29 June 2025: Articles 
Differential Diagnosis and a Novel Mutation in Birt-Hogg-Dubé Syndrome: Insights from 2 Cases
Challenging differential diagnosis, Unusual setting of medical care, Rare disease
Lingfang Tu ACE 1, Yuan Ye BEG 1, Jianya Zhou CF 1, Zhijie Pan AD 1*DOI: 10.12659/AJCR.947530
Am J Case Rep 2025; 26:e947530






Abstract
BACKGROUND: Birt-Hogg-Dubé (BHD, OMIM# 135150) syndrome is an inherited autosomal dominant disorder predominantly caused by mutation of FLCN gene, which encodes for folliculin. Although FLCN has been suggested to be involved in the mechanistic target of the rapamycin (mTOR) signaling pathway, the functional role of folliculin is poorly understood. BHD is characterized by skin abnormalities, pulmonary cysts, spontaneous pneumothorax, and kidney neoplasms. BHD can be asymptomatic or occur with symptoms such as cough or shortness of breath, or in extremis after an episode of spontaneous pneumothorax. The purpose of this report is to describe 2 Chinese cases of BHD syndrome, with a literature review of this rare disease.
CASE REPORT: The patients were 2 Chinese women diagnosed as BHD syndrome, aged 57 and 58 years old. Both patients had a history of pneumothorax, and physical examination revealed skin abnormalities. High-resolution computed tomography (HRCT) demonstrated sparsely-distributed, thin-walled lung cysts. Whole-exome sequencing (WES) analysis identified a mutation in the FLCN gene, confirming the diagnosis of BHD. In addition, a novel pathogenic variant of FLCN mutation in exon 12 (NM_144997.5: c.1341delC, p.Thr448Profs*20) was identified, and this is the first report of an unprecedented FLCN mutation in exon 12.
CONCLUSIONS: As an autosomal dominant hereditary disease, BHD should be distinguished from emphysema, TSC, LAM, and other diffuse cystic lung diseases for differential diagnosis. When BHD is suspected, identification of pathogenic FLCN germline mutations is essential for a definitive diagnosis.
Keywords: Pneumothorax, Kidney Neoplasms, Skin Abnormalities, Humans, Birt-Hogg-Dube Syndrome, Female, Middle Aged, Proto-Oncogene Proteins, Diagnosis, Differential, Tumor Suppressor Proteins, Mutation
Introduction
Birt-Hogg-Dubé syndrome (BHD syndrome, also known as Hornstein-Knickenberg syndrome, OMIM# 135150), characterized by skin abnormalities, pulmonary cysts, spontaneous pneumothorax, and kidney neoplasms, is a rare autosomal dominant disorder predominantly induced by germline mutation in the
In 1975, Hornstein and Knickenberg first described this syndrome [14], which is currently regarded as a rare disorder. The epidemiology of this rare disease is largely unknown. Muller et al [15] found the prevalence of BHD in the general population is about 2 per million, with no sex predilection. In a nationwide population-based study performed in South Korea, the prevalence of BHD was 0.57 per million, with no peak age [16]. Clinical manifestations of BHD include dermatological lesions (such as fibrofolliculomas, trichodiscomas, and acrochordons), kidney and lung cysts, spontaneous pneumothorax, kidney neoplasms, colon polyps, and colorectal cancers [6,17,18]. Typical clinical presentations and detection of
Case Reports
CASE 1:
A 57-year-old Chinese woman was admitted to the Department of Respiratory and Critical Care Medicine in the First Affiliated Hospital of Zhejiang University School of Medicine (Hangzhou, China). Her chief concern was chest tightness for 3 days. She had a history of hypertension for 5 years and diabetes mellitus for 20 years, and no history of smoking, alcohol, or drug abuse. Levamlodipine (2.5 mg, once daily) was prescribed to control blood pressure, and metformin (1000 mg, twice daily), glimepiride (4 mg, once daily), and acarbose (50 mg, twice daily) were given to control blood glucose. She reported a prior history of recurrent spontaneous pneumothorax during 10 years ago, and thoracoscopic bullectomy with pleurodesis was performed to reduce recurrent pneumothorax. She also reported a history of familial pneumothorax in her father, younger brother, and son, but none of them had received genetic evaluation. Physical examination in the patient revealed multiple dome-shaped, whitish or skin-colored papules on the nose, cheeks, neck, and auricles (Figure 1A–1C), and several papules on the mucosal surface of the lower lip (Figure 1D), and the breath sound was completely absent in the left lower lobe. Skin abnormalities on the face were diagnosed as fibrofolliculomas by skin biopsy (Figure 2A, 2B) and papules on the neck were diagnosed as skin tags. Chest high-resolution computed tomography (HRCT) was performed and demonstrated sparsely-distributed, thin-walled lung cysts in the lower lobes, with a large pneumothorax in the left hemithorax and mild pneumothorax in the right hemithorax (Figure 3A–3C). After treatment with insertion of an indwelling drainage device, the pneumothorax was obviously reduced (Figure 3D–3F). Renal magnetic resonance imaging (MRI) revealed multiple renal cysts (Figure 4A, 4B). Laboratory tests found that C-reactive protein was slightly high (11.8 mg/L, normal range <8 mg/L). The patient showed a poor glycemic control, as fasting blood glucose level (8.41 mmol/L, normal range 3.9–6.1 mmol/L), HbA1% (9.9%, normal range 6.3–9.0%) and HbA1c% (8.4%, normal range 4.2–6.2%) were obviously high. There were no obvious abnormalities in the complete blood count, arterial blood gas analysis, liver and kidney functions, autoimmune antibodies, or tumor markers. WES analysis identified a novel mutation of the FLCN gene in exon 12 (NM_144997.5: c.1341delC, p.Thr448Profs*20) (Figure 5A), confirming the diagnosis of BHD. After 1-week treatment, her respiratory symptoms were significantly improved and the chest tube was removed. Poor dietary habits and irregular monitoring for blood glucose levels were the main reasons for poor glycemic control. The patient was advised to have regular follow-up visits in the endocrinology outpatient clinic. During follow-up, she had no recurrence of pneumothorax, but her blood glucose levels were uncontrolled due to poor dietary patterns and non-adherence to monitoring.
