27 May 2025: Articles 
A 61-Year-Old Man with Perforation of the Left Ventricle and Pericardium 3 Days After Insertion of a Cardiac Pacemaker Lead
Rare disease
Shanqing Bao ACE 1, Ke Yang BCD 1, Yuanhong Li AEF 1, Tenglong Wang BCDE 1, Chengxin Zhang ADFG 1*DOI: 10.12659/AJCR.947341
Am J Case Rep 2025; 26:e947341






Abstract
BACKGROUND: The use of implantable cardiac devices, including permanent pacemakers, has become routine, and reported complications are rare. However, in some cases, a cardiac pacemaker lead can perforate the ventricular or atrial wall. However, patients can present with nonspecific and heterogeneous clinical manifestations, leading to potential delays in diagnosis. We present a case of a 61-year-old man with perforation of the left ventricle and pericardium diagnosed 3 days after the insertion of a cardiac pacemaker lead.
CASE REPORT: A 61-year-old man with symptomatic second-degree type II sinoatrial block underwent uneventful dual-chamber permanent pacemaker implantation. On the evening of the third day following the pacemaker implantation procedure, the patient presented with persistent chest pain and was admitted to the hospital. Emergency chest computed tomography demonstrated that the right ventricular pacemaker lead had penetrated the left ventricle and pericardium. The patient underwent surgery on the fourth day of admission, and the pacing lead was secured to the left ventricular myocardium via a small incision in the left intercostal space. The surgical procedure was completed successfully, and the patient was discharged on the third postoperative day, without any complications.
CONCLUSIONS: Cardiac perforation due to the lead is a rare but potentially fatal complication of pacemaker implantation. We present a patient who presented with a left ventricular and pericardium perforation 3 days after pacemaker implantation. This clinical case underscores the necessity for screening for perforation in patients treated with cardiac implantable electronic devices prior to discharge.
Keywords: Pacemaker, Artificial, Foreign-Body Migration, Heart Injuries, Surgical Procedures, Operative, Humans, Male, Middle Aged, Pericardium, Heart Ventricles
Introduction
The use of implantable cardiac devices, encompassing permanent pacemakers, has become a customary medical procedure, which has a low incidence of reported complications [1]. Serious complications include battery dysfunction, implant site infection, and electrode lead breakage/displacement [2]. Cardiac perforation is a rare complication after pacemaker and implantable cardioverter-defibrillator implantation, with incidence rates ranging from 0% to 6.38% [3]. Perforation can occur acutely at the time of lead insertion or can be delayed for days, months, or even years. Symptoms vary widely in patients with lead perforation, and some patients can be underdiagnosed due to mild and asymptomatic symptoms [4]. The right ventricle is the most common site of cardiac perforation, primarily because this is a common site for ventricular leads, and because the myocardial wall is thinner here than at other common pacing sites, such as the interventricular septum and the right ventricular outflow tract [5,6]. In rare cases, the perforation crosses the interventricular septum and causes a left ventricular perforation [7].
This report describes 61-year-old man with perforation of the left ventricle and pericardium diagnosed at 3 days after insertion of a cardiac pacemaker lead.
