19 June 2025: Articles 
Fatal Progression of Vulvar Cancer in Pregnancy: A Case Report on Delayed Intervention
Unusual clinical course, Unusual setting of medical care
Kartika Hapsari ABCDEFG 1,2, Alfonsus Zeus Suryawan ABCDEFG 1*, Ali Budi Harsono CDEF 1, Gatot Nyarumenteng A. Winarno DEF 1, Hermin Aminah Usman BD 3DOI: 10.12659/AJCR.947567
Am J Case Rep 2025; 26:e947567






Abstract
BACKGROUND: Vulvar cancer (VC) in pregnancy is a rare case, and its incidence is unknown until now. This case report highlights the rapid progression of disease 3 months after delivery, and our limitation in low resource setting.
CASE REPORT: A pregnant woman in her early 40’s presented with a left vulvar lesion. The lesion was 7×5 cm, with clitoris involvement. No infiltration to adjacent organs was present. Her biopsy showed well-differentiated squamous cell vulva carcinoma. After C-section delivery at 34 weeks of gestation, the diagnosis remained FIGO stage IB (T1b N0 M0). MRI and radical vulvectomy were planned immediately, but due to National Health Insurance limitations the procedure was performed 3 months later. After evaluation 3 months later, the clinical diagnosis had progressed to advanced-stage vulva carcinoma. This case report highlights rapid progression of VC in pregnancy and 3 months after delivery. The possibility of rapid progression of VC during the postpartum period should not be overlooked, and timely treatment of VC in pregnancy is essential to ensure better outcomes.
CONCLUSIONS: Gynecologists should not overlook the possibility of rapid progression of VC after delivery due to several factors, such as immunologic and physiological changes during the puerperium phase. The operation should be carried out as soon as possible, but could be delayed after delivery, considering inguinal lymphadenectomy is an integral part of frozen section surgical staging.
Keywords: Pregnancy, Vulva, Vulvar Neoplasms, Humans, Female, Pregnancy Complications, Neoplastic, Disease Progression, Carcinoma, Squamous Cell, adult, Fatal Outcome
Introduction
Vulvar cancer (VC) in pregnancy is rare, and its incidence is unknown. Between 1955 and 2014, only 36 case reports were reported worldwide [1]. Underreporting may be a contributing factor to the unknown incidence of vulvar cancer in pregnancy. Currently, there is no clear guideline for managing VC in pregnancy due to its rarity. Winarno et al reported 5 cases of vulvar cancer in pregnancy, which were treated by surgical resection and simultaneous sentinel lymph node biopsy (SLNB), suggesting that surgical treatment in pregnancy complicated with VC is safe during pregnancy [2].
VC treatment in pregnancy should never be delayed, as delayed diagnosis can lead to tumor upstaging, but surgery in the third trimester may entail imminent surgery or be delayed until after delivery [3,4]. A literature review by Palicelli showed similar outcomes from 10 patients with VC in pregnancy who underwent radical vulvectomy during pregnancy and 12 who underwent surgery after delivery [4].
This case report highlights the rapid progression of disease 3 months after delivery in a low-resource setting.
Case Report
INVESTIGATIONS:
Physical examination revealed a 7×5 cm exophytic mass at the left labia majora with clitoris involvement. Margins were 3 cm from the vagina, 2 cm from the urethra, and 3 cm from the anal sphincter (Figure 1). No inguinal lymphatic enlargement was present. Abdominal ultrasound revealed pregnancy at 31–32 weeks, with estimated fetal weight of 1779 grams and oligohydramnios. Vulva biopsy revealed the mass was well-differentiated squamous cell carcinoma, not otherwise specified, on the vulva. p16 staining was done afterward and gave negative result, showing no human papilloma virus (HPV) involvement (Figure 2).
DIFFERENTIAL DIAGNOSIS:
Staging for vulvar cancer follows the latest International Federation of Gynecology and Obstetrics (FIGO) guideline [5]. According to the American Joint Committee on Cancer (AJCC) Tumor-Node-Metastases and FIGO guidelines, our patient was stage IB with T1b, which means the lession was more than 2 cm (7×5 cm) in size and still confined to the vulva and perineum. Because the tumor did not extend to the lower third of the urethra and vagina, and due to lack of anal involvement, we did not classify our patient as stage II [5,6]. The working diagnosis was G5P4A0 31–32 weeks of pregnancy with vulva cancer FIGO stage IB (T1b N0 M0). We also performed abdominal ultrasound, which showed no enlargement of inguinal, hypogastric, parametrium, and paraaortic lymphatic nodes. However, pelvic MRI could not be performed at that time due National Health Insurance limitations.
