22 June 2025: Articles 
Managing Pyeloureteral Atresia in Pediatrics: A Case of Right-Sided Hydronephrosis and Surgical Intervention
Rare disease
Shaden S. AlMousa ABCDEFG 1*DOI: 10.12659/AJCR.947597
Am J Case Rep 2025; 26:e947597






Abstract
BACKGROUND: Pyeloureteral atresia is a rare congenital anomaly characterized by complete obstruction of the ureteropelvic junction, leading to severe hydronephrosis and potential renal damage. Early diagnosis and surgical intervention are essential to preserve renal function and prevent long-term complications.
CASE REPORT: A 3-year-old boy presented with a 3-day history of worsening abdominal pain, nausea, and vomiting. Physical examination revealed abdominal tenderness, primarily in the right lower quadrant. Notably, there were no genitourinary symptoms such as dysuria, hematuria, or changes in urinary frequency. Laboratory tests indicated mild leukocytosis and elevated serum creatinine, suggesting impaired renal function. Abdominal ultrasound revealed massive right-sided hydronephrosis, which was further evaluated by contrast-enhanced CT, confirming an atretic segment at the ureteropelvic junction consistent with pyeloureteral atresia. The child underwent right-sided pyeloplasty, involving resection of the atretic segment and reconstruction of the ureteropelvic junction to restore urinary flow. Recovery was smooth, with renal function normalizing within 1 week. A follow-up ultrasound at 2 weeks after surgery confirmed the resolution of hydronephrosis. He was scheduled for regular follow-ups to monitor renal health.
CONCLUSIONS: This case shows the importance of early recognition and management of pyeloureteral atresia in pediatric patients. Comprehensive imaging, detailed surgical intervention, and timely management can optimize outcomes, preserving renal function and ensuring long-term health. Continued awareness and research are necessary to improve diagnosis and treatment strategies for this rare congenital anomaly.
Keywords: Hydronephrosis, Nephrectomy, Tomography, Ureteral Obstruction, Humans, Male, Child, Preschool, Ureter, Kidney Pelvis
Introduction
Pyeloureteral atresia is a rare congenital anomaly characterized by complete obstruction of the ureteropelvic junction, leading to severe hydronephrosis and potential renal impairment [1]. This condition arises from abnormal embryological development of the ureteric bud and metanephric blastema interaction during the fifth to seventh weeks of gestation, resulting in a complete blockage of urine flow from the renal pelvis to the bladder. The estimated prevalence is less than 1 in 10 000 live births, making it a significant but uncommon cause of obstructive uropathy in pediatric populations [2]. The obstruction often manifests in early infancy or childhood, presenting with symptoms such as abdominal pain, flank pain, and signs of renal dysfunction [1,2].
Early diagnosis is crucial, as the condition can lead to progressive renal damage if left untreated [2]. Imaging modalities such as ultrasound and computed tomography (CT) play a pivotal role in the diagnosis, revealing the extent of hydronephrosis and the atretic segment of the ureter. Treatment typically involves surgical intervention to relieve the obstruction and restore normal urinary flow. Prompt surgical management is essential to preserve renal function and prevent long-term complications [3].
This case report describes a 3-year-old boy who presented with abdominal pain and was found to have massive right-sided hydronephrosis secondary to pyeloureteral atresia. The report emphasizes the importance of early diagnosis and timely surgical intervention in managing this rare condition, aiming to contribute to the limited literature on pyeloureteral atresia and improve understanding of its management strategies.
Case Report
A 3-year-old boy was brought to the pediatric emergency department with a 3-day history of worsening abdominal pain. The pain was initially described as intermittent but had become constant and severe. His mother reported he had associated symptoms of nausea and vomiting, with no recent changes in bowel habits. Importantly, there were no genitourinary symptoms such as dysuria, hematuria, increased urinary frequency, urgency, or decreased urine output.
He had been generally healthy, with no significant past medical or surgical history and no known drug allergies. There was no history of trauma, recent infections, or significant family medical history.