Case Report
A 61-year-old male patient underwent permanent pacemaker implantation for second degree type II sinoatrial block. He was previously received a diagnosis of coronary artery disease and hypertension and underwent coronary stent implantation 6 months earlier. On the third day after pacemaker implantation, the patient developed persistent chest pain and came to our hospital. An electrocardiogram showed sinus rhythm (Figure 1), chest X-ray showed the right ventricular lead exceeding the left heart edge (Figure 2A), and chest computed tomography (CT) showed the pacing lead penetrating the left ventricle and pericardium (Figure 2B–2D). After the diagnosis was made, the patient underwent surgery. Intraoperative fluoroscopy was used to locate the pacing lead at the point of entry into the left ventricle (Figure 3A), a 4-cm skin incision was made at the appropriate thoracic site, and the subcutaneous tissue was incised to enter the left chest. The pacing lead penetrated the pericardium into the thoracic cavity for approximately 5 cm (Figure 3B), and the pericardium was incised to see that the lead was approximately 5 mm from the left anterior descending branch, with a small amount of bloody fluid in the pericardial cavity. Using 4-0 Prolene with a felt spacer, the purse-string was sutured to the left ventricular surface, and the suture was passed through the tip of the pacing lead (Figure 3C). The lead was slowly withdrawn into the ventricle and the purse-string was tightened and knotted to ensure that the tip of the lead was secured to the left ventricular myocardium. The pacemaker was tested for good function, and the lead was seen to be in a satisfactory position on fluoroscopy (Figure 3D). Postoperative chest CT showed that the position of the lead was fixed within the left ventricular myocardium, and the patient was discharged on day 3 after the procedure, without complications.
Discussion
Physicians should be familiar with the diagnosis and treatment of complications associated with pacemaker implantation, which include displacement of atrial and/or ventricular leads, necessitating repositioning; infection; pneumothorax requiring chest tube placement or prolonged hospitalization; hemothorax; cardiac tamponade; acute myocardial infarction; and death [8]. The incidence of cardiac perforation resulting from pacemaker implantation is relatively low but can potentially be life-threatening. In such cases, the leads can perforate the outside of the pericardium, increasing the risk of vascular or pulmonary injury [4]. The classification of perforation is dependent on the time of symptom onset, and thus can be categorized as acute (presenting within 24 h), subacute (within 30 days), or chronic (more than 30 days after implantation) [5]. The clinical presentation of cardiac perforation is highly variable and can include chest pain, dyspnea, hypotension, and shock. The most common presenting symptom is chest pain, which accounts for 46% of cases [9]. It can manifest in a variety of timeframes, but is most frequently observed in subacute episodes. Asymptomatic presentations are most prevalent in chronic cohorts and are frequently overlooked or misdiagnosed [10]. The diagnosis of cardiac perforation should be considered in all patients treated with pacemaker or combination devices, regardless of the duration of implantation. Our patient presented with a subacute episode of chest pain, which was likely caused by irritation of the chest wall and lung tissue by the lead tip.
It has been demonstrated that the prevalence of cardiac perforation can be elevated in instances in which active fixed leads are used [7]. The use of exposed and small-diameter lead tips has been identified as a risk factor for cardiac perforation. Similarly, excessive twisting of active fixed leads has been linked to an increased likelihood of this complication. The forced advancement of the myocardial wall or overextension of the fixation helix exerts additional stress on the myocardium [11]. Our patient was implanted with a permanent pacemaker with a helical lead, and the helical tip may have been overextended.
The diagnosis of perforation is primarily based on imaging findings, rather than on clinical features. In patients with suspected perforation, chest X-rays are useful for determining whether the location of the leads is anomalous, particularly when compared with the postoperative view [12]. Echocardiography is a straightforward, non-invasive examination that enables the assessment of electrode positioning and the detection of pacemaker lead tips within the pericardium. It is also a valuable tool for diagnosing pericardial effusion and pericardial tamponade, which are significant complications associated with lead perforation [13]. However, both diagnostic methods have inherent limitations, and the precise location of the pacemaker lead may not be accurately determined. A chest CT scan is considered a valuable diagnostic tool for identifying pacemaker lead perforation, as it can accurately demonstrate pacemaker lead displacement [14]. Recent studies have demonstrated that CT imaging has a 98.1% accuracy in diagnosing lead perforation, which is a superior diagnostic performance, compared with that of chest radiography (73.1%) and echocardiography (82.7%) [15]. However, the presence of artefacts from the exposed metal portion of the lead can result in an inability to accurately locate the lead, which is detrimental to the identification of minor perforations. Therefore, it is necessary to select an appropriate window for detection.