TREATMENT:
Patient was planned for cesarean section at 34–35 weeks of pregnancy considering fetal weight and lung maturation. A cesarean section was performed after 1 month of observation, and a healthy male baby was born weighing 2270 g and the New Ballard Score (NBS) was 35 weeks. MRI and radical vulvectomy were planned to be performed immediately after the cesarian section, but National Health Insurance did not provide coverage for simultaneous procedures. The patient was then planned for procedures 3 months afterward, with routine monitoring at our Obstetrics and Oncology Policlinic.
OUTCOME AND FOLLOW UP:
Three months later, without prior routine control before, the patient was contacted for evaluation and surgical planning at the Gynecology-Oncology Policlinic. However, she presented with mass enlargement to 8×8 cm with clitoris involvement and infiltration to the vagina, urethra, and anorectal tissue, as well as left inguinal enlargement (Figure 3).
Pelvic MRI revealed a solid mass in the left vulva with invasion of vulvar stroma, pubic part, and labia major and minor, one-third of the distal urethra had been infiltrated, and left pelvic nodes were already involved (Figure 4). The working diagnosis became vulva carcinoma FIGO stage IVA. Due to the progression of the disease, vulvectomy was no longer possible, and she received concurrent chemoradiotherapy (CCRT) in a palliative care setting.
Discussion
The diagnosis of vulvar cancer in this case was considered early, but due to patient-related delay and National Health Insurance limitations, intervention was delayed. Due to its rarity, the outcomes and optimal management of pregnancy complicated by vulvar cancer remain understudied. A previous study reported that 42.6% of patients with vulvar cancer underwent cesarean section [1]. While vulvar cancer may be asymptomatic, most women present earlier with vulvar pruritus or pain or have noticed a lump or ulcer [5]. However, our patient did not realize the small lump was a cancerous mass, which led to a delayed diagnosis when the patient came at 30 weeks of pregnancy with an enlarged vulvar mass categorized as early vulvar cancer [5]. To increase the survival rate of the mother, definitive treatment should not be delayed. Our patient presented in the third trimester, and surgical intervention could be performed after delivery [2,4]. We planned for vulvectomy immediately after delivery, but the National Health Insurance limitations delayed surgery by 3 months.
After the patient-related delay, she showed swift progression of disease in the postpartum period until definitive treatment could be started. Pregnancy and early postpartum are periods in which the immune system tends to be more humoral and accompanied by possible suppression of cellular immunity. Groer et al reported that cytotoxic T lymphocytes, known for eliminating tumor target cells in an antigen and cell-contact-dependent manner, also decrease in pregnancy and the postpartum period [7]. The rich vasculature of the pelvic area, especially during pregnancy and early postpartum, followed by secretion of sex and growth hormones, also favor cancer progression [4].
Vulvar cancer tends to grow slowly and progress over a period of years, but in this case, at the time of diagnosis the stadium was 1B, which rapidly progressed to stage 4A in only 3 months during the postpartum period. The postpartum period is the time period after delivery, when maternal physiological and anatomy returns to the nonpregnant state, which occurs 6 weeks to 6 months after delivery [8]. In this period, cellular immunity, as measured by cytokine production, does not return to pre-pregnancy levels until the first 3–4 months postpartum [7]. Cytotoxic T lymphocytes are known for eliminating tumor target cells in an antigen- and cell-contact-dependent manner and decrease in pregnancy and the postpartum period. This hypothetically could have contributed to the rapid progression of VC in our patient.
