11 July 2025: Articles 
Term Pregnancy in Herlyn-Werner-Wunderlich Syndrome: Successful Management of Congenital Obstructed Hemivagina and Ipsilateral Renal Agenesis (OHVIRA)
Unusual or unexpected effect of treatment, Rare disease
Norah AlqntashDOI: 10.12659/AJCR.947938
Am J Case Rep 2025; 26:e947938






Abstract
BACKGROUND: Obstructed hemivagina and ipsilateral renal agenesis (OHVIRA) syndrome, also known as Herlyn-Werner-Wunderlich syndrome, is a rare congenital anomaly characterized by a didelphic uterus, an obstructed hemivagina, and ipsilateral renal agenesis. This report describes a case of successful term pregnancy in a 20-year-old woman with OHVIRA syndrome.
CASE REPORT: A 20-year-old Saudi woman presented with primary infertility after 3 years of unsuccessful conception attempts, including failed assisted reproductive techniques. Her medical history was unremarkable, and menstrual cycles were regular but variable in flow. Pelvic ultrasound revealed a didelphic uterus and a fluid collection in the vaginal canal measuring 36.0×17.3 mm. MRI confirmed a didelphic uterus with an obstructed right hemivagina and hematocolpos. A renal ultrasound revealed right-sided renal agenesis, consistent with OHVIRA syndrome. Surgical management involved drainage of hematocolpos and excision of the obstructing vaginal septum. The patient recovered without complications. Eleven months later, she presented with missed menstruation and a positive β-hCG level of 23 000 mIU/L. Ultrasound confirmed an intrauterine pregnancy in the right uterus. The pregnancy was uneventful, and she delivered a healthy male infant weighing 2.4 kg via elective cesarean section at 38 weeks of gestation.
CONCLUSIONS: Early recognition and accurate diagnosis of OHVIRA syndrome using appropriate imaging are essential for timely surgical intervention, which can significantly improve reproductive outcomes. This case highlights that successful full-term pregnancy is achievable following proper management.
Keywords: Pregnancy, Congenital Abnormalities, Infertility, Case Reports, Hereditary Renal Agenesis, Mullerian aplasia, Humans, Female, kidney, Vagina, Kidney Diseases, young adult, Uterus, Abnormalities, Multiple, Syndrome
Introduction
Obstructed hemivagina ipsilateral renal agenesis (OHVIRA) syndrome, formerly known as Herlyn-Werner-Wunderlich (HWW) syndrome, is a rare congenital condition of urogenital abnormality [1]. The precise etiology remains uncertain; however, it is hypothesized that the maldevelopment of both Müllerian and Wolffian ducts plays a contributory role [2,3]. It is characterized by a triad of uterine didelphys, unilateral hemivagina obstruction, and ipsilateral kidney agenesis [1]. This syndrome was first described in 1922 and later characterized as a distinct entity in 1976 [2,4]. According to a recent study, the incidence of OHVIRA syndrome is 0.1–3.8% [1]. Most of these abnormalities (17.3%) are renal anomalies, with renal agenesis accounting for 64.6% of them. These abnormalities are also frequently associated with 1 or more extragenital malformations. Renal agenesis and blocked hemivagina were detected in 23.6% of patients with didelphic uterus, whereas 29.1% of patients had related renal abnormalities [5]. Additional extragenital abnormalities include gastrointestinal malformations (12%), congenital heart disease, and skeletal abnormalities (12–19%) [6]. Most cases of OHVIRA syndrome are diagnosed during adolescence, typically after menarche, when patients present with abdominal pain and severe dysmenorrhea [7,8]. It is important to evaluate the syndrome in adolescents and young women who present with persistent vaginal discharge, pelvic pain or mass, primary infertility, or urinary symptoms [9]. Magnetic resonance imaging (MRI) is the primary imaging modality for diagnosing OHVIRA syndrome. However, ultrasound (US) and computed tomography (CT) scans can serve as alternative diagnostic tools [2]. Early detection of OHVIRA syndrome is crucial to prevent potential complications such as infertility and pelvic inflammatory disease [9].
