20 June 2025: Articles 
Incidental Finding of a Primary Polypoid Low-Grade B-Cell Gastric Lymphoma Managed with Chemotherapy
Unusual clinical course, Challenging differential diagnosis
MengHan WangDOI: 10.12659/AJCR.947782
Am J Case Rep 2025; 26:e947782






Abstract
BACKGROUND: This report describes the case of a 57-year-old man with an incidental finding of a primary polypoid low-grade B-cell gastric lymphoma managed with chemotherapy. The case has unique clinical features and represents an uncommon manifestation of gastric follicular lymphoma. This report seeks to raise awareness among clinicians regarding early detection and diagnosis of this condition.
CASE REPORT: A middle-aged man was referred for further evaluation following the incidental detection of a gastric mass during a routine health check-up. Gastroscopy revealed an irregular lesion on the gastric wall. Contrast-enhanced CT showed a well-defined polypoid mass. Endoscopic biopsy was performed, and histopathological examination showed neoplastic lymphoid follicles. Immunohistochemical staining was positive for CD20, CD10, and BCL-2, confirming a diagnosis of grade 2 follicular lymphoma. The patient underwent standard chemotherapy, consisting of rituximab, cyclophosphamide, doxorubicin (hydroxydaunorubicin), vincristine (Oncovin), and prednisone(R-CHOP), and the condition remained stable with no signs of recurrence during follow-up.
CONCLUSIONS: Primary follicular lymphoma of the stomach is a rare type of gastric tumor, often overlooked in early diagnosis. Standard treatment regimens, such as R-CHOP, are effective in controlling the disease. This case highlights the importance of considering lymphoma in the diagnosis of gastric subepithelial lesions, even in asymptomatic patients. It underscores the value of early endoscopic evaluation and histopathological confirmation in guiding timely and effective treatment.
Keywords: Diagnosis, endoscopy, Lymphoma, Follicular, Gastric Mucosa, Humans, Male, Stomach Neoplasms, Middle Aged, Incidental Findings, Vincristine, Cyclophosphamide, Antineoplastic Combined Chemotherapy Protocols, doxorubicin, Prednisone, rituximab, Gastroscopy, Lymphoma, B-Cell, Antibodies, Monoclonal, Murine-Derived
Introduction
Follicular lymphoma (FL) is a common subtype of non-Hodgkin B-cell lymphoma. In the gastrointestinal tract, large B-cell lymphoma and mucosa-associated lymphoid tissue (MALT) lymphoma are more common, while FL is relatively rare [1]. Gastric lymphoma accounts for approximately 5% of gastric neoplasms but is the most common location for extranodal lymphomas, representing about 30% to 40% of these cases and 55% to 65% of lymphomas affecting the gastrointestinal tract [2]. Most FL cases occur in lymph nodes, whereas extranodal FL is less prevalent [1]. The gastrointestinal tract is the most common site for extranodal FL, accounting for approximately 40% of cases. Most gastrointestinal FLs are secondary to systemic lymphoma [3]. FL affecting the duodenum is more common, whereas primary gastric FL is extremely rare. A study by Takata et al revealed that out of 125 cases of primary gastrointestinal FL, 111 cases (89%) involved the duodenum, 50 cases (40%) involved the jejunum, 28 cases (22%) involved the ileum, 5 cases (4%) involved the colon, and only 2 cases (1.6%) involved the stomach [4]. In most reported cases, the disease remains confined to the gastrointestinal tract and regional lymph nodes, and even when the disease progresses, the prognosis is generally favorable [5].
Endoscopically, primary gastric FL typically presents as a submucosal tumor or slightly elevated lesion, while MALT lymphoma and diffuse large B-cell lymphoma often present as ulcerative or depressed lesions [6]. Endoscopic observation alone cannot reliably differentiate FL from other submucosal tumors, including gastric cancer, ectopic pancreas, neuroendocrine tumors, and leiomyomas [5]. Early diagnosis of primary gastric FL is a significant challenge for gastroenterologists. To overcome these diagnostic challenges, it is essential to integrate use of other diagnostic tools. Firstly, endoscopic ultrasound (EUS) has shown significant advantages in evaluating submucosal lesions [7]. A previous study has demonstrated that EUS can assist in identification of hypoechoic submucosal lesions and determination the layer of origin, which is crucial for distinguishing FL from other submucosal tumors such as gastrointestinal stromal tumors (GIST) or neuroendocrine tumors [3]. Additionally, fine-needle aspiration (FNA) under EUS guidance allows for precise tissue sampling, thus greatly improving diagnostic accuracy.
