right-sided tumor may not benefit from the addition of an EGFR antagonist to chemotherapy. Our patient was qualified for palliative de novo systemic treatment. The patient was disqualified from local treatment (surgery and radiotherapy). She was diagnosed with wild-type colon cancer, with a right-sided tumor. She was therefore qualified for therapy with an EGFR antagonist. A randomized phase III PRIME clinical trial included patients with stage IV colorectal cancer, with EGFR expression in tumor cells, demonstrated in an immunohistochemical study [11]. In the study group, patients were treated with panitumumab with FOLFOX4 chemotherapy. In the control group, patients were treated only with chemotherapy according to the FOLFOX4 program. In 60% of patients, normal functioning of the KRAS gene was found. In these patients, after adding panitumumab to cytotoxic therapy according to the FOLFOX4 regimen, compared to the group of patients receiving chemotherapy alone FOLFOX4, only a trend towards improved RR (55% vs 48%, respectively,
This case proved to be particularly complex, as we encountered several clinical and diagnostic problems. At first, the patient’s symptoms and the presence of enlarged periaortic lymph nodes could have indicated a diagnosis of lymphoma or other hematologic disease. Ultimately, minimally invasive diagnostic testing yielded a diagnosis of CRC.
The PRIME study reported a 57% objective response rate (ORR) in patients with wild-type CRC, with 1% of patients achieving CR [11]. In our patient, CR was first reported on imaging studies on 3 follow-up evaluations for treatment efficacy. Ovarian metastases of CRC are rare, so their diagnosis and treatment can be difficult [12]. The main diagnostic problem in our patient was the suspicion of a second, independent cancer. To verify the origin of this tumor, collection of material for histopathological examination was performed, confirming CRC ovarian metastasis.
For panitumumab, reported skin toxicities are similar to those reported for other EGFR inhibitors and include acne-like eruptions, papulopustular rashes, and pruritus [13]. Most patients (approximately 90%) treated with panitumumab develop skin reactions, a pharmacologic effect of epithelial growth factor receptor (EGFR) inhibitors. These reactions are generally classified as mild to moderate. If a patient develops a grade 3 skin reaction (on the NCI-CTC/CTCAE toxicity scale) or higher, or if the reaction is deemed intolerable, panitumumab should be temporarily discontinued until the skin reaction improves (≤ grade 2) [14,15]. In our patient, we noted a grade 2 papulopustular rash based on the CTCAE toxicity scale, involving the face and trunk area. Standard treatment (antibiotic therapy and symptomatic medications) was administered. One of the more commonly reported adverse effects during administration of FOLFOX4 chemotherapy is polyneuropathy [16]. Our patient also developed this complication. Hence, the dose of oxaliplatin was reduced.
Chemotherapy is the primary first-line therapy for advanced CRC in the absence of qualifying metastasectomy. The addition of biologic drugs reduces the risk of death compared to chemotherapy alone in patients with wild-type CRC. When determining the optimal treatment regimen, physicians should take into account the patient’s general condition, comorbidities, the target of therapy, the presence of RAS and BRAF mutations, and the presence of microsatellite instability [17]. CRC metastasis to the ovaries is rare. There are few publications on this subject. A study by Chen et al found that cytoreductive surgery (CRS) without macroscopic residual lesions plays an important role in treating mCRC of the ovaries [18]. Ovarian metastases occur in 3–5% of patients with colorectal cancer [19]. The role of oophorectomy in that setting continues to be debated. A study by Thornblade et al showed that patients benefit from removal of ovarian metastases. Our patient had the metastatic lesion removed during diagnostic and therapeutic surgery.
Conclusions
Modern molecularly targeted systemic therapies significantly prolong survival in patients with advanced CRC. Despite the advanced stage of CRC, few patients have achieved CR of the disease on imaging studies. If the existence of a second cancer is suspected during the course of oncologic therapy, one should always seek specimens for verification by histopathological examination. This case supports previous studies, reports, and clinical trial data showing that treatment with panitumumab-FOLFOX4 can lead to a response in patients with advanced colonic adenocarcinoma, and shows the importance of patient selection using molecular diagnostics, including KRAS mutation testing.