On physical examination, he appeared to be in moderate distress. His vital signs were stable, with a temperature of 37.0°C, heart rate of 115 beats per minute, respiratory rate of 22 breaths per minute, and blood pressure of 100/65 mmHg. The abdominal examination revealed diffuse tenderness, most pronounced in the right lower quadrant. There was no rebound tenderness or guarding, and bowel sounds were normal. The rest of the physical examination, including the assessment of other systems, was unremarkable.
Given the clinical presentation, a work-up was initiated. Laboratory investigations included a complete blood count (CBC), serum electrolytes, renal function tests, and urinalysis. The CBC showed a white blood cell count of 12 000/μL, indicating mild leukocytosis. Renal function tests revealed an elevated serum creatinine level of 1.2 mg/dL (normal range for age: 0.2–0.5 mg/dL), suggestive of impaired renal function. Electrolytes were within normal limits, and urinalysis showed no significant abnormalities.
The initial differential diagnosis for this presentation included acute appendicitis, which was less likely given the absence of localized tenderness or rebound tenderness; intussusception, which was considered due to the child’s age but was excluded by imaging; and other causes of obstructive uropathy, such as ureteral stricture or valve obstruction.
To further investigate the cause of the abdominal pain and renal impairment, an abdominal ultrasound was performed. The ultrasound findings were significant for massive right-sided hydronephrosis with an antral diameter of 40 mm. No obstruction at the level of the ureter was observed on ultrasound, which, combined with the extent of hydronephrosis, raised suspicion for a congenital obstruction such as pyeloureteral atresia rather than ureteropelvic junction obstruction (UPJO) (Figure 1).
A contrast-enhanced CT scan of the abdomen and pelvis was subsequently performed. The CT scan confirmed the presence of massive right-sided hydronephrosis and revealed a markedly dilated right renal pelvis and ureter with a narrow, atretic segment noted just below the renal pelvis (Figure 2). These findings were highly suggestive of pyeloureteral atresia, as the abrupt transition from a dilated renal pelvis to a narrow segment is more characteristic of atresia than UPJO, which typically presents with a tapering transition.
In the acute setting, a renal scan (eg, MAG3 or DMSA) was not performed due to the urgency of the clinical situation, impaired renal function, and the need for prompt surgical intervention. The imaging findings were sufficient to guide surgical planning, and a functional scan was deferred to the postoperative follow-up period once renal function had stabilized.
Intraoperatively, a narrow, non-canalized segment of the ureter was observed just below the renal pelvis, confirming the diagnosis of pyeloureteral atresia. This absence of a patent lumen strongly differentiated the condition from UPJO, which usually involves a partially obstructed but patent ureter. The gross appearance of the atretic segment was consistent with congenital atresia rather than an acquired stricture or inflammation.
The child was admitted to the pediatric surgery department, and a urologic consultation was obtained. The child underwent a right-sided pyeloplasty, which involved resection of the atretic segment and reconstruction of the ureteropelvic junction to restore urinary flow. The procedure was completed without complications, and he was transferred to the pediatric postoperative unit for recovery.
The hospital course was generally uneventful. Postoperatively, he was monitored for signs of infection, pain management, and renal function. Renal function improved significantly, with serum creatinine levels returning to within normal limits. He tolerated oral intake and resumed normal bowel and urinary function.
Upon discharge, he was scheduled for regular follow-up visits to monitor renal function and ensure continued resolution of the hydronephrosis (Figure 3). Regular urologic evaluations were advised to monitor renal health and prevent potential long-term complications.
Discussion
Pyeloureteral atresia is an exceptionally uncommon condition, often diagnosed in infancy or early childhood due to its severe clinical manifestations. Its prevalence is estimated to be less than 1 in 10 000 live births, making it a rare but important cause of obstructive uropathy in pediatric populations [3]. The complete obstruction at the ureteropelvic junction results in significant hydronephrosis and can lead to progressive renal damage if not promptly addressed.
In pediatric patients with hydronephrosis, more common differentials such as ureteropelvic junction obstruction, ureteral stricture, or congenital ureteral valves must be considered. Ureteropelvic junction obstruction, in particular, is the most common cause of congenital hydronephrosis [4]. In this case, the absence of a tapering obstruction and the intraoperative finding of a completely non-canalized ureter segment favored a diagnosis of pyeloureteral atresia over ureteropelvic junction obstruction.