After performing the fine-needle aspiration, immunohistochemical analysis is essential to confirm the diagnosis of FL. It has been demonstrated in the literature that markers such as CD10, BCL-2, and BCL-6 are crucial in differentiating FL from other gastrointestinal lymphomas [8]. Furthermore, genetic testing, such as the detection of the t(14;18) translocation, can further confirm molecular characteristics of FL [2]. According to a previous report, over 85% of FL patients display BCL-2 gene translocations, a molecular feature that not only aids in diagnosis but also provides valuable insights for prognosis and treatment planning [9].
Although EUS and fine-needle aspiration biopsy have been shown to significantly improve the accuracy of FL diagnosis, advanced endoscopic imaging techniques such as narrow-band imaging (NBI) also demonstrate potential for early screening [10]. A study indicated that NBI can clearly display the vascular structure of submucosal lesions, thereby facilitating identification of the “tree-like appearance” of lymphoma cell infiltration, which is indicative of significant neovascularization [11]. Although NBI alone is not sufficient for diagnosis, its integration with conventional endoscopic techniques and pathology can significantly enhance the sensitivity of early detection.
Recently, we treated a 57-year-old man with an incidental finding of a primary polypoid low-grade B-cell gastric lymphoma managed with chemotherapy. The diagnosis was confirmed following multiple imaging and pathological examinations, including endoscopic biopsy. This article discusses the imaging findings, endoscopic features, and pathological results of this case, providing a reference for the future diagnosis and treatment of this rare disease. The requirement of written informed consent was waived by the Ethics Committee of our hospital.
Case Report
A 57-year-old man underwent an upper-gastrointestinal endoscopy during a routine health check-up, which revealed a raised lesion in the gastric body, accompanied by chronic atrophic gastritis and a negative result for
To further investigate the nature of the lesion, upper-gastrointestinal endoscopy was performed. The white-light endoscopy revealed punctate erythema in the gastric fundus and body, with thickened mucosal folds exhibiting a serpentine appearance. A raised lesion with a central depression, measuring approximately 1.5×1.2 cm, was observed on the greater curvature of the middle gastric body. Endoscopic ultrasound revealed a homogeneous hypoechoic lesion in the middle gastric body. The lesion appeared firm, with poor elasticity, and originated from the submucosal layer (Figure 2). Due to the difficulty of diagnosis solely based on endoscopic findings, fine-needle aspiration (22G) biopsy was performed, and the pathology report confirmed follicular lymphoma, grade 2. Immunohistochemical staining showed CD21 (FDC network), CD20 (diffusely positive), CD3 (scattered positive), CD10 (positive), BCL-6 (positive), MUM1 (partially positive), BCL-2 (approximately 90% positive), CD5 (negative), CyclinD1 (negative), C-Myc (20%positive), PAX-5(positive), and CD19/CD22 (Figure 3). In situ hybridization for Epstein-Barr virus-encoded RNA (EBER) was negative. Due to financial reasons, the patient refused to undergo genetic testing. Based on the histopathological features observed with hematoxylin and eosin (H&E) staining, together with the immunohistochemical profile, a final pathology diagnosis of follicular lymphoma was established.
The patient was referred to the Hematology Department for further evaluation. Subsequently, he underwent positron emission tomography-computed tomography (PET-CT) (Figure 1), which demonstrated irregular thickening with high metabolic activity in the gastric body, consistent with follicular lymphoma, and a highly metabolic lymph node on the greater curvature of the stomach, suggesting lymphomatous involvement. The bone marrow biopsy revealed the absence of tumor cell infiltration. Although most primary gastrointestinal lymphomas are of the MALT type, they typically exhibit negative immunohistochemical staining for CD10, BCL6, and BCL2, which was inconsistent with our pathology findings [11]. Furthermore, PET-CT revealed no evidence of disease in other organs. Therefore, a diagnosis of primary gastric follicular lymphoma, stage II according to the Lugano classification, was considered. Given that gastric FL is not an indication for endoscopic submucosal dissection (ESD), and after excluding contraindications, we initiated R-CHOP chemotherapy, which consisted of rituximab 700 mg on day 0, cyclophosphamide 130 mg on day 1, doxorubicin 90 mg on day 1, vincristine 2 mg on day 1, and dexamethasone 16 mg on days 1–5. Prior to the administration of chemotherapy, hydration, alkalinization, and antiemetic treatments were administered. The patient tolerated the treatment well and did not report significant discomfort. He is currently under close outpatient follow-up.
