14 June 2025: Articles 
Management of Post-Kyphoplasty Cement Dislodgement in Osteoporotic Vertebral Fracture: A Case Report
Unusual clinical course, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents
Wennan Du ABCDEF 1, Zhiliang Guo ABCDG 1*DOI: 10.12659/AJCR.947316
Am J Case Rep 2025; 26:e947316






Abstract
BACKGROUND: Bone cement dislodgement (BCD) is a recognized complication of percutaneous vertebroplasty (PVP) that may be more common after percutaneous kyphoplasty (PKP). This report describes a 71-year-old woman with cement dislodgement following PKP of an osteoporotic T12 vertebral fracture successfully treated with repeat vertebroplasty(VP) through the right pedicle.
CASE REPORT: A 71-year-old woman underwent PKP surgery for T12 vertebral fracture caused by a fall. The pain disappeared after surgery, but 2 weeks later, she felt obvious pain again without any cause. Computed tomography (CT) showed BCD in T12 vertebra. Repeat PVP surgery was performed through the right pedicle, then the pain disappeared again. Six months later, the VAS score was 1 and the ODI score was 6.4%.
CONCLUSIONS: BCD is a complication of PKP that can occur without trauma. CT can definitively establish the diagnosis. Repeat VP is an effective treatment option for managing this condition, even when only the unilateral pedicle is accessible.
Keywords: Bone Cements, Osteoporotic Fractures, vertebroplasty, Humans, Female, Aged, Spinal Fractures, kyphoplasty, Thoracic Vertebrae, Reoperation, Tomography, X-Ray Computed
Introduction
Osteoporotic vertebral compression fractures (OVCF) are the most common fragility fractures [1]. PVP and PKP are 2 percutaneous interventional procedures used to treat symptomatic, nonhealing fragility fractures of the spine by injecting cement into the vertebral body, thereby providing structural support. PVP has a higher rate of cement extravasation than PKP. Therefore, PVP has been replaced with PKP as the main surgical procedure addressing OVCF [1]. Complications such as infections, bleeding, neurological dysfunction, and bone cement leakage occur in about 50% of patients who undergo vertebroplasty, but about 95% of them are clinically asymptomatic [1]. BCD is another complication after PKP and PVP, which can cause local pain, and even spinal deformity and neurological dysfunction [2]. BCD was first reported by Tsai [3] in 2003 and usually requires open surgery [2–4]. Some reports demonstrated minimally invasive surgery (MIS) can be a useful way to avoid open surgery [5,6]. This report describes a 71-year-old woman with BCD following PKP of T12 OVCF successfully treated with repeat VP.
Case Report
The patient was a 71-year-old woman with osteoporosis. She did not smoke, drink, or abuse drugs. She had undergone PKP twice for OVCF of L1 and L2 at her hometown hospital. This time, she underwent PKP surgery at another hospital for OVCF of the T12 caused by a fall. After the surgery, the pain was relieved; however, it recurred 2 weeks later without any cause. She experienced severe pain, which rendered her immobile and caused significant sleep disturbance. Fortunately, she had no neurological symptoms. Her back pain visual analog scale (VAS) score was 7, and the Oswestry Disability Index (ODI) score was 70%. CT showed the BCD in the T12 vertebra, with obvious cavities around the cement. The CT scan showed the cavities around the bone cement were interconnected. The cement mass obstructed the left pedicle, while the right pedicle had a passage leading to the cavity (Figure 1). The preoperative examination showed no contraindications, and repeat VP surgery was deemed appropriate following discussion with the patient.
During the surgical procedure, the patient received general anesthesia. After anesthesia, she was placed in prone position. G-arm fluoroscopy was used to locate and mark the surface projection of the right pedicle of the T12. Routine disinfection was performed with iodophor. A scalpel was used to incise the skin along the surface projection of the right pedicle of T12. Under fluoroscopy guidance, the needle was advanced to the posterior two-thirds of the inferior endplate, and its anterior position was adjusted to target the area not filled by the original bone cement along the right pedicle (Figure 2). During the puncture process, there was a slight sand-like obstruction sensation. After the puncture was made, the puncture needle core was pulled out. We prepared the bone cement twice in chronological order to make sure the cement was at the same stage when it was injected into the vertebra. Under G-arm fluoroscopy, about 3 ml of early-stage bone cement (Polymethyl Methacrylate, Heraeus) was injected into the vertebrae, and no cement leakage was observed.
The pain was relieved after this surgery. The postoperative CT scan showed the cavity was filled with bone cement (Figure 3). Six months after the surgery, the VAS was 1, and the ODI score was 6.4%.
