28 April 2025: Articles 
Post-COVID-19 Guillain-Barré Syndrome with GM1 and GD1b Antibodies: A Case Study and Literature Review
Rare coexistence of disease or pathology
Mrudula ThiriveediDOI: 10.12659/AJCR.947416
Am J Case Rep 2025; 26:e947416






Abstract
BACKGROUND: The coronavirus disease 2019 (COVID-19) pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has led to the emergence of various neurological complications, including Guillain-Barré syndrome (GBS). GBS is an acute, immune-mediated disorder characterized by progressive weakness, sensory deficits, and autonomic dysfunction. Anti-ganglioside antibodies are often seen in GBS; however, they are rarely reported in the setting of COVID-19-related GBS. We present a case of post-COVID-19 GBS with positive GM1 and GD1b antibodies.
CASE REPORT: An 86-year-old man presented with progressive quadriparesis, sensory deficits, and hyporeflexia 4 weeks after COVID-19 infection. Brain and spine imaging were unremarkable. Cerebrospinal fluid (CSF) analysis revealed albuminocytological dissociation, consistent with acute inflammatory demyelinating polyneuropathy (AIDP). Despite 2 courses of intravenous immunoglobulin (IVIG), the patient showed minimal improvement in muscle strength. Nerve conduction studies (NCS) revealed severe sensorimotor polyneuropathy, with axonal and demyelinating features. Serum testing showed elevated GM1 and GD1b anti-ganglioside antibody titers.
CONCLUSIONS: Although numerous cases of COVID-19-related GBS have been reported, anti-ganglioside antibody positivity, particularly GM1 and GD1b, is uncommon. The underlying mechanism is presumed to be autoimmune, likely triggered by molecular mimicry. Our case contributes to the evolving understanding of GBS immunology in the context of COVID-19. Although this case report may not alter current GBS management, the co-occurrence of GM1 and GD1b antibodies in post-COVID-19 GBS underscores the need for continued vigilance, immunological profiling, and research into potential prognostic and therapeutic implications.
Keywords: COVID-19, Guillain-Barré syndrome, Antibodies, Humans, Male, G(M1) Ganglioside, Aged, 80 and over, Gangliosides, Autoantibodies, Pandemics, SARS-CoV-2, Immunoglobulins, Intravenous
Introduction
Guillain-Barré syndrome is an immune-mediated polyneuropathy that affects the peripheral nervous system [1]. It is characterized by acute or subacute onset of weakness and/or abnormal sensation involving the extremities and cranial nerve innervated muscles, reduced or absent deep tendon reflexes, and the presence of albuminocytological dissociation in the CSF [2]. It is often preceded by an acute illness caused by pathogens such as Cytomegalovirus, Zika virus, Epstein-Barr virus, Campylobacter jejuni, Influenza, and, potentially, SARS-CoV-2. The disease classically starts in the acute phase 1–2 weeks after the immune stimulation, with peak clinical findings 2–4 weeks after the stimulation [3]. The mechanism is thought to be autoimmune, stemming from molecular mimicry, but the complex interplay between the host and microbe factors is not well understood. There are numerous articles citing the pathological role of the ACE 2 (angiotensin-converting enzyme) receptor and heat shock protein (HSP) [2].
GBS occurs worldwide, with an overall incidence rate of 1–2 cases per 100 000 people per year [1]. A meta-analysis of studies from North America and Europe showed an exponential increase in GBS incidence, from 0.6 to 2.66 per 100 000 person-years, across all age groups. The incidence increases by 20% for every 10-year increase in age, with higher risk in males than females [4]. During the COVID-19 pandemic, a notable increase in GBS cases was reported in some populations. However, some studies suggest a decline in GBS cases, likely due to reduced exposure to pathogens and due to social distancing [2]. Some cases of GBS occurred as post-infectious or para-infectious phenomena, without consistent evidence [5].
Gangliosides are molecular markers, expressed on peripheral nerves, that are important in the maintenance and repair of neurons. They also participate in synaptic transmission and play a central role in the molecular mimicry pathophysiology of GBS. The molecular mimicry triggered by previous infection results in formation of anti-ganglioside antibodies that attack proteins in the axonal membrane. This results in a rapidly progressive ascending flaccid paresis; it can also affect sensory fibers and cranial nerves. Different types of anti-ganglioside antibodies are noted in GBS, including GM1, GD1a, GQ1b, and GD1b. GM1 is the most common ganglioside antibody found in patients with classic GBS, while GQ1b is associated with Miller-Fisher syndrome (MFS). A study revealed positive GM1 antibodies in 88% of patients with classic GBS [6]. GM1 antibodies are frequently associated with motor dysfunction whereas GD1b is seen in sensory forms of GBS [7].