Discussion
This case highlights several important clinical insights regarding the diagnosis and management of primary gastric follicular lymphoma (FL), a rare subtype of extranodal non-Hodgkin lymphoma. Due to its rarity, nonspecific symptoms, and often indolent course, primary gastric FL is easily overlooked or misdiagnosed, being particularly mistaken for mucosa-associated lymphoid tissue (MALT) lymphoma, which shares overlapping histologic features but differs significantly in pathogenesis, clinical course, and treatment strategy [12].
Follicular lymphoma is a common type of non-Hodgkin lymphoma, typically occurring in lymph nodes but also involving other organs such as the liver, spleen, and bone marrow. However, primary gastrointestinal FL is rare, accounting for only 1–3.6% of gastrointestinal non-Hodgkin lymphomas [1]. Primary gastric lymphomas are predominantly classified into 3 categories: diffuse large B-cell lymphoma (DLBCL), mucosa-associated lymphoid tissue (MALT) lymphoma, and FL [6]. In endoscopic examinations, DLBCL is characterized by the presence of ulcerative, nodular, or mass-like lesions. The most common endoscopic feature of DLBCL is ulceration, which typically presents as deep, irregular ulcers with necrotic bases and exudate [13]. The ulcer margins are often irregular, and the lesions frequently exhibit extensive invasion into the gastric wall. Occasionally, raised masses or nodular lesions are observed, with thickening of the gastric wall taking on a nodular or mass-like appearance [13]. In advanced stages, widespread mucosal erosion and hemorrhage may be seen on endoscopy [14].
MALT lymphoma is closely associated with
Furthermore, DLBCL and MALT lymphoma are more frequently associated with lymph node involvement or systemic spread, whereas FL tends to remain localized, with fewer cases of widespread dissemination [16]. Most gastric FL presents as hypoechoic submucosal tumor-like lesions, with a few mucosal changes during EUS examinations [11]. Depressed and ulcerative lesions are rare compared with MALT lymphoma or diffuse large B-cell lymphoma. These findings were consistent with the endoscopic findings in the present case. Previous studies have shown that primary intestinal FL often presents with symptoms such as bowel obstruction, whereas primary gastric FL typically lacks the clinical symptoms such as abdominal pain, diarrhea, early satiety, bloating, or positive fecal occult blood tests [17]. This aligns with the clinical presentation observed in our patient, whose lesion was discovered during a routine health check-up, highlighting the potential benefit of early endoscopic screening in asymptomatic individuals.
From the pathological perspective, FL and MALT lymphoma have distinct immunohistochemical profiles. MALT lymphoma typically expresses CD20 and CD79a as B-cell markers and is associated with BCL-10 and MALT1 gene abnormalities [18]. Conversely, FL is often positive for BCL-2 and CD10, and is associated with the t(14;18) chromosomal translocation [19]. These immunohistochemical differences are of paramount importance in distinguishing these 2 types of lymphomas.
The patient underwent standard laboratory tests and an enhanced abdominal CT scan upon admission. However, because the lesion on imaging could be easily mistaken for gastric cancer or other malignant lesions, we arranged for electronic gastroscopy and endoscopic ultrasound (EUS). As in a previously reported case, narrow-band imaging (NBI) revealed a “tree-like appearance” (TLA) phenomenon, which indicated significant lymphomatous infiltration and associated neovascularization [11]. Although TLA was initially studied and defined in MALT lymphoma [20], the presence of TLA during endoscopy does not necessarily rule out the possibility of follicular lymphoma. In our patient’s NBI imaging, the typical TLA was not observed. We speculate that this may be attributable to the fact that he had grade 2 lymphoma. According to the guidelines, grade 3B FL (characterized by sheet-like blastoid cells) is considered an aggressive lymphoma, while grades 1, 2, and 3A are categorized as indolent diseases [21]. For indolent lymphomas, tumor cell infiltration and neovascularization are relatively less pronounced, which may explain the absence of typical TLA.