Discussion
BCD is an uncommon complication after PKP and PVP, and PKP is an independent risk factor for BCD [7]. BCD can be treated by repeat VP. Zhang et al described 3 cases of BCD managed with repeat VP, in which working cannulas were placed at the superior and inferior margins of the cement mass, followed by bone cement injected during the late stage [6]. In their cases, the bone cement was injected into the vertebral body at a late stage, which is different from the early-stage injection we performed. The diffusion coefficient of high-viscosity bone cement is negatively correlated with the injection time, the leakage rate does not decrease with longer injection time, and high-viscosity bone cement should be injected as early as possible [8]. Yonezawa et al treated BCD patients with revision balloon kyphoplasty and vertebra-pediculoplasty using cannulated screws, allowing the cement to stabilize within the fractured vertebra, even under load stress, thus preventing secondary BCD [5]. A similar technique was applied in the treatment of Kummell disease to prevent BCD [9]. Our search of PubMed found no report of secondary BCD after repeat VP. It is unclear whether it is necessary to use screws and balloons, as reported by Yonezawa.
Yonezawa [5] and Zhang [6] performed bone cement injection by placing cannulas at the bilateral (left and right) sides and superior and inferior margins of the cement mass, which differs from the approach we used. Postoperative CT scans (Figure 3) demonstrated interconnected cavities around the original cement mass; unilateral pedicle injection of bone cement successfully filled the cavity around the cement.
Some patients with BCD are not suitable for repeat VP because the cement has partially or completely migrated outside the vertebral body. In such cases, internal fixation surgery is required [2–4]. Zhang classified BCD into 4 types according to the characteristics of CT and MRI: in situ bone cement loosening, anterior migration of bone cement, anterior migration of bone cement accompanied by posterior movement of bone mass, and posterior migration of bone cement [6]. According to this classification method, only the first type is suitable for repeat VP. Whether in situ loosening is the beginning of BCD still requires further research. If it is, early detection and repeat VP may avoid open surgery.
Conclusions
BCD is a complication of PKP that can occur without trauma. CT can definitively establish the diagnosis. Repeat VP is an effective treatment option for managing this condition, even when only the unilateral pedicle is accessible.
Figures
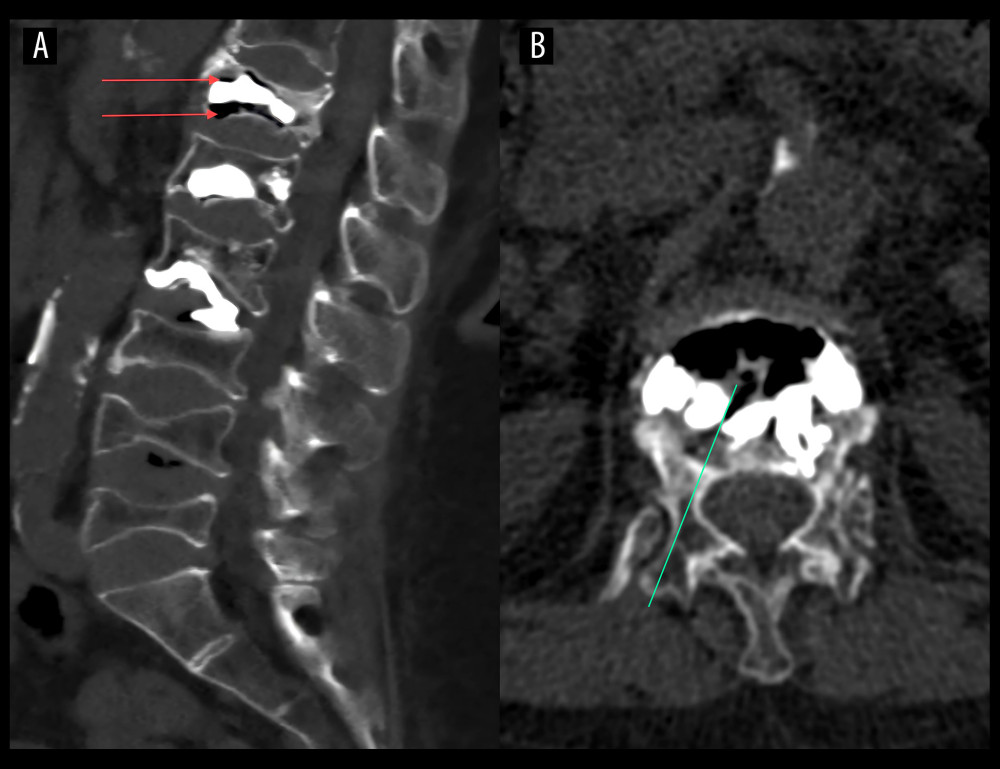 Figure 1. Computed tomography (CT) scan from a 71-year-old woman with bone cement dislodgement (BCD) following percutaneous kyphoplasty (PKP) of a T12 vertebral fracture before treatment with repeat vertebroplasty. (A) The scan shows a cavity around the cement, as indicated by the red arrows. (B) The CT scan shows a passage to the cavity, indicated by a green line.