CASE 2:
A 58-year-old Chinese woman visited our outpatient clinic for respiratory disease in the First Affiliated Hospital of Zhejiang University School of Medicine (Hangzhou, China), and she had recurrent episodes of pneumothorax. Thoracoscopic bullectomy with pleurodesis was performed and there was no recurrence of spontaneous pneumothorax after this treatment. She reported no chronic diseases, and her family history of kidney neoplasms or genetic disorders was negative. Physical examination revealed dome-shaped skin papules on her face and neck (Figure 1E, 1F). Complete blood count, liver and kidney functions were normal. Chest HRCT was demonstrated multiple thin-walled lung cysts, mainly distributed in the subpleural and basilar medial regions of the lung (Figure 3G–3I). Abdominal MRI or CT was not performed in this patient. WES analysis identified a mutation of FLCN gene in exon 14 (NM_144997.5: c.1579_1580insA, p.Arg527Glnfs*75) (Figure 5B), leading to the diagnosis of BHD. During follow-up, she had no obvious respiratory symptoms and her pulmonary function was normal.
Discussion
In 1975, Hornstein and Knickenberg first described perifollicular fibromatosis with polyps of the colon in 2 sibs[14]. In 1977, Birt, Hogg, and Dubé reported a family in which several members had skin abnormalities, consisting of fibrofolliculomas, trichodiscomas, and acrochordons (skin tags) [19]. This disorder was subsequently known as BHD syndrome, and it is currently considered an autosomal dominant hereditary disease characterized by dermatologic lesions, lung cysts, spontaneous pneumothorax, and kidney neoplasms [20]. The prevalence of BHD is 1.86 per million in men and 1.88 per million in women [15]. Here, we reported 2 Chinese cases of BHD syndrome with typical dermatological lesions, spontaneous pneumothorax, pulmonary cysts, and mutation of the
The tumor-suppressor gene
Folliculin-interacting protein 1 (FNIP1) and FNIP2 form a complex with the C-terminus of FLCN, and the complex interacts with AMPK [8,25], which can act as a critical sensor of cellular metabolism and a negative regulator of mTOR [8,26,27]. Previous studies demonstrated a conflicting role for
BHD has great clinical heterogeneity, ranging from asymptomatic to variable phenotypic features of the skin, lungs, and kidneys. Our 2 patients presented with typical clinical features of BHD syndrome, including lung cysts, recurrent pneumothorax, cutaneous abnormalities, and renal cysts. Irregular and variable pulmonary cysts is a characteristic feature of BHD, affecting 80% or more of BHD patients [6,22,44]. Compared with sporadic primary pneumothorax, where pulmonary cysts are mainly distributed in the apical predominance, lung cysts of BHD tend to be located in the basal lung regions [2]. BHD-affected patients have an increased risk of recurrent spontaneous pneumothorax, which may be associated with the rupture propensity of lung cysts [45]. Familial pneumothorax is found in about 35% of patients with BHD, and approximately 24% of BHD patients have a history of spontaneous pneumothorax [46], and the average age at the first episode of pneumothorax is 36–38 years [22,46,47]. Studies suggested that Asian patients with BHD had a higher incidence of pneumothorax but a lower incidence of renal or cutaneous manifestations [48,49], but further assessment is still needed to demonstrate genetic, epidemiological, and clinical differences between Asian and White populations. Skin abnormalities of BHD are mainly manifested as fibrofolliculomas, trichodiscomas, acrochordons, angiofibromas, and intraoral lesions [45]. Fibrofolliculomas and trichodiscomas are benign tumors of perifollicular mesenchyme, which can appear as multiple small, dome-shaped, yellowish or skin-colored papules on the face, neck, scalp, and upper trunk [3]. Fibrofolliculomas occur in 82–92% of BHD-affected patients [50], and skin lesions were histologically confirmed as fibrofolliculomas in 1 of our cases. Multiple cutaneous fibrofolliculomas, at least 1 histologically confirmed, are considered as a major diagnostic criterion for the syndrome [2]. Different types of kidney neoplasms were found in BHD, including chromophobe/oncocytic hybrid, chromophobe, clear cell, oncocytoma, and papillary, and the most common form is a chromophobe–oncocytoma hybrid [51]. Kidney tumors are observed in about 30% of BHD-affected individuals, and occur at an average age of 50 years [6,20,44]. Older age and male sex are risk factors for renal tumor development in BHD [52]. Additionally, renal cysts also occur in BHD patients [18], and occasionally are the only renal manifestation [53]. About 45% of people with BHD have asymptomatic renal cystic changes without any clear symptoms [53]. Other findings, such as colon polyps or cancer, parotid oncocytomas, lipomas, thyroid nodules/cancer, and liver cysts, have been infrequently reported, but none of those are considered to be a clinical phenotype of BHD [21,45].