Due to the lack of specific endoscopic features for FL, early fine-needle aspiration biopsy and comprehensive pathological evaluation, including immunohistochemical analysis, are crucial for correct diagnosis [10]. In this case, the diagnosis of gastric FL was confirmed based on pathological and immunohistochemical findings. This case highlights that early tissue biopsy is a critical tool in avoiding misdiagnosis, and EUS-guided fine-needle aspiration biopsy is a safe and feasible method for obtaining tissue samples. For the diagnosis of primary gastric FL, a thorough upper-gastrointestinal endoscopic examination is necessary, as well as a comprehensive ultrasound evaluation of lymph nodes and bone marrow biopsy [22]. This is necessary to ascertain the disease stage, which is crucial for developing an appropriate treatment plan.
Immunochemotherapy is currently the most commonly used treatment option both in China and internationally [23]. Among these, the combination of rituximab and chemotherapy has become the standard first-line treatment for patients with FL11/14/24 4: 20: 00 AM. Both the CHOP regimen and the CVP regimen (Cyclophosphamide + Vincristine + Prednisone) have been shown to improve both the short-term and long-term prognosis of patients. Of these, the R-CHOP regimen is one of the most frequently used standard treatments for FL patients, while the R-CVP regimen is more suitable for elderly patients or those with compromised cardiac function [21]. For patients in stage I-II FL without bulky disease (tumor diameter less than 7 cm), there is sufficient clinical evidence to support the use of involved-site radiation therapy (ISRT) [24]. However, in our patient, due to the specific location of the gastric FL and to minimize the risk of perforation and bleeding, we opted for systemic chemotherapy with the R-CHOP regimen, taking into account the patient’s strong preference for treatment.
The Follicular Lymphoma International Prognostic Index (FLIPI) is widely used to predict the prognosis of patients with FL. With the increasing use of anti-CD20 monoclonal antibody therapy for FL, the FLIPI-2 model has become more commonly applied in clinical practice [25]. FLIPI-2 incorporates the following factors: β2-microglobulin levels exceeding the upper limit of the normal range, the largest involved lymph node having a diameter greater than 6 cm, bone marrow involvement, hemoglobin levels <120 g/L, and age >60 years [26]. One point is assigned for each factor, resulting in a risk classification: a score of 0–1 point indicates low risk, 2 points indicates intermediate risk, and 3–5 points indicates high risk. The 2-year overall survival rates for these groups are 98%, 94%, and 87%, respectively, while the 2-year progression-free survival rates are 84%, 70%, and 42%, respectively [26].
Conclusions
We report a rare case of primary gastric follicular lymphoma that presented as a submucosal tumor on endoscopy. In this case, EUS and NBI imaging were not sufficient for an accurate diagnosis, thus necessitating EUS-guided fine-needle aspiration biopsy, followed by pathological and immunohistochemical examination. The patient was subsequently treated with R-CHOP chemotherapy and is currently under close outpatient follow-up.
Figures
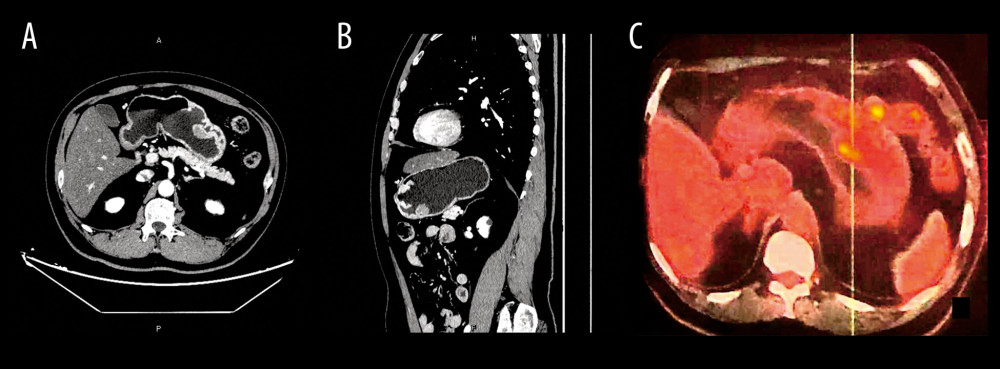 Figure 1. (A, B) Enhanced abdominal computed tomography (CT) scan image of primary gastric follicular lymphoma; (C) Positron emission tomography-computed tomography (PET-CT) image of primary gastric follicular lymphoma.