Figure 1. Computed tomography (CT) scan from a 71-year-old woman with bone cement dislodgement (BCD) following percutaneous kyphoplasty (PKP) of a T12 vertebral fracture before treatment with repeat vertebroplasty. (A) The scan shows a cavity around the cement, as indicated by the red arrows. (B) The CT scan shows a passage to the cavity, indicated by a green line. 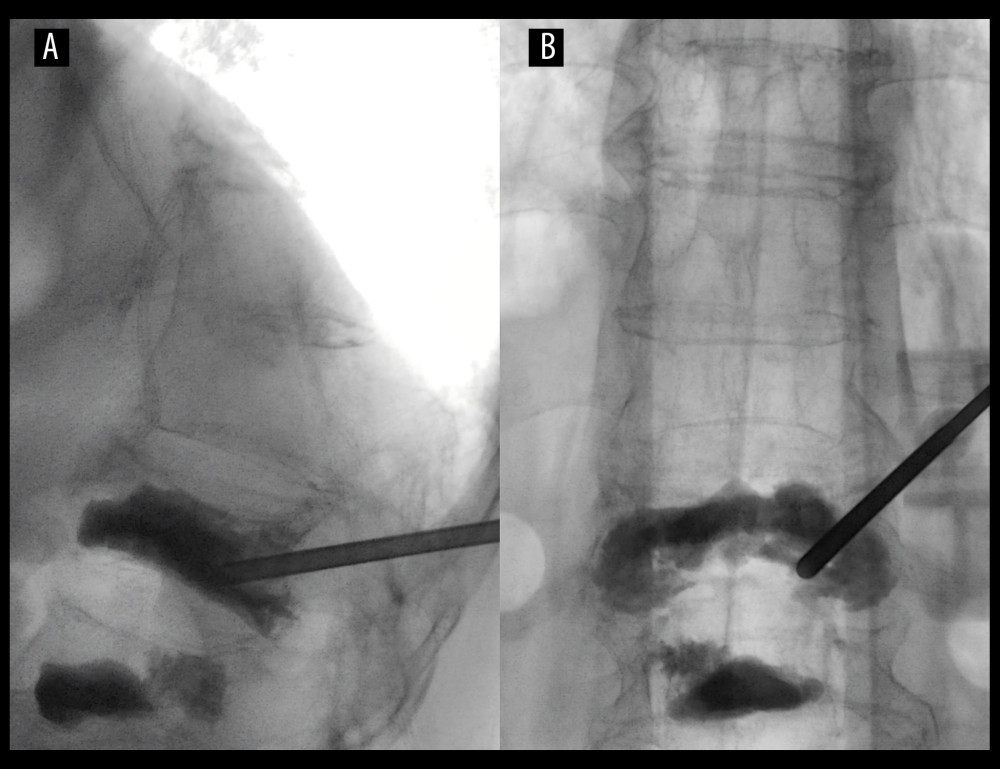 Figure 2. Intraoperative X-ray. (A) The X-ray shows the cannula was placed to the posterior two-thirds of the inferior endplate along the right pedicle. (B) The cannula was placed to the area not filled by the original bone cement.