In clinical practice, BHD is easily underdiagnosed, or mistakenly diagnosed as pulmonary emphysema, LAM, pulmonary Langerhans cell histiocytosis, and other cystic lung diseases. The identification of skin lesions, especially fibrofolliculomas, should raise the suspicion of BHD and prompt further investigations to narrow the differential diagnosis [45]. For definitive diagnosis, biopsy of dermatological lesions, investigation of personal and family history of cutaneous lesions, spontaneous pneumothorax, lung cysts, renal neoplasia, and evaluation of genetic testing are important [45]. Confirmative diagnosis of BHD needs evidence of clinical manifestations and identification of
Clinical management of BHD aims at early recognition and the diagnosis and treatment of pneumothorax and kidney neoplasms. Currently, there is no specific therapy for BHD-related lung cysts. Treatment of pulmonary cysts is limited to prevention and management of pneumothorax, and management of BHD-related pneumothorax is similar to that of sporadic primary pneumothorax [2]. Pleurodesis is recommended after the first episode of spontaneous pneumothorax in BHD [46]. However, pleurodesis only reduced the rate of recurrent pneumothorax by half [54]. Both of our patients underwent pleurodesis, but it was only effective in preventing recurrent pneumothorax in 1 patient. BHD-affected patients should be discouraged from piloting aircraft and deep-sea diving, as exposure to large ambient pressure changes can induce pneumothorax [2]. There is no evidence that BHD-affected individuals should be advised against air travel unless they have an ongoing or recently treated pneumothorax [54,55]. Most BHD-associated renal tumors have a low malignant potential and a favorable prognosis. A delayed nephron-sparing strategy, which can preserve kidney function over time, is recommended in treatment of BHD-related renal cancers [50,56]. When surgery is not applicable, other techniques such as radiofrequency ablation and cryotherapy are alternative methods. It has been suggested that BHD-affected individuals are more vulnerable to cigarette smoke-induced pulmonary function impairment [57], and some evidence shows that smoking can increase the risk of pneumothorax and renal tumors in BHD; therefore, smoking cessation is encouraged in people with BHD [2]. BHD skin abnormalities do not need specific treatment, as they are basically benign. However, excision, debulking, laser ablation using fractional CO2 or erbium-YAG laser, or electrodessication can be applied for aesthetic reasons [2].
Conclusions
We report 2 Chinese cases of BHD syndrome and a previously unknown causative mutation of the
Figures
 Figure 1. Physical examination revealed dermatological lesionsMultiple dome-shaped papules were revealed on the nose, cheeks (A), neck (B), auricles (C), and the mucosal surface of the lower lip (D) of a 57-year-old Chinese woman. Dome-shaped papules were identified on the face (E) and neck (F) of a 58-year-old Chinese woman. (White arrow indicates the skin abnormalities).