The optimal treatment for patients with perforations remains unclear. In accordance with the 2017 Heart Rhythm Society expert consensus statement, if lead perforation results in pain, bleeding, or other complications, lead removal will constitute an essential component of the patient’s comprehensive treatment plan [16]. Although it is less invasive, this approach can result in fatal complications, including pericardial tamponade or hemorrhagic shock. A small incision was made through the left intercostal space, allowing for the stable fixation of the pacing lead within the left ventricular myocardium, while avoiding the potential complications of pericardial tamponade and additional surgical incisions that can be caused by removing the lead. This approach is less invasive than open heart surgery, thereby avoiding the potential complications of sternotomy and prolonged hospitalization.
Conclusions
This study reports the case of a patient who presented with a left ventricular and pericardium perforation 3 days after pacemaker implantation and underwent a successful, minimally invasive repair of the perforation. This clinical case underscores the necessity for screening for perforation in patients treated with cardiac implantable electronic devices prior to discharge.
Figures
 Figure 1. Electrocardiogram is suggestive of sinus rhythm.
Figure 1. Electrocardiogram is suggestive of sinus rhythm. 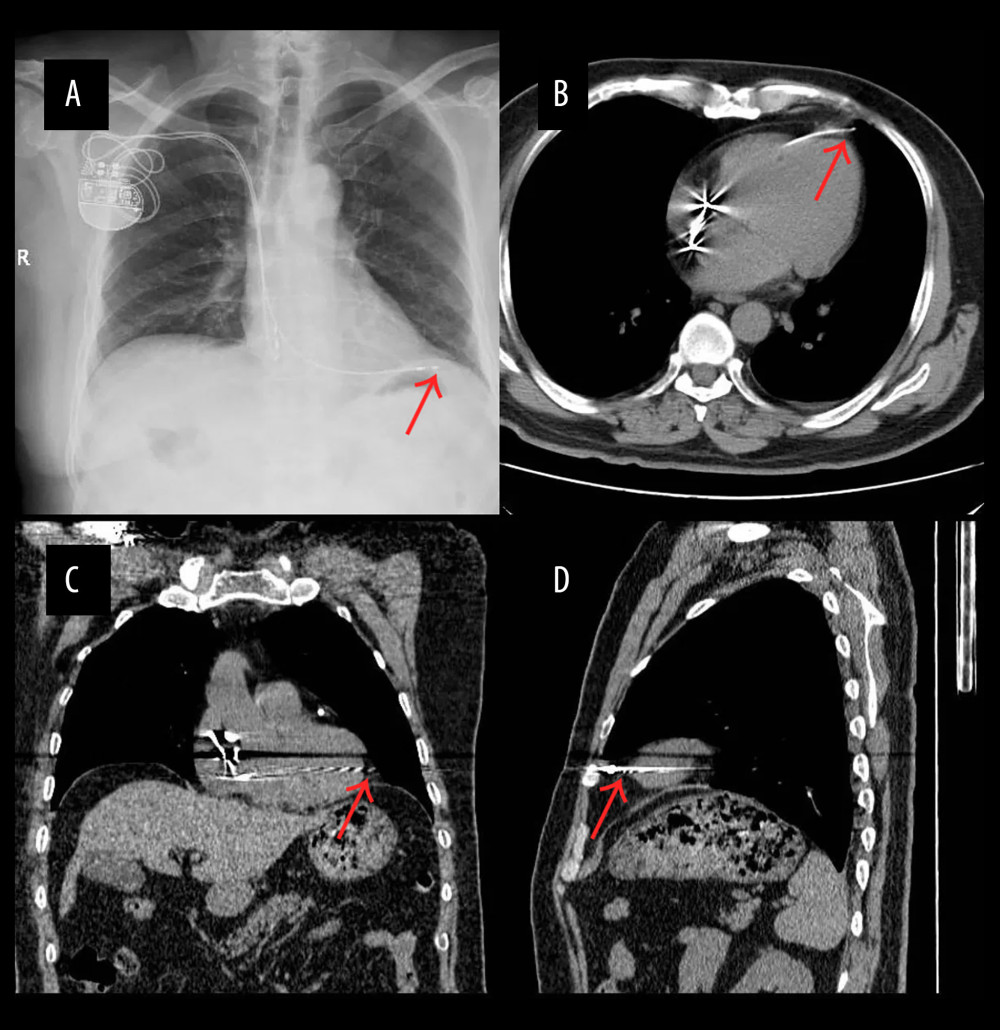 Figure 2. (A) Chest X-ray showed the right ventricular lead over the left edge of the heart. (B–D) Chest computed tomography showed the pacing lead crossing the left ventricle and pericardium.