Case Report
The patient was an 86-year-old man with a medical history of hypertension, gastroesophageal reflux, obstructive sleep apnea on continuous positive airway pressure (CPAP), and recent COVID-19 infection treated with a 5-day course of Nirmatrelvir/Ritonavir (Paxlovid). Approximately 4 weeks after the start of infection, he was hospitalized for partial small-bowel obstruction, managed conservatively, and discharged. Five days later, he returned with progressive generalized weakness, difficulty ambulating, and inability to use his walker. He reported no bowel movement since discharge.
The patient denied falls, vision changes, paresthesias, dysphagia, fever, weight loss, or urinary/stool incontinence. His vital signs were stable, and the general exam was unremarkable. Neurological evaluation revealed intact cranial nerves, 4/5 strength in all extremities, diminished pain and vibration sensation, and diffuse hyporeflexia (1+). Gait was not assessed due to weakness.
Initial labs, including comprehensive metabolic panel (CMP), creatinine kinase (CK), thyroid stimulating hormone (TSH), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), vitamin B12, and folate, were normal. Computed tomography (CT) of the head showed an age-indeterminate infarct in the left occipital lobe. Magnetic resonance imaging (MRI) of the brain ruled out an acute infarct, and cervical spine MRI showed no disc herniation or cord compression. Magnetic resonance angiography (MRA) of the head and neck showed no large-vessel occlusion. Abdominal imaging revealed constipation and mild ileus.
On hospital day 2, the patient’s strength declined to 2/5 in all limbs. Sensory loss progressed, and reflexes were absent in his knees, ankles, and the left biceps. Coordination and gait could not be assessed due to weakness. Given the rapid progression and recent COVID-19 infection, acute inflammatory demyelinating polyneuropathy (AIDP) was suspected. MRI of the thoracic and lumbar spine revealed no acute pathology.
CSF analysis showed albuminocytologic dissociation (WBC 1, protein 95.9 mg/dL), consistent with GBS. He was started on IVIG at 400 mg/kg/day for 5 days, with minimal improvement. Plasma exchange (PLEX) was considered but was unavailable locally. Attempts to transfer the patient were unsuccessful, so a second IVIG course was administered per Neurology recommendation.
Nerve conduction studies on hospital day 14 demonstrated severe sensorimotor polyneuropathy with axonal and demyelinating features. Compound muscle action potentials (CMAPs) showed absent responses in the median, ulnar, and tibial nerves bilaterally, while left peroneal and tibial nerves showed prolonged latency, decreased amplitude, and conduction velocities (Figure 1). Sensory nerve action potentials (SNAPs) were absent across tested nerves (Figure 2).
Serum testing revealed elevated anti-ganglioside antibody titers: GM1 at 1: 16 000 (reference <1: 2000) and positive GD1b at <1: 2000 (reference <1: 2000). These findings supported an immune-mediated etiology.
The hospital course was complicated by hyponatremia (lowest sodium 119 mmol/L on day 7) and encephalopathy. He was managed in the intensive care unit with hypertonic saline, leading to gradual improvement in sodium levels and mental status. Physicians need to be more vigilant and consider early escalation of care, as this can be a rapidly progressive disease. Constipation was treated with laxatives. His respiratory and swallowing functions remained intact. Painful neuropathy developed and was managed with gabapentin.
Despite 2 courses of IVIG and physical and occupational therapy, the patient showed minimal motor recovery (persistent 2/5 strength in all limbs). For ongoing rehabilitation and supportive care, he was discharged to a long-term acute care facility after a 24-day hospitalization.
Discussion
Guillain-Barré syndrome (GBS) has emerged as a notable neurological complication in the context of COVID-19 infection and vaccination [8–10]. In our case, an elderly patient developed post-infectious quadriparesis with elevated GM1 and GD1b antibodies, an uncommon finding in COVID-19-related GBS. Advanced age and immunosenescence likely contributed to disease severity [11].