Figure 1. Physical examination revealed dermatological lesionsMultiple dome-shaped papules were revealed on the nose, cheeks (A), neck (B), auricles (C), and the mucosal surface of the lower lip (D) of a 57-year-old Chinese woman. Dome-shaped papules were identified on the face (E) and neck (F) of a 58-year-old Chinese woman. (White arrow indicates the skin abnormalities). 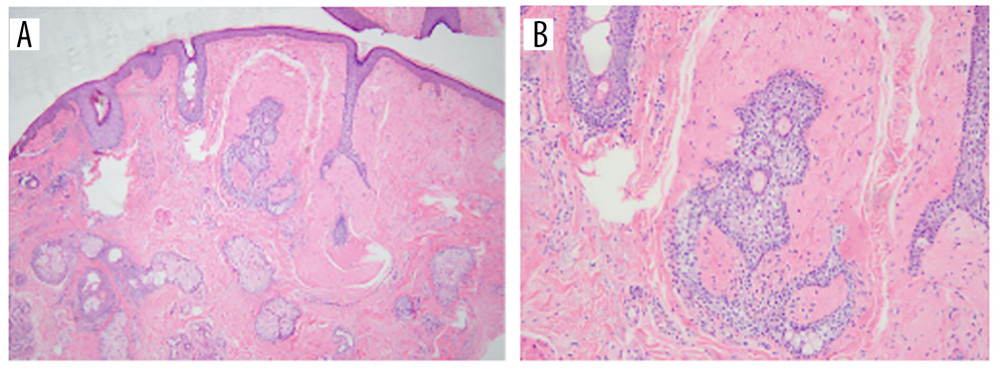 Figure 2. Skin lesions on the face of a 57-year-old Chinese woman were pathologically diagnosed as fibrofolliculomasThe epidermis is normal, and hyperplasia of fibrous connective tissue is visible in the dermis (A, B). (H&E staining, magnification ×40 in A, magnification ×100 in B).
Figure 2. Skin lesions on the face of a 57-year-old Chinese woman were pathologically diagnosed as fibrofolliculomasThe epidermis is normal, and hyperplasia of fibrous connective tissue is visible in the dermis (A, B). (H&E staining, magnification ×40 in A, magnification ×100 in B). 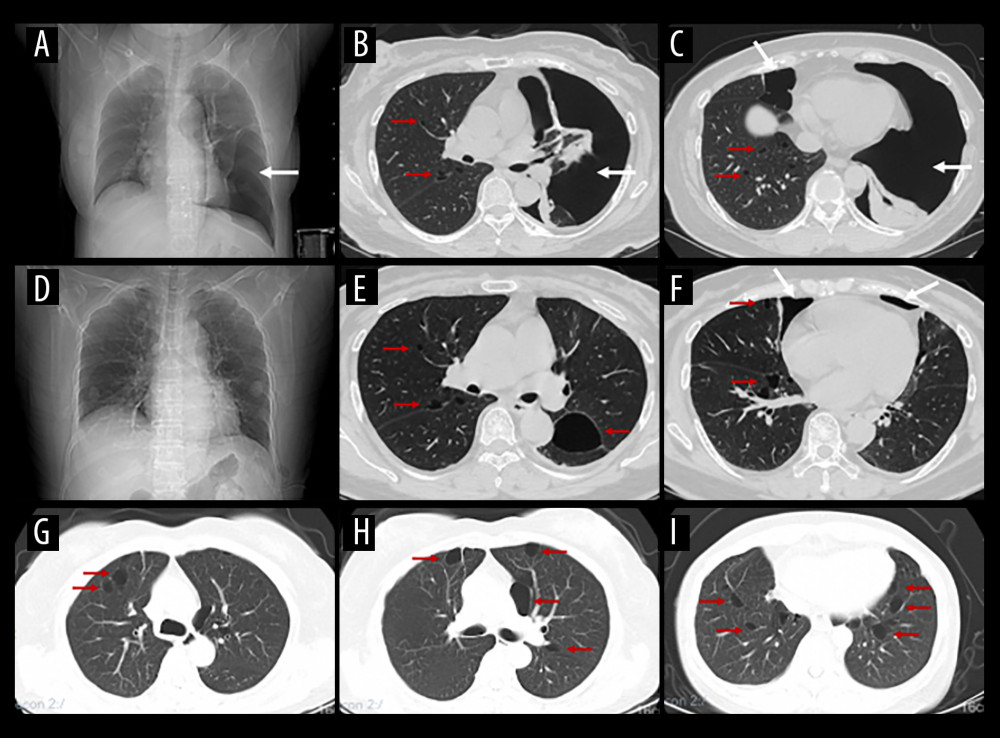 Figure 3. Chest imaging findings demonstrated the presence of multiple lung cysts with or without pulmonary pneumothoraxChest X-ray showed pneumothorax on the left side of the lung (A) and chest HRCT showed sparsely-distributed, thin-walled lung cysts in the lower lobes, with a large amount of pneumothorax at the left hemithorax and mild pneumothorax at the right hemithorax (B, C) of a 57-year-old Chinese woman, and subsequential chest X-ray (D) and chest HRCT performed after treatment of the pneumothorax (E, F). Chest HRCT demonstrated lung cysts in the subpleural (G, H) and basilar medial regions (I) of a 58-year-old Chinese woman. (White arrows indicate pulmonary pneumothorax, and red arrows indicate cystic lesions of the lungs).