Figure 2. (A) Chest X-ray showed the right ventricular lead over the left edge of the heart. (B–D) Chest computed tomography showed the pacing lead crossing the left ventricle and pericardium. 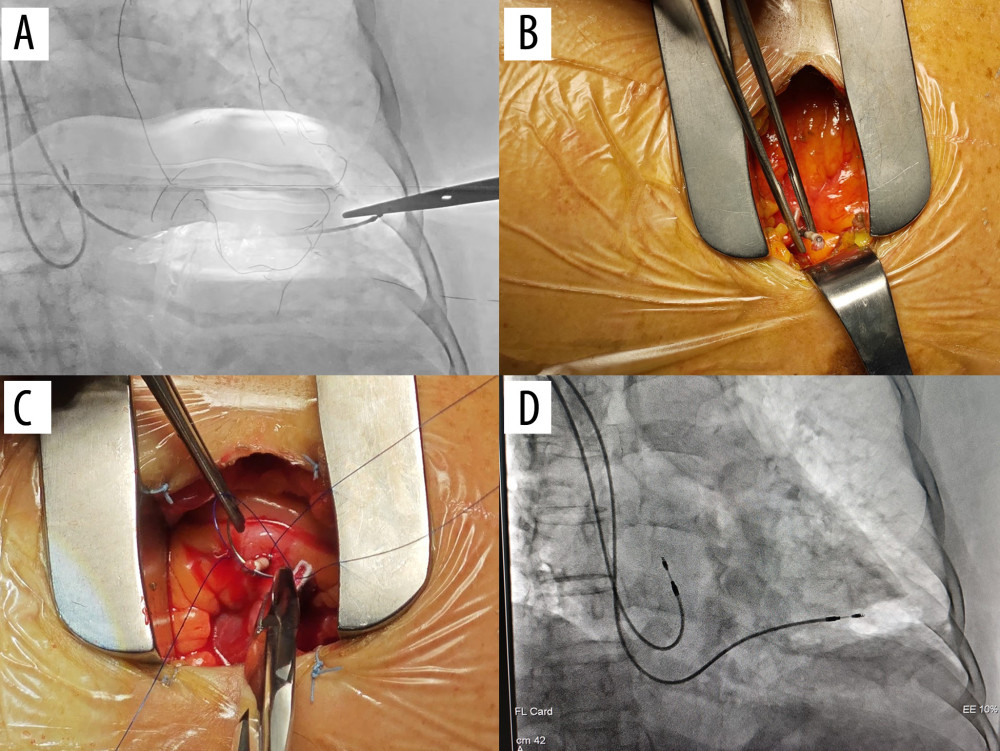 Figure 3. (A) Fluoroscopic positioning of the pacing lead at the point of penetration into the ventricle. (B) The pacing lead was advanced through the pericardium and into the thorax under. (C) A suture was passed through the tip of the lead. (D) Fluoroscopic image of the lead positioned within the left ventricle.