Management typically involves surgical intervention, including hematocolpos drainage and vaginal septum resection [2]. However, anatomical challenges may arise, particularly in adolescent females with a narrow vaginal canal or in cases complicated by hematocolpos-related distortion. Some experts have proposed a staged surgical approach to address these concerns, using initial drainage of the hematocolpos to alleviate anatomical distortion, followed by delayed septal resection after a period of vaginal remodeling and tissue healing [10], which demonstrates a significant impact on fertility outcomes. A retrospective study assessed 51 patients with OHVIRA syndrome for long-term outcomes after surgery. Among the 14 patients who were seeking pregnancy, 12 (85.71%) achieved pregnancy. Out of 16 patients, 14 underwent cesarean sections, with indications including 1 case of placenta previa, 9 cases of breech presentation, and 4 cases of patient’s request. Despite the generally smooth progression of pregnancies, complications were observed in the form of fetal growth restriction (2 cases), placenta previa (1 case), and gestational diabetes (1 case). Based on the study results, the high incidence of breech presentation associated with uterine malformations contributes to the frequent need for cesarean sections. Additionally, careful prenatal monitoring is recommended, especially in cases where unilateral renal agenesis coexists, as it can predispose patients to preeclampsia. However, the literature on pregnancy outcomes in patients with OHVIRA syndrome remains limited [11].
This report describes a case of a successful term pregnancy in a 20-year-old woman with congenital obstructed hemivagina and ipsilateral renal agenesis (Herlyn-Werner-Wunderlich syndrome). We also review the relevant literature to provide a broader clinical context and insights into the case.
Case Report
A 20-year-old Saudi woman and her 28-year-old husband were referred to an outpatient clinic with concerns about primary infertility after trying to conceive naturally for 3 years. She had previously undergone trials of artificial reproductive techniques at another hospital, but she was unaware of the specific methods used, and detailed records were not available. Her medical history was not known to include any chronic diseases, surgery, or medications. Her menstrual cycles were regular but varied in flow, alternating between heavy and light periods.
Following the initial presentation, a comprehensive investigation was initiated to identify the underlying cause. This workup included a complete blood count (CBC), thyroid function tests, and evaluation of hormonal balance through measurements of follicle-stimulating hormone (FSH), luteinizing hormone (LH), and prolactin levels. FSH and LH were assessed as part of a broader fertility evaluation to rule out any underlying hormonal factors that could contribute to her difficulty conceiving, even though her menstrual cycles were regular. However, an anti-Müllerian hormone (AMH) assessment was not performed. The results are summarized in Table 1. Aside from elevated prolactin, all the findings were within normal ranges. To assess male-factor infertility, a human sperm assay (HSA), including sperm count and motility, was performed on the patient’s husband. The semen analysis revealed normal findings, as detailed in Table 2.
Imaging studies were initiated to further evaluate the cause of primary infertility and investigate the potential underlying anatomical abnormalities. A pelvic ultrasound (Figure 1) revealed a didelphys anteverted uterus of normal size, confirming the presence of uterine duplication. Additionally, a fluid collection measuring approximately 36.0×17.3 mm was observed within the vaginal canal (Figure 2), suggesting a possible obstruction or hematocolpos, which warranted further evaluation.
Following the ultrasound, pelvic magnetic resonance imaging (MRI) was performed, providing a more detailed evaluation of the anatomical abnormalities. The MRI confirmed the presence of a didelphic uterus with 2 distinct uterine cavities and separate cervices. Additionally, it identified a vertically-oriented vaginal septum, consistent with a duplicated vagina (Figure 3), further supporting the diagnosis and explaining the previously observed vaginal collection.
The right-sided hemivagina was distended with fluid. This fluid collection extended superiorly into the corresponding right-sided cervix. Both ovaries exhibited normal morphology, and the urinary bladder appeared unremarkable.
Given the combination of uterus didelphys and obstructed hemivagina on MRI, further investigation was warranted to assess for a potential association with OHVIRA syndrome. To confirm or exclude the suspected diagnosis, a renal ultrasound was performed to assess the presence or absence of a kidney ipsilateral to the obstructed hemivagina. The ultrasound revealed a solitary left kidney with normal echogenicity and a size of 12.40×5.86 cm (Figure 4), while the right kidney was not visualized, suggesting renal agenesis. These findings align with the diagnostic criteria for Herlyn-Werner-Wunderlich syndrome, further supporting the diagnosis.