Figures
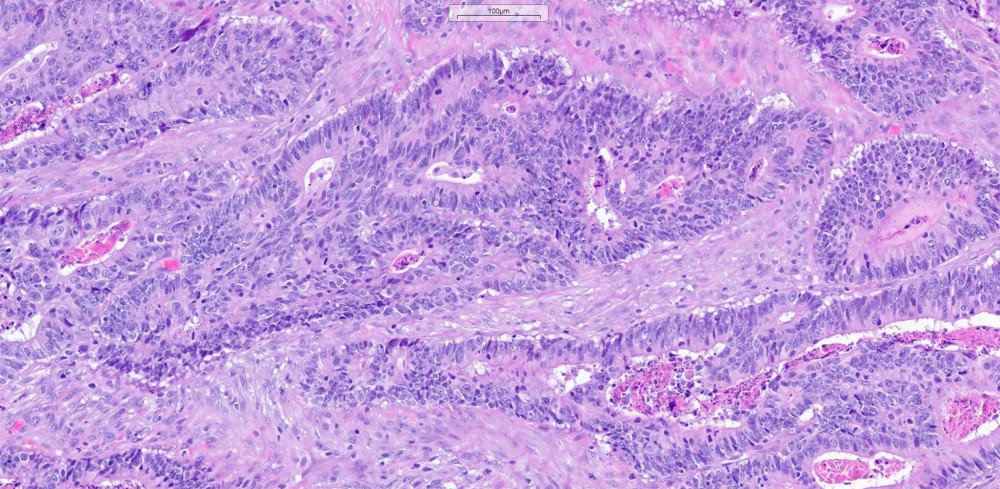 Figure 1. Histopathological picture of adenocarcinoma dated 30.09.2021.
Figure 1. Histopathological picture of adenocarcinoma dated 30.09.2021. 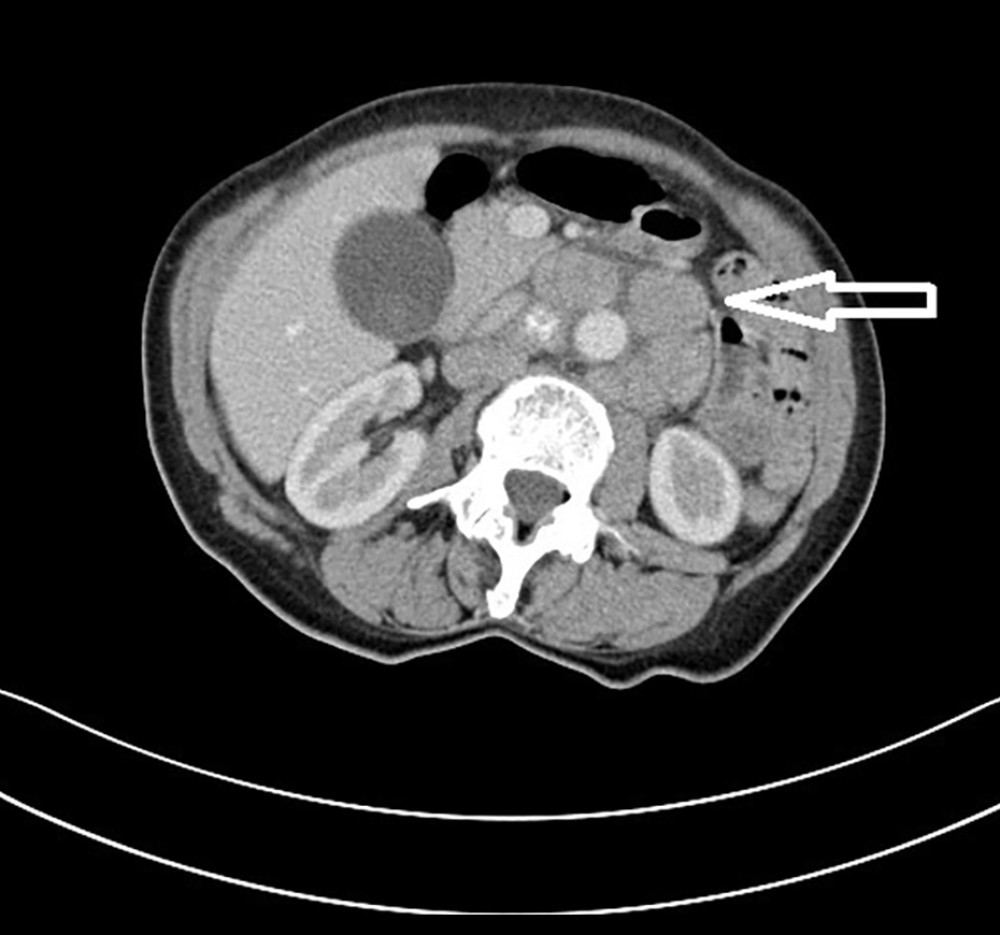 Figure 2. CT scan of the abdomen dated 01.10.2021 (enlarged periaortic lymph nodes with a dimension of 23 mm are marked with an arrow).