Figure 3. (A) Fluoroscopic positioning of the pacing lead at the point of penetration into the ventricle. (B) The pacing lead was advanced through the pericardium and into the thorax under. (C) A suture was passed through the tip of the lead. (D) Fluoroscopic image of the lead positioned within the left ventricle. References
1. Mahapatra S, Bybee KA, Bunch TJ, Incidence and predictors of cardiac perforation after permanent pacemaker placement: Heart Rhythm, 2005; 2(9); 907-11
2. Tobin K, Stewart J, Westveer D, Frumin H, Acute complications of permanent pacemaker implantation: their financial implication and relation to volume and operator experience: Am J Cardiol, 2000; 85(6); 774-76
3. Hamada Y, Sakaki M, Watanabe Y, Delayed right ventricular pacemaker lead perforation 9 years after implantation: Am J Case Rep, 2023; 24; e940291
4. Allouche E, Chargui S, Fathi M, Bezdah L, Subacute right ventricle perforation: A pacemaker lead complication: BMJ Case Rep, 2021; 14(5); e242489
5. Kumar P, Skrabal J, Frasure SE, Pourmand A, Pacemaker lead related myocardial perforation: Am J Emerg Med, 2022; 53; 281e1-e3
6. Vanezis AP, Prasad R, Andrews R, Pacemaker leads and cardiac perforation: JRSM Open, 2017; 8(3); 2054270416681432
7. Cano Ó, Andrés A, Alonso P, Incidence and predictors of clinically relevant cardiac perforation associated with systematic implantation of active-fixation pacing and defibrillation leads: A single-centre experience with over 3800 implanted leads: Europace, 2017; 19(1); 96-102
8. Dijkshoorn LA, Smeding L, Pepplinkhuizen S, Fifteen years of subcutaneous implantable cardioverter-defibrillator therapy: Where do we stand, and what will the future hold?: Heart Rhythm, 2025; 22(1); 150-58
9. Fiorillo G, Ghazihosseini S, Agizza S, Management of iatrogenic atrial perforation caused by pacemaker electrodes: A case report: J Med Case Rep, 2024; 18(1); 524
10. Waddingham PH, Elliott J, Bates A, Iatrogenic cardiac perforation due to pacemaker and defibrillator leads: a contemporary multicentre experience: Europace, 2022; 24(11); 1824-33
11. Sterliński M, Przybylski A, Maciag A, Subacute cardiac perforations associated with active fixation leads: Europace, 2009; 11(2); 206-12
12. Rajkumar CA, Claridge S, Jackson T, Diagnosis and management of iatrogenic cardiac perforation caused by pacemaker and defibrillator leads: Europace, 2017; 19(6); 1031-37
13. Caiati C, Pollice P, Truncellito L, Minimal cardiac perforation by lead pacemaker complicated with pericardial effusion and impending tamponade: Optimal management with no pericardiocentesis driven by echocardiography: Diagnostics (Basel), 2020; 10(4); 191
14. Balabanoff C, Gaffney CE, Ghersin E, Radiographic and electrocardiography-gated noncontrast cardiac CT assessment of lead perforation: Modality comparison and interobserver agreement: J Cardiovasc Comput Tomogr, 2014; 8(5); 384-90
15. Zhang X, Zheng C, Wang P, Assessment of cardiac lead perforation: Comparison among chest radiography, transthoracic echocardiography and electrocardiography-gated contrast-enhanced cardiac CT: Eur Radiol, 2019; 29(2); 963-74
16. Kusumoto FM, Schoenfeld MH, Wilkoff BL, 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction: Heart Rhythm, 2017; 14(12); e503-e51
Figures
Figure 1. Electrocardiogram is suggestive of sinus rhythm.Figure 2. (A) Chest X-ray showed the right ventricular lead over the left edge of the heart. (B–D) Chest computed tomography showed the pacing lead crossing the left ventricle and pericardium.Figure 3. (A) Fluoroscopic positioning of the pacing lead at the point of penetration into the ventricle. (B) The pacing lead was advanced through the pericardium and into the thorax under. (C) A suture was passed through the tip of the lead. (D) Fluoroscopic image of the lead positioned within the left ventricle. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133