Hyponatremia, as seen in our patient, is a recognized complication of intravenous immunoglobulin (IVIG) therapy. It can result from pseudohyponatremia due to increased serum proteins or from translocational shifts [12,13]. Syndrome of inappropriate antidiuretic hormone secretion (SIADH), associated with GBS, is another possible cause [14]. In our case, sodium normalization after IVIG supported pseudohyponatremia as the likely etiology. Dysautonomia likely explained the concurrent constipation.
Electrodiagnostic studies are essential for confirming GBS subtype and assessing prognosis [15]. In our patient, nerve conduction testing was a limited study, which showed absent motor and sensory responses in multiple nerves, suggesting a severe, mixed axonal and demyelinating sensorimotor neuropathy. A retrospective study conducted on 365 GBS patients between 1998 and 2013 noted that a single electrophysiological study may suffice to establish the electrodiagnosis of GBS subtype based on the modified criteria when performed in the first 3 weeks of symptom onset [16].
Although not essential for diagnosis, anti-ganglioside antibody testing is valuable in atypical or severe presentations. Several antibodies – GM1, GD1a, GD1b, GQ1b, and GM2 – have been reported in COVID-19-associated GBS [17–19]. Our literature review revealed only 3 previous cases of GBS after COVID-19 infection specifically with positive GM1 antibodies. Our patient is the fourth such case.
In 2020, Petrelli et al reported a case involving pure motor axonal neuropathy [20], while Civardi et al described a 72-year-old woman with favorable response to IVIG but requiring respiratory support [21]. Dufour et al reported a younger patient with good recovery [15]. Compared to these cases, our patient had both axonal and demyelinating neuropathy and did not experience respiratory compromise, although significant weakness persisted (Table 1).
Studies have observed a lower prevalence of anti-GM1 and anti-GQ1b antibodies in COVID-19-related GBS, suggesting a potentially distinct pathophysiology from classical GBS [22,23]. While the GM1 and GD1b antibodies in our patient may reflect an incidental finding, their presence raises questions about possible antigenic triggers in SARS-CoV-2 infection.
Elevated anti-GM1 titers are associated with poorer long-term motor recovery and increased risk of persistent disability [24]. Anti-GQ1b antibodies, in contrast, tend to predict more favorable outcomes [11]. The prognostic value of GD1a and GD1b antibodies remains unclear, although some studies suggest GD1a is associated with worse outcomes [25].
Importantly, large-cohort studies have not shown consistent differences in disease severity, course, or outcomes between COVID-19-associated and non-COVID-19 GBS. However, other reports suggest COVID-related GBS has greater severity and slower recovery [26].
Standard GBS treatment includes IVIG or plasma exchange (PLEX). For refractory cases, emerging therapies like complement inhibitors (eg, eculizumab) and IgG-cleaving enzymes (e.g., imlifidase) are under investigation. Eculizumab has shown mixed results; 1 trial found no significant improvement in motor recovery [27]. FcRn antagonists, which lower IgG levels, are also being explored but require further clinical validation.
Conclusions
This case underscores the neurological complications of COVID-19, highlighting GBS as a severe post-infectious sequela. The presence of GM1 and GD1b antibodies in COVID-19-related GBS remains rare, warranting further research into its pathophysiology, prognostic implications, and novel therapeutic strategies. Clinicians should remain vigilant for atypical presentations and consider alternative treatment approaches in refractory cases. Increased reporting of such cases may help refine treatment guidelines and improve patient outcomes.
Figures
 Figure 1. Nerve conduction studyCompound muscle action potential (CMAP) of the nerves, including left median, right median, left ulnar, right ulnar, right peroneal and right tibial, showed no responses. CMAP of the left peroneal and left tibial nerves showed prolonged latency and decreased amplitude and conduction velocities.