The diagnosis of pyeloureteral atresia relies heavily on imaging studies. Ultrasonography is typically the first modality used and is instrumental in detecting hydronephrosis [4]. In this case, the massive right-sided hydronephrosis prompted further investigation with contrast-enhanced CT, which was pivotal in identifying the atretic segment of the ureter. CT imaging provides detailed anatomical information and confirms the diagnosis by visualizing the complete obstruction and assessing the extent of hydronephrosis. Our patient had mildly elevated serum creatinine at presentation; however, a contrast-enhanced CT was deemed necessary to clarify the diagnosis. Adequate hydration was ensured, and the risk of contrast-induced nephropathy was considered low, as pediatric patients with mild renal impairment (eGFR >30 mL/min/1.73 m2) are generally not at high risk.
Differential diagnosis for severe hydronephrosis in young children includes other causes of obstructive uropathy such as ureteral stricture, congenital ureteral valves, or bladder outlet obstruction [5]. However, the distinctive finding of a completely obstructed ureteropelvic junction with no flow beyond the obstruction supports the diagnosis of pyeloureteral atresia. It is crucial to differentiate this from conditions that may present similarly but require different management approaches.
While the imaging findings and intraoperative observations strongly suggested pyeloureteral atresia, the absence of pathological confirmation remains a limitation of this report. The overlap of imaging characteristics with ureteropelvic junction obstruction makes differentiation challenging. However, the abrupt transition from the dilated renal pelvis to the narrow, non-canalized segment observed intraoperatively was more characteristic of congenital atresia than ureteropelvic junction obstruction, which typically presents with a tapered narrowing. This observation, coupled with the absence of a patent lumen, reinforced the diagnosis of pyeloureteral atresia.
The management of pyeloureteral atresia is primarily surgical. The goal of surgical intervention is to relieve the obstruction and restore normal urinary flow. Pyeloplasty, the procedure performed in this case, involves excising the atretic segment of the ureter and reconstructing the ureteropelvic junction [5]. This approach is generally successful, with studies indicating high rates of functional improvement and resolution of hydronephrosis postoperatively. Early surgical intervention is essential to prevent long-term renal impairment and preserve kidney function.
Postoperative care involves monitoring for complications such as infection or postoperative renal dysfunction [6]. Although this patient had severe hydronephrosis with cortical thinning, a renal scan (eg, MAG3 or DMSA) was not performed during the acute phase due to the need for urgent surgical intervention. Instead, renal function was evaluated through serial serum creatinine levels and imaging. The child’s renal function improved significantly following surgery, as evidenced by the normalization of serum creatinine levels and resolution of hydronephrosis on follow-up imaging.
The importance of this case extends beyond its rarity, emphasizing the need for awareness and early diagnosis of pyeloureteral atresia in pediatric patients presenting with abdominal pain and hydronephrosis. It also shows the effectiveness of modern imaging techniques in diagnosing and managing congenital anomalies. Continued research and case reporting are essential to improving our understanding of this condition and refining treatment strategies to optimize outcomes for affected children.
Conclusions
This case demonstrates the significance of early diagnosis and timely surgical intervention in managing severe hydronephrosis caused by suspected pyeloureteral atresia. While the imaging findings and intraoperative observations strongly suggested this rare condition, the absence of pathological confirmation introduced diagnostic uncertainty. The successful resolution of hydronephrosis and normalization of renal function in the short term emphasize the potential benefits of prompt surgical management. However, further follow-up and pathological evidence would be necessary to conclusively differentiate pyeloureteral atresia from other similar conditions, such as UPJO. Future reports should include comprehensive diagnostic data and long-term outcomes to strengthen the understanding and management of this rare congenital anomaly. When pyeloureteral atresia is detected at birth, timely surgical intervention is typically recommended within the first few weeks to months of life, depending on the severity of hydronephrosis and renal function. Early correction is crucial to preserve renal function and prevent irreversible damage.