Figure 3. Chest imaging findings demonstrated the presence of multiple lung cysts with or without pulmonary pneumothoraxChest X-ray showed pneumothorax on the left side of the lung (A) and chest HRCT showed sparsely-distributed, thin-walled lung cysts in the lower lobes, with a large amount of pneumothorax at the left hemithorax and mild pneumothorax at the right hemithorax (B, C) of a 57-year-old Chinese woman, and subsequential chest X-ray (D) and chest HRCT performed after treatment of the pneumothorax (E, F). Chest HRCT demonstrated lung cysts in the subpleural (G, H) and basilar medial regions (I) of a 58-year-old Chinese woman. (White arrows indicate pulmonary pneumothorax, and red arrows indicate cystic lesions of the lungs). 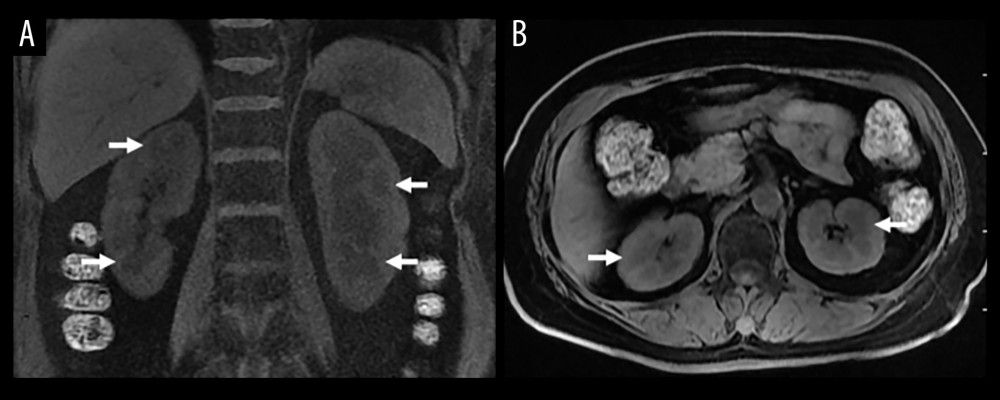 Figure 4. Renal MRI revealed multiple renal cysts of a 57-year-old Chinese womanMultiple kidney cysts were shown on the coronal scans (A), and transverse scans of renal MRI (B). (White arrows indicate kidney cysts).
Figure 4. Renal MRI revealed multiple renal cysts of a 57-year-old Chinese womanMultiple kidney cysts were shown on the coronal scans (A), and transverse scans of renal MRI (B). (White arrows indicate kidney cysts). 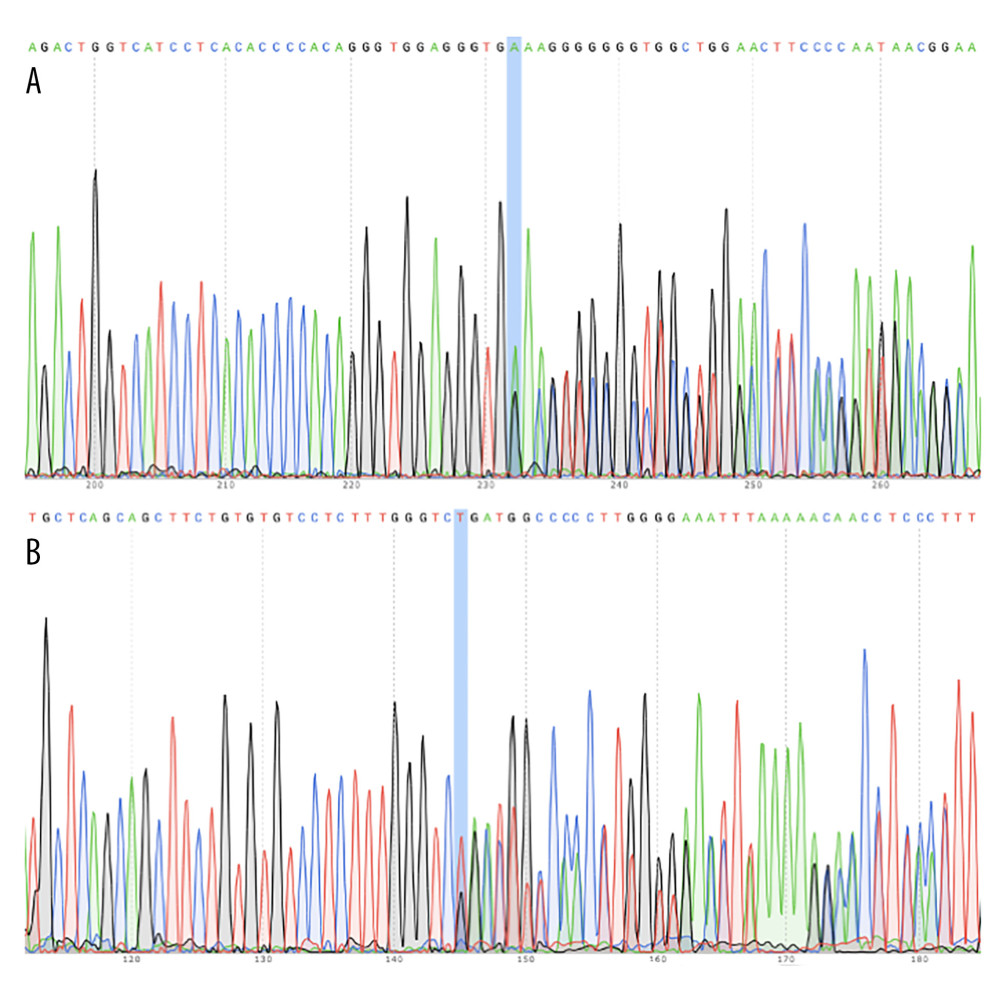 Figure 5. WES analysis identified mutation in FLCN geneWES revealed a novel mutation of FLCN gene in exon 12 of a 57-year-old Chinese woman (A). WES identified a mutation of FLCN gene in exon 14 of a 58-year-old Chinese woman (B).