For those patients whose vulval surgery is delayed until the post-natal period, there is no clear guidance regarding the timing of such surgery [3]. Most reports and analyses state that the operation must be performed after the diagnosis, but some exception exist. As early-stage VC is a relatively slow-growing tumor, treatment can be safely deferred until after labor if diagnosed at the third trimester [2]. Primary treatment for early VC is surgical resection, which is associated with good prognosis [9]. As our patient was 1B but with a relatively bigger mass, at 7×5 cm, inguinofemoral lymphadenectomy should be performed along with mass resection [5,9]. Panici et al assessed the prognosis of patients with VC that undergoes unilateral or bilateral inguinal lymphadenectomy, finding that lymphadenectomy is not associated with more postsurgical complications [10]. Inguinal lymphadenectomy is an integral part of VC surgical staging, as undiagnosed inguinal node metastases are often fatal [11]. However, during pregnancy, groin lymphadenectomy would likely result in bilateral leg lymphoedema and inguinal seroma due to poor venous return [3,12]. Physiological changes occurring during pregnancy also create a heavier circulatory burden, which can increase maternal morbidity due to patient immobility. Gaunt et al stated that staging surgery for inguinal lymphatics should be delayed at least until 6 weeks postnatally unless there is clear evidence of inguinal node metastasis on clinical and cross-sectional imaging assessment [12]. We ruled out lymphatic nodes involvement at the time of diagnosis with ultrasonography, which showed no inguinal or other lymphatic enlargement. However, MRI was not available during pregnancy due to National Health Insurance coverage limitations, and could only be performed later, after delivery.
Our patient’s nutritional status before pregnancy was poor and she was considerably underweight (IMT <18 kg/m2), which indicates malnourishment, in which energy quotas cannot be met, which also could have contributed to a declining immune system [13]. HPV infection is a significant factor in disease progression. HPV involvement can be detected with p16 IHC testing, as p16 itself is an indirect marker of HPV involvement due to its overexpression caused by the viral E7 protein [14]. Unfortunately, p16 IHC staining was negative, which indicated our patient did not have HPV infection.