Figure 2. CT scan of the abdomen dated 01.10.2021 (enlarged periaortic lymph nodes with a dimension of 23 mm are marked with an arrow). 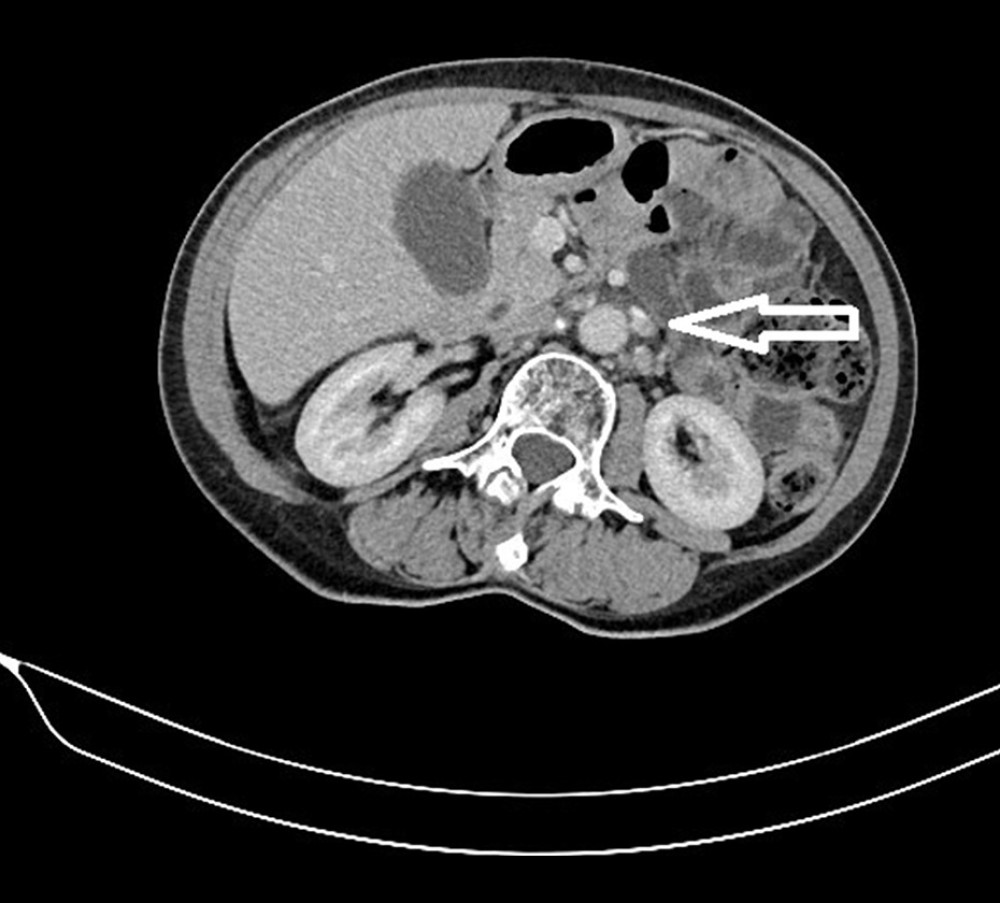 Figure 3. CT scan of the abdomen dated 01.07.2022 (periaortic lymph nodes with a dimension of 6 mm are marked with an arrow; complete remission was assessed according to RECIST 1.1).