Figure 1. (A, B) Enhanced abdominal computed tomography (CT) scan image of primary gastric follicular lymphoma; (C) Positron emission tomography-computed tomography (PET-CT) image of primary gastric follicular lymphoma. 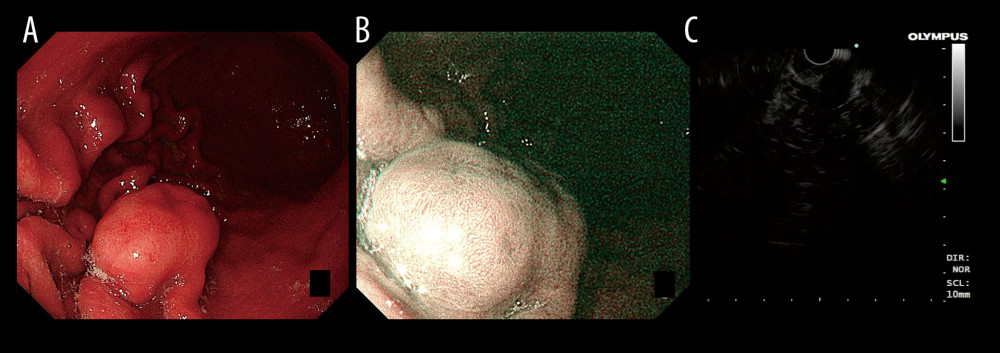 Figure 2. Endoscopy images of primary gastric follicular lymphoma: (A) White-light; (B) Narrow-band; (C) Endoscopic ultrasound.
Figure 2. Endoscopy images of primary gastric follicular lymphoma: (A) White-light; (B) Narrow-band; (C) Endoscopic ultrasound.  Figure 3. Immunohistochemistry: (A) Hematoxylin and eosin (H&E) staining, ×60; (B) CD10 expression, ×60; (C) CD20 expression, ×60; (D) BCL-2 expression, ×60; (E) BCL-6 expression, ×60; (F) Ki-67 expression, ×60.
Figure 3. Immunohistochemistry: (A) Hematoxylin and eosin (H&E) staining, ×60; (B) CD10 expression, ×60; (C) CD20 expression, ×60; (D) BCL-2 expression, ×60; (E) BCL-6 expression, ×60; (F) Ki-67 expression, ×60. References
1. Tran QT, Nguyen Duy T, Nguyen-Tran BS, Endoscopic and histopathological characteristics of gastrointestinal lymphoma: A multicentric study: Diagnostics (Basel), 2023; 13(17); 2767
2. Herlevic V, Reynolds SB, Morris JD, Gastric lymphoma: StatPearls, 2025, StatPearls Publishing http://www.ncbi.nlm.nih.gov/books/NBK567799/
3. Goto A, Nishikawa J, Sakaida I, Primary gastric follicular lymphoma presenting as a submucosal tumor: ACG Case Rep J, 2020; 7(11); e00478
4. Takata K, Okada H, Ohmiya N, Primary gastrointestinal follicular lymphoma involving the duodenal second portion is a distinct entity: A multicenter, retrospective analysis in Japan: Cancer Sci, 2011; 102(8); 1532-36
5. Watanabe T, Recent advances in treatment of nodal and gastrointestinal follicular lymphoma: World J Gastroenterol, 2023; 29(23); 3574-94
6. Na HY, Kim YA, Lee C, Gastric follicular lymphoma: A report of 3 cases and a review of the literature: Oncol Lett, 2018; 16(1); 741-48
7. Park E, Nishimura M, Simoes P, Endoscopic advances in the management of gastric cancer and premalignant gastric conditions: World J Gastrointest Endosc, 2023; 15(3); 114-21
8. Bannerji R, Arnason JE, Advani RH, Odronextamab, a human CD20×CD3 bispecific antibody in patients with CD20-positive B-cell malignancies (ELM-1): Results from the relapsed or refractory non-Hodgkin lymphoma cohort in a single-arm, multicentre, phase 1 trial: Lancet Haematol, 2022; 9(5); e327-e39
9. Loghavi S, Kanagal-Shamanna R, Khoury JD, Fifth Edition of the World Health Classification of Tumors of the Hematopoietic and Lymphoid Tissue: Myeloid neoplasms: Mod Pathol, 2024; 37(2); 100397
10. Kouanda A, Mclean R, Faggen A, Telecytology versus in-room cytopathologist for EUS-guided FNA or fine-needle biopsy sampling of solid pancreatic lesions: Gastrointest Endosc, 2023; 97(3); 466-71
11. Koya Y, Watanabe T, Kume K, Usefulness of magnifying endoscopy and endoscopic ultrasonography for the gastric involvement of follicular lymphoma: Clin J Gastroenterol, 2020; 13(1); 55-59
12. Ishikawa E, Nakamura M, Satou A, Shimada K, Nakamura S, Mucosa-associated lymphoid tissue (MALT) lymphoma in the gastrointestinal tract in the modern era: Cancers, 2022; 14(2); 446