Figure 1. Nerve conduction studyCompound muscle action potential (CMAP) of the nerves, including left median, right median, left ulnar, right ulnar, right peroneal and right tibial, showed no responses. CMAP of the left peroneal and left tibial nerves showed prolonged latency and decreased amplitude and conduction velocities. 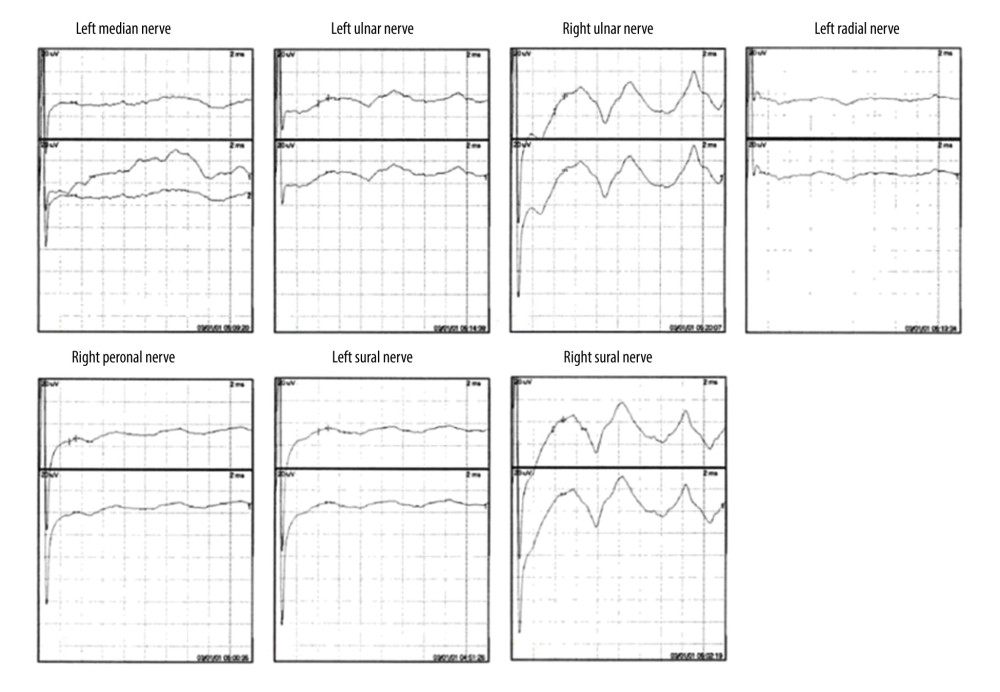 Figure 2. Nerve conduction studySensory nerve action potential (SNAP) of the nerves, including left median, left ulnar, right ulnar, left radial, right peroneal, left sural, and right sural, showed no responses.
Figure 2. Nerve conduction studySensory nerve action potential (SNAP) of the nerves, including left median, left ulnar, right ulnar, left radial, right peroneal, left sural, and right sural, showed no responses. 
References
1. Bragazzi NL, Kolahi AA, Nejadghaderi SA, Global, regional, and national burden of Guillain-Barré syndrome and its underlying causes from 1990 to 2019: J Neuroinflammation, 2021; 18(1); 264
2. Pimentel V, Luchsinger VW, Carvalho GL, Guillain-Barré syndrome associated with COVID-19: A systematic review: Brain Behav Immun Health, 2023; 28; 100578
3. Leonhard SE, Mandarakas MR, Gondim FAA, Diagnosis and management of Guillain-Barré syndrome in ten steps: Nat Rev Neurol, 2019; 15(11); 671-83
4. Sejvar JJ, Baughman AL, Wise M, Morgan OW, Population incidence of Guillain-Barré syndrome: A systematic review and meta-analysis: Neuroepidemiology, 2011; 36(2); 123-33
5. Freire M, Andrade A, Sopeña B, Guillain Barré syndrome associated with COVID-19-lessons learned about its pathogenesis during the first year of the pandemic, a systematic review: Autoimmun Rev, 2021; 20(8); 102875
6. Basta I, Suturkova L, Vujić A: Srp Arh Celok Lek, 2005; 133(3–4); 123-28
7. Yuki N, Guillain-Barré syndrome and anti-ganglioside antibodies: A clinician-scientist’s journey: Proc Jpn Acad Ser B Phys Biol Sci, 2012; 88(7); 299-326
8. Lim SH, Ju HJ, Han JH, Autoimmune and autoinflammatory connective tissue disorders following COVID-19: JAMA Netw Open, 2023; 6(10); e2336120
9. Chan M, Han SC, Kelly S, Tamimi M, A case series of Guillain-Barré syndrome after COVID-19 infection in New York: Neurol Clin Pract, 2021; 11(4); e576-e78
10. Keh RYS, Scanlon S, Datta-Nemdharry P, COVID-19 vaccination and Guillain-Barré syndrome: Analyses using the National Immunoglobulin Database: Brain, 2023; 146(2); 739-48
11. Goronzy JJ, Weyand CM, Immune aging and autoimmunity: Cell Mol Life Sci, 2012; 69(10); 1615-23
12. Steinberger BA, Ford SM, Coleman TA, Intravenous immunoglobulin therapy results in post-infusional hyperproteinemia, increased serum viscosity, and pseudohyponatremia: Am J Hematol, 2003; 73(2); 97-100
13. Nguyen MK, Rastogi A, Kurtz I, True hyponatremia secondary to intravenous immunoglobulin: Clin Exp Nephrol, 2006; 10(2); 124-26
14. Netto AB, Chandrahasa N, Koshy SS, Taly AB, Hyponatremia in Guillain-Barre syndrome: A review of its pathophysiology and management: Can J Neurol Sci, 2025; 52(1); 9-19