Figure 5. WES analysis identified mutation in FLCN geneWES revealed a novel mutation of FLCN gene in exon 12 of a 57-year-old Chinese woman (A). WES identified a mutation of FLCN gene in exon 14 of a 58-year-old Chinese woman (B). References
1. Schulz T, Hartschuh W, Birt-Hogg-Dubé-syndrome and Hornstein-Knickenberg-syndrome are the same. Different sectioning technique as the cause of different histology: J Cutan Pathol, 1999; 26; 55-61
2. Menko FH, van Steensel MA, Giraud S, Birt-Hogg-Dubé syndrome: Diagnosis and management: Lancet Oncol, 2009; 10; 1199-206
3. Khoo SK, Bradley M, Wong FK, Birt-Hogg-Dubé syndrome: Mapping of a novel hereditary neoplasia gene to chromosome 17p12-q11.2: Oncogene, 2001; 20; 5239-42
4. Schmidt LS, Warren MB, Nickerson ML, Birt-Hogg-Dubé syndrome, a genodermatosis associated with spontaneous pneumothorax and kidney neoplasia, maps to chromosome 17p11.2: Am J Hum Genet, 2001; 69; 876-82
5. Nickerson ML, Warren MB, Toro JR, Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt-Hogg-Dubé syndrome: Cancer cell, 2002; 2; 157-64
6. Schmidt LS, Nickerson ML, Warren MB, Germline BHD-mutation spectrum and phenotype analysis of a large cohort of families with Birt-Hogg-Dubé syndrome: Am J Hum Genet, 2005; 76; 1023-33
7. Napolitano G, Di Malta C, Esposito A, A substrate-specific mTORC1 pathway underlies Birt-Hogg-Dubé syndrome: Nature, 2020; 585; 597-602
8. Baba M, Hong S-B, Sharma N, Folliculin encoded by the BHD gene interacts with a binding protein, FNIP1, and AMPK, and is involved in AMPK and mTOR signaling: Proc Natl Acad Sci, 2006; 103; 15552-57
9. van Steensel MAM, van Geel M, Badeloe S, Poblete-Gutiérrez P, Frank J, Molecular pathways involved in hair follicle tumor formation: All about mammalian target of rapamycin?: Exp Dermatol, 2009; 18; 185-91
10. Inoki K, Corradetti MN, Guan K-L, Dysregulation of the TSC-mTOR pathway in human disease: Nat Genet, 2005; 37; 19-24
11. Hancock E, Osborne J, Lymphangioleiomyomatosis: A review of the literature: Respir Med, 2002; 96(1); 1-6
12. Wei MH, Blake PW, Shevchenko J, Toro JR, The folliculin mutation database: An online database of mutations associated with Birt-Hogg-Dubé syndrome: Hum Mutat, 2009; 30; E880-E90
13. Lim DHK, Rehal PK, Nahorski MS, A new Locus-Specific Database (LSDB) for mutations in the folliculin (FLCN) gene: Hum Mutat, 2010; 31; E1043-E51
14. Hornstein OP, Kniekenberg M, Perifollicular fibromatosis cutis with polyps of the colon – a cutaneo-intestinal syndrome sui generis: Arch Dermatol Res, 1975; 253; 161-75
15. Muller ME, Daccord C, Taffé P, Lazor R, Prevalence of Birt-Hogg-Dubé syndrome determined through epidemiological data on spontaneous pneumothorax and bayes theorem: Front Med, 2021; 8; 631168
16. Park HJ, Kim YJ, Kim MJ, Kim HC, Epidemiology and clinical features of Birt-Hogg-Dubé syndrome: A nationwide population-based study in South Korea: PLoS One, 2022; 17; e0269358
17. Toro JR, Glenn G, Duray P, Birt-Hogg-Dubé syndrome a novel marker of kidney neoplasia: Arch Dermatol, 1999; 135; 1195-202
18. Furuya M, Yao M, Tanaka R, Genetic, epidemiologic and clinicopathologic studies of Japanese Asian patients with Birt-Hogg-Dubé syndrome: Clin Genet, 2016; 90; 403-12
19. Birt AR, Hogg GR, Dubé WJ, Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons: Arch Dermatol, 1977; 113; 1674-77
20. Leter EM, Koopmans AK, Gille JJP, Birt-Hogg-Dubé syndrome: Clinical and genetic studies of 20 families: J Invest Dermatol, 2008; 128; 45-49
21. Schmidt LS, Linehan WM, FLCN: The causative gene for Birt-Hogg-Dubé syndrome: Gene, 2018; 640; 28-42
22. Toro JR, Pautler SE, Stewart L, Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg-Dubé syndrome: Am J Respir Crit Care Med, 2007; 175; 1044-53