In the present case, delayed presentation and National Health Insurance coverage were the main reasons for the disease progression. However, her immune system and nutrition status could also have contributed to the rapid disease progression. Compared to previous research suggestions, in this case therapy was delayed until 9 weeks after delivery, without proper imaging and further staging workups.
Alternatively, we could have performed early radical vulvectomy during pregnancy and cesarean section later, at 34 weeks of pregnancy. Although inguinal lymphadenectomy increases the risk of morbidity, it is well justified considering the risk of mass progression, which hinders optimal treatment. Therapy was then followed by external beam radiation therapy (EBRT) and concurrent chemotherapy after birth. A multidisciplinary team (MDT) approach is mandatory in all cases of malignancy in pregnancy. In the present case, there was a joint conference with Oncology Gynecology, the Fetomaternal Division, and the perinatologist before we determined the course of therapy.
Conclusions
Gynecologists should not overlook the possibility of rapid progression of VC after delivery, due to several factors, such as immunologic and physiological changes during the puerperium phase. Surgery should be performed as soon as possible because it safe to conduct during pregnancy but can be delayed after delivery if diagnosed in the third trimester, considering inguinal lymphadenectomy is an integral part of frozen section surgical staging. Delaying the surgery is not an option even during pregnancy; however, staging for inguinal metastases can be conducted postnatally considering the adverse effect is greater than the benefit if conducted during pregnancy.
Figures
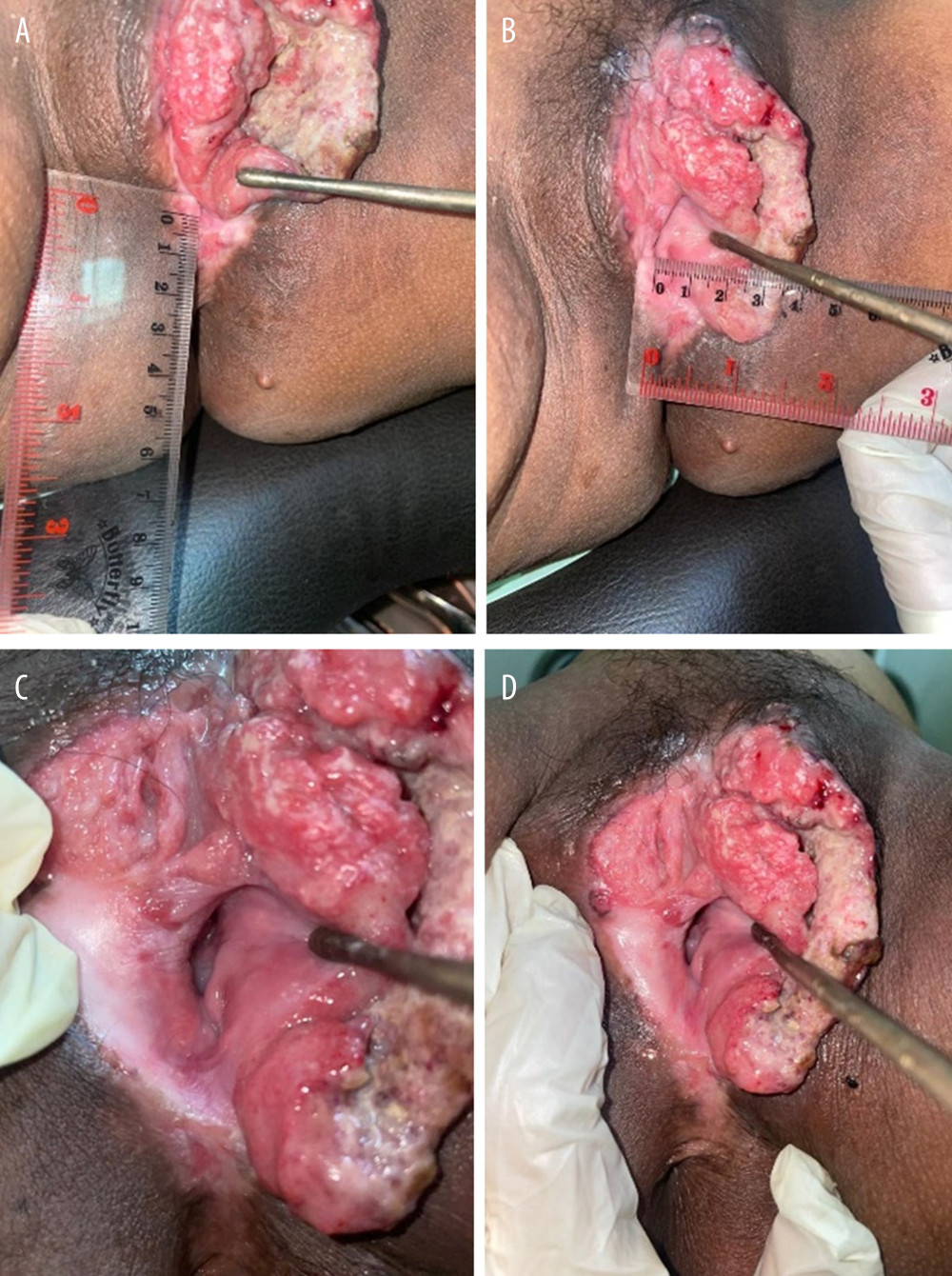 Figure 1. Vulvar mass at 30 weeks of pregnancy, (A) No infiltration to anorectal tissue; (B) 3 cm margin from vagina; (C, D) exophytic mass at left labia with clitoris involvement.
Figure 1. Vulvar mass at 30 weeks of pregnancy, (A) No infiltration to anorectal tissue; (B) 3 cm margin from vagina; (C, D) exophytic mass at left labia with clitoris involvement. 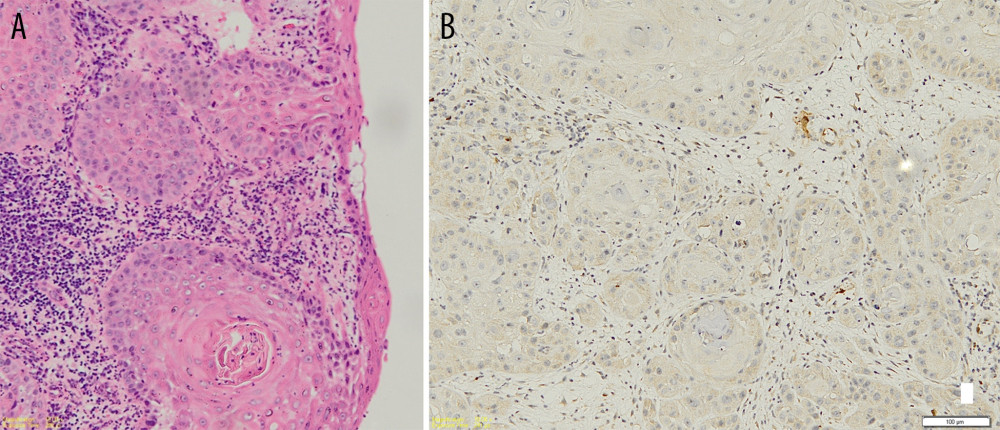 Figure 2. Histopathology and p16 immunohistology examination, (A) 100× enlargement shows keratin pearl formations alongside hyperplastic, hyperchromatic, and mitotic cell on vulval mass. (B) p16 Staining shows negative results.