15. Dufour C, Co TK, Liu A, GM1 ganglioside antibody and COVID-19 related Guillain Barre ayndrome – a case report, systemic review and implication for vaccine development: Brain Behav Immun Health, 2021; 12; 100203
16. Rajabally YA, Durand MC, Mitchell J, Electrophysiological diagnosis of Guillain-Barré syndrome subtype: Could a single study suffice?: J Neurol Neurosurg Psychiatry, 2015; 86(1); 115-19
17. Gutiérrez-Ortiz C, Méndez-Guerrero A, Rodrigo-Rey S, Miller Fisher syndrome and polyneuritis cranialis in COVID-19: Neurology, 2020; 95(5); e601-e5
18. Lantos JE, Strauss SB, Lin E, COVID-19-associated Miller Fisher syndrome: MRI findings: Am J Neuroradiol, 2020; 41(7); 1184-86
19. Gigli GL, Bax F, Marini A, Guillain-Barré syndrome in the COVID-19 era: Just an occasional cluster?: J Neurol, 2021; 268(4); 1195-97
20. Petrelli C, Scendoni R, Paglioriti M, Logullo FO, Acute motor axonal neuropathy related to COVID-19 infection: A new diagnostic overview: J Clin Neuromuscul Dis, 2020; 22(2); 120-21
21. Civardi C, Collini A, Geda DJ, Geda C, Antiganglioside antibodies in Guillain-Barré syndrome associated with SARS-CoV-2 infection: J Neurol Neurosurg Psychiatry, 2020; 91(12); 1361-62
22. Racke MK, Niles JK, Lorenz RA, Kaufman HW, Changes in ganglioside antibody positivity rates during the COVID-19 pandemic: J Neuroimmunol, 2022; 367; 577877
23. Thomma RCM, Fokke C, Walgaard C, High and persistent anti-GM1 antibody titers are associated with poor clinical recovery in Guillain-Barré syndrome: Neurol Neuroimmunol Neuroinflamm, 2023; 10(4); e200107
24. van den Berg LH, Marrink J, de Jager AE, Anti-GM1 antibodies in patients with Guillain-Barré syndrome: J Neurol Neurosurg Psychiatry, 1992; 55(1); 8-11
25. Lleixà C, Martín-Aguilar L, Pascual-Goñi E, Autoantibody screening in Guillain-Barré syndrome: J Neuroinflammation, 2021; 18(1); 251
26. Filosto M, Cotti Piccinelli S, Gazzina S, Guillain-Barré syndrome and COVID-19: An observational multicentre study from two Italian hotspot regions: J Neurol Neurosurg Psychiatry, 2021; 92(7); 751-56
27. Kuwabara S, Kusunoki S, Kuwahara M, Efficacy and safety of eculizumab in Guillain-Barré syndrome: A phase 3, multicenter, double-blind, randomized, placebo-controlled clinical trial: J Peripher Nerv Syst, 2024; 29(3); 339-49
Figures
Figure 1. Nerve conduction studyCompound muscle action potential (CMAP) of the nerves, including left median, right median, left ulnar, right ulnar, right peroneal and right tibial, showed no responses. CMAP of the left peroneal and left tibial nerves showed prolonged latency and decreased amplitude and conduction velocities.Figure 2. Nerve conduction studySensory nerve action potential (SNAP) of the nerves, including left median, left ulnar, right ulnar, left radial, right peroneal, left sural, and right sural, showed no responses. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133