Figures
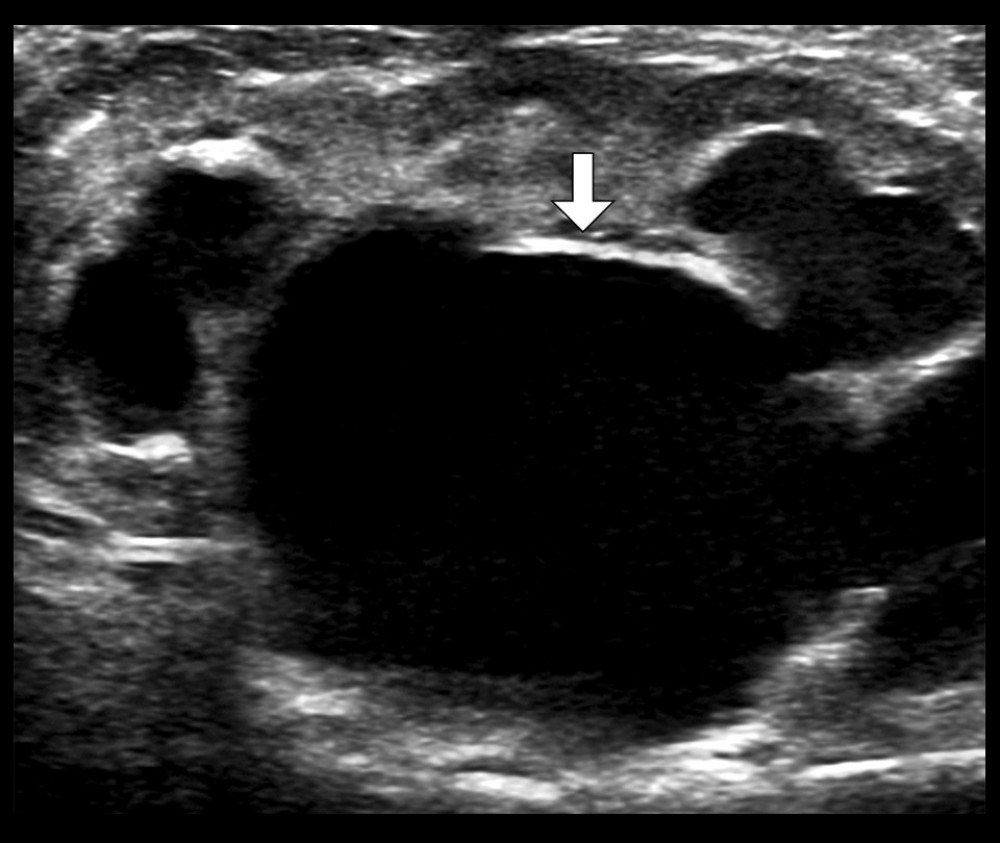 Figure 1. Preoperative renal ultrasound imageGreyscale ultrasound image demonstrating significant hydronephrosis (arrow) with thinning of the renal parenchyma.
Figure 1. Preoperative renal ultrasound imageGreyscale ultrasound image demonstrating significant hydronephrosis (arrow) with thinning of the renal parenchyma.  Figure 2. Contrast-enhanced CT scan of the abdomen and pelvis (coronal view)An axial CT image demonstrating massive right-sided hydronephrosis and a dilated renal pelvis. A narrow, atretic segment is observed at the ureteropelvic junction (arrow), consistent with the diagnosis of pyeloureteral atresia.