Figure 2. Histopathology and p16 immunohistology examination, (A) 100× enlargement shows keratin pearl formations alongside hyperplastic, hyperchromatic, and mitotic cell on vulval mass. (B) p16 Staining shows negative results. 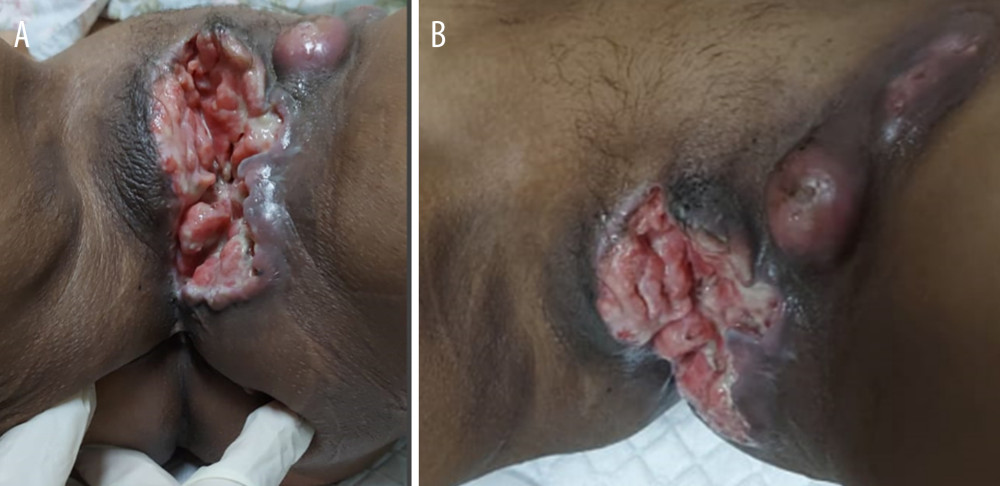 Figure 3. Vulvar mass at 3 months postpartum. (A) Mass infiltrated to vagina, 1/3 upper urethra, and anorectal tissue. (B) Inguinal enlargement and ulcerated node.
Figure 3. Vulvar mass at 3 months postpartum. (A) Mass infiltrated to vagina, 1/3 upper urethra, and anorectal tissue. (B) Inguinal enlargement and ulcerated node. 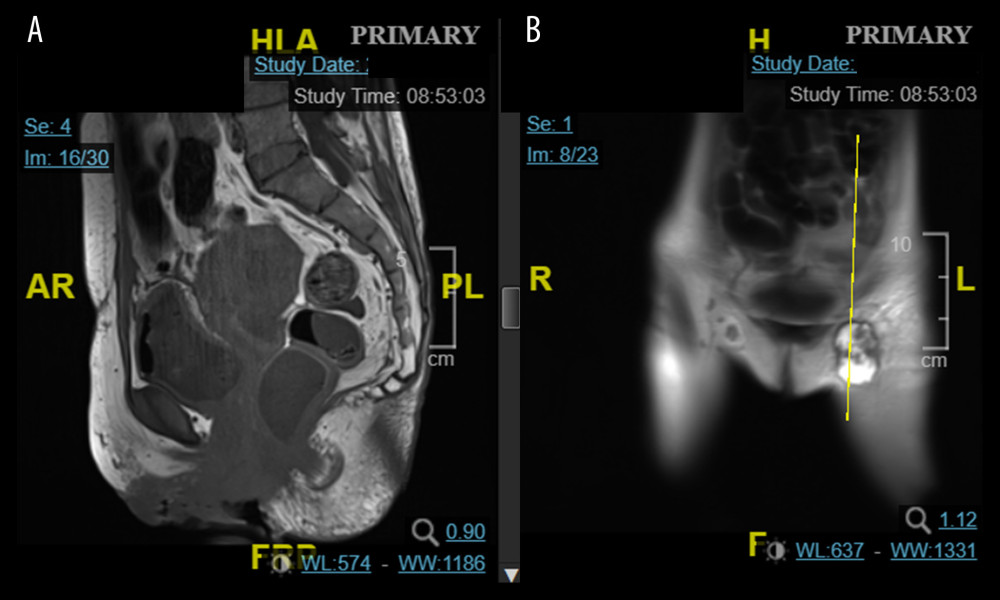 Figure 4. Pelvic MRI at 3 months postpartum. (A) Tumor shows infiltration of stroma; pubic part; and labia. (B) Metastatic nodule in left inguinal node.