23. Nahorski MS, Lim DHK, Martin L, Investigation of the Birt-Hogg-Dubé tumour suppressor gene (FLCN) in familial and sporadic colorectal cancer: J Med Genet, 2010; 47; 385-90
24. Sattler EC, Syunyaeva Z, Mansmann U, Steinlein OK, Genetic risk factors for spontaneous pneumothorax in Birt-Hogg-Dubé syndrome: Chest, 2020; 157; 1199-206
25. Hasumi H, Baba M, Hong SB, Identification and characterization of a novel folliculin-interacting protein FNIP2: Gene, 2008; 415; 60-67
26. Towler MC, Hardie DG, AMP-activated protein kinase in metabolic control and insulin signaling: Circ Res, 2007; 100; 328-41
27. Shaw RJ, LKB1 and AMP-activated protein kinase control of mTOR signalling and growth: Acta Physiol (Oxf), 2009; 196; 65-80
28. Chen J, Futami K, Petillo D, Deficiency of FLCN in mouse kidney led to development of polycystic kidneys and renal neoplasia: PLoS One, 2008; 3; e3581
29. van Slegtenhorst M, Khabibullin D, Hartman TR, The Birt-Hogg-Dube and tuberous sclerosis complex homologs have opposing roles in amino acid homeostasis in Schizosaccharomyces pombe: J Biol Chem, 2007; 282; 24583-90
30. Hartman TR, Nicolas E, Klein-Szanto A, The role of the Birt-Hogg-Dubé protein in mTOR activation and renal tumorigenesis: Oncogene, 2009; 28; 1594-604
31. Hudon V, Sabourin S, Dydensborg AB, Renal tumour suppressor function of the BirteHoggeDubé syndrome gene product folliculin: J Med Genet, 2010; 47; 182-89
32. Baba M, Furihata M, Hong SB, Kidney-targeted Birt-Hogg-Dubé gene inactivation in a mouse model: Erk1/2 and Akt-mTOR activation, cell hyperproliferation, and polycystic kidneys: J Natl Cancer Inst, 2008; 100; 140-54
33. Hasumi Y, Baba M, Ajima R, Homozygous loss of BHD causes early embryonic lethality and kidney tumor development with activation of mTORC1 and mTORC2: Proc Natl Acad Sci, 2009; 106; 18722-27
34. Hong SB, Oh H, Valera VA, Inactivation of the FLCN tumor suppressor gene induces TFE3 transcriptional activity by increasing its nuclear localization: PLoS One, 2010; 5; e15793
35. Park H, Staehling K, Tsang M: Immunity, 2012; 36; 769-81
36. Cash TP, Gruber JJ, Hartman TR, Loss of the Birt-Hogg-Dubé tumor suppressor results in apoptotic resistance due to aberrant TGFβ-mediated transcription: Oncogene, 2011; 30; 2534-46
37. Hong S-B, Oh H, Valera VA, Tumor suppressor FLCN inhibits tumorigenesis of a FLCN-null renal cancer cell line and regulates expression of key molecules in TGF-β signaling: Mol Cancer, 2010; 9; 160
38. Petit CS, Roczniak-Ferguson A, Ferguson SM, Recruitment of folliculin to lysosomes supports the amino acid-dependent activation of rag gtpases: J Cell Biol, 2013; 202; 1107-22
39. Tsun ZY, Bar-Peled L, Chantranupong L, The folliculin tumor suppressor is a GAP for the RagC/D GTPases that signal amino acid levels to mTORC1: Mol Cell, 2013; 52; 495-505
40. Possik E, Jalali Z, Nouët Y, Folliculin regulates Ampk-dependent autophagy and metabolic stress survival: PLoS Genet, 2014; 10; e1004273
41. Dunlop EA, Seifan S, Claessens T, FLCN, a novel autophagy component, interacts with GABARAP and is regulated by ULK1 phosphorylation: Autophagy, 2014; 10; 1749-60
42. Nahorski MS, Seabra L, Straatman-Iwanowska A, Folliculin interacts with p0071 (plakophilin-4) and deficiency is associated with disordered rhoa signalling, epithelial polarization and cytokinesis: Hum Mol Genet, 2012; 21; 5268-79
43. Medvetz DA, Khabibullin D, Hariharan V, Folliculin, the product of the Birt-Hogg-Dube tumor suppressor gene, interacts with the adherens junction protein p0071 to regulate cell-cell adhesion: PLoS One, 2012; 7; e47842
44. Zbar B, Alvord WG, Glenn G, Risk of renal and colonic neoplasms and spontaneous pneumothorax in the Birt-Hogg-Dubé syndrome: Cancer Epidemiol Biomark Prev, 2002; 11; 393-400