Figure 2. Contrast-enhanced CT scan of the abdomen and pelvis (coronal view)An axial CT image demonstrating massive right-sided hydronephrosis and a dilated renal pelvis. A narrow, atretic segment is observed at the ureteropelvic junction (arrow), consistent with the diagnosis of pyeloureteral atresia. 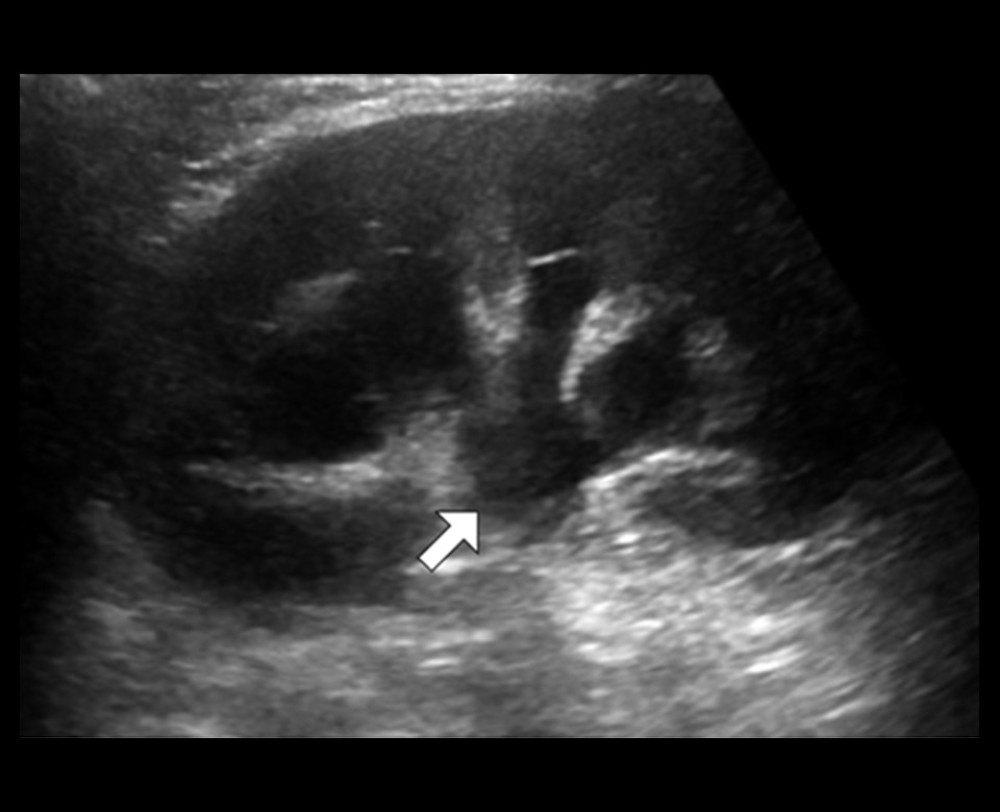 Figure 3. Postoperative renal ultrasound imagePostoperative greyscale ultrasound image demonstrating marked interval improvement in the hydronephrosis (arrow).
Figure 3. Postoperative renal ultrasound imagePostoperative greyscale ultrasound image demonstrating marked interval improvement in the hydronephrosis (arrow). References
1. Bagnara V, Castorina S, Nappo SG, Hypothesis on etiopathogenesis, congenital or acquired, of an imperforate distal ureter: A case report: J Med Case Rep, 2015; 9; 227
2. Estrada CR, Prenatal hydronephrosis: Early evaluation: Curr Opin Urol, 2008; 18; 401-3
3. Kannaiyan L, Karl S, Mathai J, Congenital ureteric stenosis: A study of 17 children: Pediatr Surg Int, 2009; 25; 513-17
4. Lima M, Di Salvo N, Portoraro A, Uretero-pelvic junction stenosis: Considerations on the appropriate timing of correction based on an infant population treated with a minimally-invasive technique: Children (Basel), 2021; 8; 107
5. Cancian M, Pareek G, Caldamone A, Histopathology in ureteropelvic junction obstruction with and without crossing vessels: Urology, 2017; 107; 209-13
6. Mendelsohn C, Functional obstruction: The renal pelvis rules: J Clin Invest, 2004; 113; 957-59
Figures
Figure 1. Preoperative renal ultrasound imageGreyscale ultrasound image demonstrating significant hydronephrosis (arrow) with thinning of the renal parenchyma.Figure 2. Contrast-enhanced CT scan of the abdomen and pelvis (coronal view)An axial CT image demonstrating massive right-sided hydronephrosis and a dilated renal pelvis. A narrow, atretic segment is observed at the ureteropelvic junction (arrow), consistent with the diagnosis of pyeloureteral atresia.Figure 3. Postoperative renal ultrasound imagePostoperative greyscale ultrasound image demonstrating marked interval improvement in the hydronephrosis (arrow). In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133