Figure 2. Intraoperative X-ray. (A) The X-ray shows the cannula was placed to the posterior two-thirds of the inferior endplate along the right pedicle. (B) The cannula was placed to the area not filled by the original bone cement. 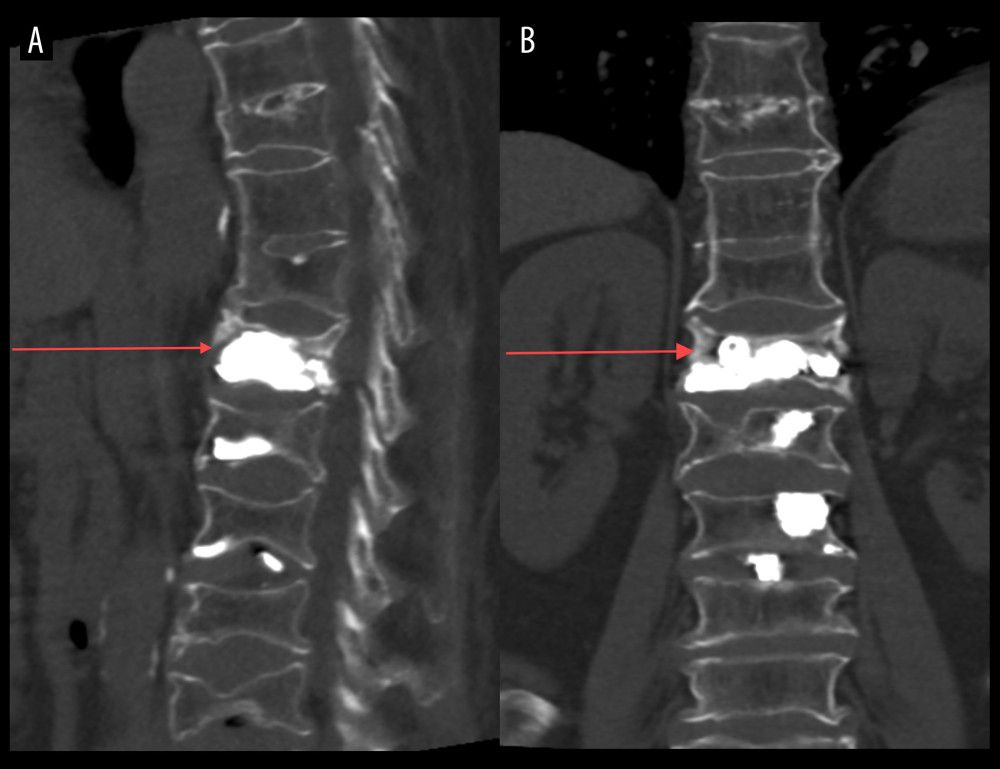 Figure 3. CT scan after the repeat VP. (A, B) Show the cavity was filled by cement, marked with red arrows.
Figure 3. CT scan after the repeat VP. (A, B) Show the cavity was filled by cement, marked with red arrows. References
1. Patel A, Petrone B, Carter KR, Percutaneous vertebroplasty and kyphoplasty: StatPearls May 30, 2023, Treasure Island (FL), StatPearls Publishing
2. Ha KY, Kim YH, Yoo SR, Molon JN, Bone cement dislodgement: One of complications following bone cement augmentation procedures for osteoporotic spinal fracture: J Korean Neurosurg Soc, 2015; 57(5); 367-70
3. Tsai TT, Chen WJ, Lai PL, Polymethylmethacrylate cement dislodgment following percutaneous vertebroplasty: A case report: Spine (Phila Pa 1976), 2003; 28(22); E457-E60
4. Kim CH, Kim P, Ju CI, Kim SW, Open surgery for osteoporotic compression fracture within one month of single level balloon kyphoplasty: Korean J Neurotrauma, 2023; 19(3); 348-55
5. Yonezawa Y, Yonezawa N, Kanazawa Y, Revision balloon kyphoplasty and vertebra-pediculoplasty using cannulated screws for osteoporotic vertebral fractures with cement dislodgement following conventional balloon kyphoplasty: J Neurointerv Surg, 2022; 14(8); 844-46
6. Zhang LL, Gan HF, Shi JH, Treatment analysis of bone cement displacement after vertebral augmentation: Chin J Orthop Trauma, 2023; 25(1); 19-24
7. Gao XC, Du JP, Chang Z, Risk factors for cement displacement after percutaneous vertebral augmentation for osteoporotic vertebral compression fracture: Chin J Trauma, 2022; 38(3); 205-12
8. Wang M, Jin Q, High-viscosity bone cement for vertebral compression fractures: A prospective study on intravertebral diffusion and leakage of bone cement: BMC Musculoskelet Disord, 2020; 21(1); 589
9. Guo J, Bai Y, Li L, A Comparative study of 2 techniques to avoid bone cement loosening and displacement after percutaneous vertebroplasty treating unstable Kummell disease: Neurospine, 2024; 21(2); 575-87
Figures
Figure 1. Computed tomography (CT) scan from a 71-year-old woman with bone cement dislodgement (BCD) following percutaneous kyphoplasty (PKP) of a T12 vertebral fracture before treatment with repeat vertebroplasty. (A) The scan shows a cavity around the cement, as indicated by the red arrows. (B) The CT scan shows a passage to the cavity, indicated by a green line.Figure 2. Intraoperative X-ray. (A) The X-ray shows the cannula was placed to the posterior two-thirds of the inferior endplate along the right pedicle. (B) The cannula was placed to the area not filled by the original bone cement.Figure 3. CT scan after the repeat VP. (A, B) Show the cavity was filled by cement, marked with red arrows. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133