13. Nakamura T, Masaki Y, Kameyama N, Unique endoscopic features of primary biliary diffuse large B-cell lymphoma: A case report with literature review (with video): DEN Open, 2024; 5(1); e414
14. Kim MS, Park JH, Kim JY, Lim SN, Lee J, Upper gastrointestinal bleeding caused by direct invasion of diffuse large B-cell lymphoma into the stomach in a patient with HIV infection: A case report: Medicine (Baltimore), 2019; 98(28); e16363
15. Kim H, Shin D, Son SM, Clinicopathological and molecular genetic characteristics of primary gastric follicular lymphoma: Hum Pathol, 2023; 136; 114-22
16. Araújo GR, Morais-Perdigão AL, Lopez-de-Cáceres CV, Lymphomas affecting the submandibular glands: Med Oral Patol Oral Cir Bucal, 2024; 29(1); e78-e86
17. Takahashi Y, Taniguchi H, Haruhi F, Pathogenesis of gastrointestinal follicular lymphomas: Consideration based on histopathology and endoscopic findings: Am J Surg Pathol, 2023; 47(10); 1134-43
18. Cho J, Basic immunohistochemistry for lymphoma diagnosis: Blood Res, 2022; 57(S1); 55-61
19. Maeshima AM, Taniguchi H, Suzuki T, Comparison of clinicopathologic characteristics of gastric follicular lymphomas and duodenal follicular lymphomas: Hum Pathol, 2017; 65; 201-8
20. Nonaka K, Ishikawa K, Arai S, A case of gastric mucosa-associated lymphoid tissue lymphoma in which magnified endoscopy with narrow band imaging was useful in the diagnosis: World J Gastrointest Endosc, 2012; 4(4); 151-56
21. Dreyling M, Ghielmini M, Rule S, Newly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up: Ann Oncol, 2021; 32(3); 298-308
22. Pausawasdi N, Maipang K, Sriprayoon T, Charatcharoenwitthaya P, Role of endoscopic ultrasound-guided fine-needle aspiration in the evaluation of abdominal lymphadenopathy of unknown etiology: Clin Endosc, 2022; 55(2); 279-86
23. Flinn IW, van der Jagt R, Kahl B, First-line treatment of patients with indolent non-hodgkin lymphoma or mantle-cell lymphoma with bendamustine plus rituximab versus R-CHOP or R-CVP: Results of the BRIGHT 5-year follow-up study: J Clin Oncol, 2019; 37(12); 984-91
24. Wark A, Kim JY, Mavriopoulou E, PET/CT-based target volume definition in involved-site radiotherapy for treatment of early-stage nodal follicular lymphoma: Strahlenther Onkol, 2025 [Online ahead of print]
25. Jóna Á, Kiss E, Illés Á, Prognostication of follicular lymphoma: A review of prognostic scores and factors: Diagn (basel Switz), 2025; 15(5); 647
26. Jacobsen E, Follicular lymphoma: 2023 update on diagnosis and management: Am J Hematol, 2022; 97(12); 1638-51
Figures
Figure 1. (A, B) Enhanced abdominal computed tomography (CT) scan image of primary gastric follicular lymphoma; (C) Positron emission tomography-computed tomography (PET-CT) image of primary gastric follicular lymphoma.Figure 2. Endoscopy images of primary gastric follicular lymphoma: (A) White-light; (B) Narrow-band; (C) Endoscopic ultrasound.Figure 3. Immunohistochemistry: (A) Hematoxylin and eosin (H&E) staining, ×60; (B) CD10 expression, ×60; (C) CD20 expression, ×60; (D) BCL-2 expression, ×60; (E) BCL-6 expression, ×60; (F) Ki-67 expression, ×60. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133