Figure 4. Pelvic MRI at 3 months postpartum. (A) Tumor shows infiltration of stroma; pubic part; and labia. (B) Metastatic nodule in left inguinal node. References
1. Matsuo K, Whitman SA, Blake EA, Feto-maternal outcome of pregnancy complicated by vulvar cancer: A systematic review of literature: Eur J Obstet Gynecol Reprod Biol, 2014; 179; 216-23
2. Winarno AS, Fehm TN, Hampl M, Vulvar cancer during pregnancy and/or breastfeeding: A report of five cases from a single center study at the University Hospital of Düsseldorf: BMC Pregnancy Childbirth, 2022; 22(1); 207
3. Amant F, Berveiller P, Boere IA, Gynecologic cancers in pregnancy: Guidelines based on a third international consensus meeting: Ann Oncol, 2019; 30(10); 1601-12
4. Palicelli A, Giaccherini L, Zanelli M, How can we treat vulvar carcinoma in pregnancy? A systematic review of the literature: Cancers (Basel), 2021; 13(4); 836
5. Olawaiye AB, Cuello MA, Rogers LJ, Cancer of the vulva: 2021 update: Int J Gynecol Obstet, 2021; 155(S1); 7-18
6. Abu-Rustum NR, Yashar CM, Arend R, Vulvar cancer, Version 3.2024, NCCN clinical practice guidelines in oncology: J Natl Compr Canc Netw, 2024; 22(2); 117-35
7. Groer ME, Jevitt C, Ji M, Immune changes and dysphoric moods across the postpartum: Am J Reprod Immunol, 2015; 73(3); 193-98
8. Romano M, Cacciatore A, Giordano R, La Rosa B, Postpartum period: Three distinct but continuous phases: J Prenat Med, 2010; 4(2); 22-25
9. Giannini A, D’Oria O, Chiofalo B, The giant steps in surgical downsizing toward a personalized treatment of vulvar cancer: J Obstet Gynaecol Res, 2022; 48(3); 533-40
10. Panici PB, Tomao F, Domenici L, Prognostic role of inguinal lymphadenectomy in vulvar squamous carcinoma: Younger and older patients should be equally treated. A prospective study and literature review: Gynecol Oncol, 2015; 137(3); 373-79
11. Ignacio Z, Sara I, Pluvio JC, Prognostic factors in patients with vulvar cancer: The VULCAN study: Int J Gynecol Cancer, 2020; 30(9); 1285-91
12. Gaunt E, Pounds R, Yap J, Vulval cancer in pregnancy: Two case reports: Case Rep Womens Health, 2022; 33; e00374
13. Bourke CD, Berkley JA, Prendergast AJ, Immune dysfunction as a cause and consequence of malnutrition: Trends Immunol, 2016; 37(6); 386-98
14. Geißler C, Tahtali A, Diensthuber M, The role of p16 expression as a predictive marker in HPV-positive oral SCCHN – a retrospective single-center study: Anticancer Res, 2013; 33(3); 913-16
Figures
Figure 1. Vulvar mass at 30 weeks of pregnancy, (A) No infiltration to anorectal tissue; (B) 3 cm margin from vagina; (C, D) exophytic mass at left labia with clitoris involvement.Figure 2. Histopathology and p16 immunohistology examination, (A) 100× enlargement shows keratin pearl formations alongside hyperplastic, hyperchromatic, and mitotic cell on vulval mass. (B) p16 Staining shows negative results.Figure 3. Vulvar mass at 3 months postpartum. (A) Mass infiltrated to vagina, 1/3 upper urethra, and anorectal tissue. (B) Inguinal enlargement and ulcerated node.Figure 4. Pelvic MRI at 3 months postpartum. (A) Tumor shows infiltration of stroma; pubic part; and labia. (B) Metastatic nodule in left inguinal node. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953068
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133