45. Daccord C, Good JM, Morren MA, Birt-Hogg-Dubé syndrome: Eur Respir Rev, 2020; 29; 200042
46. Gupta N, Seyama K, McCormack FX, Pulmonary manifestations of Birt-Hogg-Dubé syndrome: Fam Cancer, 2013; 12; 387-96
47. Houweling AC, Gijezen LM, Jonker MA: Br J Cancer, 2011; 105; 1912-19
48. Guo T, Shen Q, Ouyang R, The clinical characteristics of East Asian patients with Birt-Hogg-Dubé syndrome: Ann Transl Med, 2020; 8; 1436
49. Hu X, Zhang G, Chen X, Xu KF, Birt-Hogg-Dubé syndrome in Chinese patients: A literature review of 120 families: Orphanet J Rare Dis, 2021; 16; 101
50. Schmidt LS, Marston Linehan W, Clinical features, genetics and potential therapeutic approaches for Birt-Hogg-Dubé syndrome: Expert Opin Orphan Drugs, 2015; 3; 15-29
51. Pavlovich CP, Walther MM, Eyler RA, Renal tumors in the Birt-Hogg-Dubé syndrome: Am J Surg Pathol, 2002; 26; 1542-52
52. Kijlertsuphasri S, Petnak T, Moua T, Diagnosis of renal tumors in Birt-Hogg-Dube syndrome: Clinical presentation and risk factors in a single-center retrospective cohort: BMC Nephrol, 2024; 25(1); 329
53. Kluger N, Giraud S, Coupier I, Birt-Hogg-Dubé syndrome: Clinical and genetic studies of 10 French families: Br J Dermatol, 2010; 162; 527-37
54. Gupta N, Kopras EJ, Henske EP, Spontaneous pneumothoraces in patients with Birt-Hogg-Dubé syndrome: Ann Am Thorac Soc, 2017; 14; 706-13
55. Johannesma PC, van de Beek I, van der Wel JWT, Risk of spontaneous pneumothorax due to air travel and diving in patients with Birt-Hogg-Dubé syndrome: Springerplus, 2016; 5; 1506
56. Stamatakis L, Metwalli AR, Middelton LA, Marston Linehan W, Diagnosis and management of BHD-associated kidney cancer: Fam Cancer, 2013; 12; 397-402
57. Uemasu K, Nyunoya T, A case report of Birt-Hogg-Dubé syndrome associated with severe airway obstruction in a 62-year-old female smoker: Respirol Case Rep, 2024; 12(3); e01327
Figures
Figure 1. Physical examination revealed dermatological lesionsMultiple dome-shaped papules were revealed on the nose, cheeks (A), neck (B), auricles (C), and the mucosal surface of the lower lip (D) of a 57-year-old Chinese woman. Dome-shaped papules were identified on the face (E) and neck (F) of a 58-year-old Chinese woman. (White arrow indicates the skin abnormalities).Figure 2. Skin lesions on the face of a 57-year-old Chinese woman were pathologically diagnosed as fibrofolliculomasThe epidermis is normal, and hyperplasia of fibrous connective tissue is visible in the dermis (A, B). (H&E staining, magnification ×40 in A, magnification ×100 in B).Figure 3. Chest imaging findings demonstrated the presence of multiple lung cysts with or without pulmonary pneumothoraxChest X-ray showed pneumothorax on the left side of the lung (A) and chest HRCT showed sparsely-distributed, thin-walled lung cysts in the lower lobes, with a large amount of pneumothorax at the left hemithorax and mild pneumothorax at the right hemithorax (B, C) of a 57-year-old Chinese woman, and subsequential chest X-ray (D) and chest HRCT performed after treatment of the pneumothorax (E, F). Chest HRCT demonstrated lung cysts in the subpleural (G, H) and basilar medial regions (I) of a 58-year-old Chinese woman. (White arrows indicate pulmonary pneumothorax, and red arrows indicate cystic lesions of the lungs).Figure 4. Renal MRI revealed multiple renal cysts of a 57-year-old Chinese womanMultiple kidney cysts were shown on the coronal scans (A), and transverse scans of renal MRI (B). (White arrows indicate kidney cysts).Figure 5. WES analysis identified mutation in FLCN geneWES revealed a novel mutation of FLCN gene in exon 12 of a 57-year-old Chinese woman (A). WES identified a mutation of FLCN gene in exon 14 of a 58-year-old Chinese woman (B). In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133