Figure 3. CT scan of the abdomen dated 01.07.2022 (periaortic lymph nodes with a dimension of 6 mm are marked with an arrow; complete remission was assessed according to RECIST 1.1). 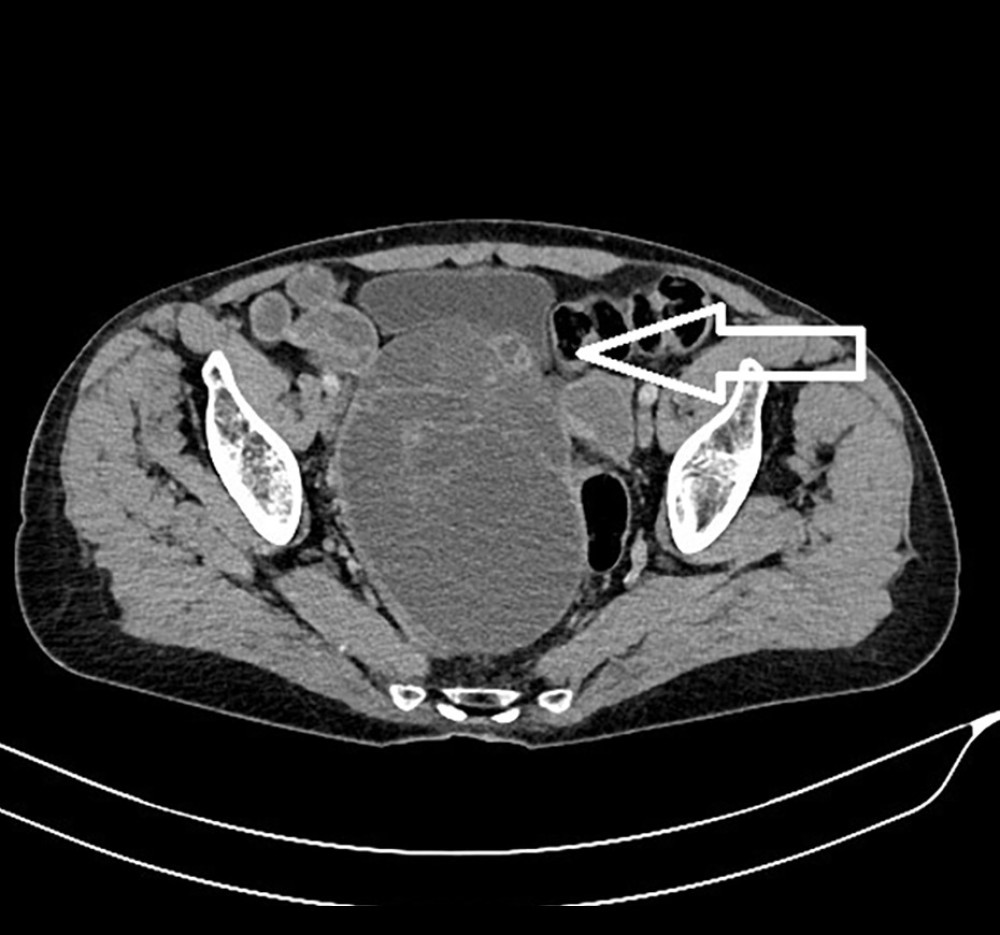 Figure 4. CT scan of the pelvis dated 22.08.2023 (arrow marks the tumor lesion in the pelvis).
Figure 4. CT scan of the pelvis dated 22.08.2023 (arrow marks the tumor lesion in the pelvis). References
1. Siegel RL, Miller KD, Jemal A, Cancer statistics, 2020: Cancer J Clin, 2020; 70(1); 7-30
2. Sakata S, Larson DW, Targeted therapy for colorectal cancer: Surg Oncol Clin N Am, 2022; 31(2); 255-64
3. Meyerhardt JA, Mayer RJ, Systemic therapy for colorectal cancer: N Engl J Med, 2005; 352(5); 476-87
4. Mayer RJ, Van Cutsem E, Falcone A, Randomized trial of TAS-102 for refractory metastatic colorectal cancer: N Engl J Med, 2015; 372(20); 1909-19
5. Battaglin F, Dadduzio V, Bergamo F, Anti-EGFR monoclonal antibody panitumumab for the treatment of patients with metastatic colorectal cancer: An overview of current practice and future perspectives: Expert Opin Biol Ther, 2017; 17(10); 1297-308
6. Li Y, Fu R, Jiang T, Mechanism of lethal skin toxicities induced by epidermal growth factor receptor inhibitors and related treatment strategies: Front Oncol, 2022; 12; 804212
7. Sonbol MB, Mountjoy LJ, Firwana B, The role of maintenance strategies in metastatic colorectal cancer: A systematic review and network meta-analysis of randomized clinical trials: JAMA Oncol, 2020; 6; e194489
8. Koopman M, Kortman GAM, Mekenkamp L, Deficient mismatch repair system in patients with sporadic advanced colorectal cancer: Br J Cancer, 2009; 100; 266-73
9. Topalian SL, Hodi FS, Brahmer JR, Safety, activity, and immune correlates of anti-PD-1 antibody in cancer: N Engl J Med, 2012; 366; 2443-54
10. Sartore-Bianchi A, Amatu A, Porcu L, HER2 Positivity predicts unresponsiveness to EGFR-targeted treatment in metastatic colorectal cancer: Oncologist, 2019; 24; 1395-402
11. Douillard JY, Siena SJ, Final results from PRIME: randomized phase III study of panitumumab with FOLFOX4 for first-line treatment of metastatic colorectal cancer: Ann Oncol, 2014; 25(7); 1346-55
12. Riihimäki M, Hemminiki A, Sudquist J, Patterns of metastasis in colon and rectal cancer: Sci Rep, 2016; 15; 29765
13. Mitchell EP, Piperdi B, Lacouture ME, The efficacy and safety of panitumumab administered concomitantly with FOLFIRI or irinotecan in second-line therapy for metastatic colorectal cancer: The secondary analysis from STEPP (Skin Toxicity Evaluation Protocol With Panitumumab) by KRAS status: Clin Colorectal Cancer, 2011; 10(4); 333-39
14. Hynes NE, Lane HA, ERBB receptors and cancer: The complexity of targeted inhibitors: Nat Rev Cancer, 2005; 5; 341-54
15. Segaert S, Tabernero J, Chosidow O, The management of skin reactions in cancer patients receiving epidermal growth factor receptor targeted therapies: J Dtsch Dermatol Ges, 2005; 3; 599-606
16. Cheng F, Zhang R, Sun Ch, Oxaliplatin-induced peripheral neurotoxicity in colorectal cancer patients: Mechanisms, pharmacokinetics and strategies: Front Pharmacol, 2023; 1; 14
17. Parseghian CM, Sun R, Woods M, Resistance mechanisms to anti-epidermal growth factor receptor therapy in RAS/RAF wild-type colorectal cancer vary by regimen and line of therapy: J Clin Oncol, 2023; 41(3); 460-71
18. Chen Z, Liu Z, Yang J, The clinicopathological characteristics, prognosis, and CT features of ovary metastasis from colorectal carcinoma: Transl Cancer Res, 2021; 10(7); 3248-58
19. Thornblade LW, Han E, Fong Y, Colorectal cancer ovarian metastases: Int J Gynecol Cancer, 2021; 31(8); 1137-44
Figures
Figure 1. Histopathological picture of adenocarcinoma dated 30.09.2021.Figure 2. CT scan of the abdomen dated 01.10.2021 (enlarged periaortic lymph nodes with a dimension of 23 mm are marked with an arrow).Figure 3. CT scan of the abdomen dated 01.07.2022 (periaortic lymph nodes with a dimension of 6 mm are marked with an arrow; complete remission was assessed according to RECIST 1.1).Figure 4. CT scan of the pelvis dated 22.08.2023 (arrow marks the tumor lesion in the pelvis). In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133