After a thorough clinical evaluation and imaging confirming a diagnosis of OHVIRA syndrome, the patient underwent surgical intervention on 25 October 2018. Examination under anesthesia revealed a didelphic uterus with 2 cervices, 2 ovaries, and 2 dilated fallopian tubes. A significant vaginal bulge on the right side was noted, associated with a hematocolpos collection. No other intra-abdominal abnormalities were identified. A vaginal opening was created to drain the hematocolpos, yielding a foul-smelling collection. Both cervical canals were subsequently identified and accessed. Hysteroscopic evaluation confirmed the presence of 2 separate endometrial cavities, each with a single ostium. A patent canal was established to facilitate future drainage of menstrual blood, and a Foley catheter was inserted to maintain patency. The procedure was completed without intraoperative complications, with minimal blood loss and no evidence of bleeding at the trocar sites. The patient was extubated and transferred to the recovery room in stable condition.
Postoperatively, a follow-up appointment was arranged to evaluate the patient’s recovery. During this visit, the patient reported experiencing no complications and had an uneventful recovery course. However, hysterosalpingography (HSG) and sono-hysterography were not performed after the surgery. Eleven months after the intervention (12 September 2019), the patient presented to the clinic with a chief concern of absence of menstruation. Her last menstrual period (LMP) was on 9 July 2019, suggesting a potential pregnancy.
A quantitative serum human chorionic gonadotropin (β-hCG) test was performed, revealing an elevated level of 23 000 mIU/L, supporting the suspicion of pregnancy. To further confirm the location and viability of the pregnancy, an ultrasound examination was conducted. This imaging identified an intrauterine gestational sac with a viable embryo implanted in the anterior wall of the right uterus (Figure 5), confirming an ongoing intrauterine pregnancy. These findings definitively established the diagnosis.
The pregnancy period was normal and uneventful, and all routine laboratory investigations were within normal limits. She completed 38 weeks of gestation, and on April 2, 2020, she was admitted for an elective cesarean section, delivering a male infant with a birth weight of 2.4 kg, which is on the lower end of the normal range but does not necessarily indicate an abnormal course of pregnancy. There were no indications of placental insufficiency or hypertensive disorders. Table 3 summarizes the key diagnostic steps, findings, and management of this case, providing a concise overview of the patient’s journey from presentation to outcome.
Discussion
In the spectrum of Müllerian anomalies, the syndrome of obstructed hemivagina, uterus didelphys, and ipsilateral renal anomalies is increasingly recognized. Based on an extensive review of the literature, more than 280 cases were reported to the best of our knowledge, indicating an increased understanding of the disorder and improved diagnosis. This case report highlights several crucial learning points. First, obstructed hemivagina ipsilateral renal agenesis (OHVIRA) can present variably, with some patients initially presenting primarily with infertility rather than the commonly described acute pelvic symptoms. Second, detailed diagnostic imaging using ultrasound and MRI is critical for accurate diagnosis, particularly in identifying anatomical abnormalities that may be missed on initial evaluation. Lastly, timely surgical intervention to drain hematocolpos and excise the vaginal septum significantly improves fertility outcomes, as evidenced by our patient’s spontaneous conception and uneventful full-term pregnancy, which underscores the importance of heightened clinical suspicion and comprehensive imaging in patients presenting with infertility and menstrual abnormalities.
The incidence of this syndrome is unknown; however, owing to improved access to advanced imaging and gynecological care, the number of diagnoses will continue to increase.
Clinical diagnosis can be challenging due to nonspecific presenting concerns or heterogeneity of presentation. Few guidelines are available to aid clinicians in making diagnoses. Tan et al conducted a retrospective case review and literature review to determine OHVIRA patient demographics, symptoms, clinical course, and operative management. They reviewed 8 cases of OHVIRA, with 2 symptomatic patients requiring urgent vaginal surgery for hematocolpos, whereas the remaining 6 were diagnosed early through postnatal ultrasound [12]. The study concluded that prepubertal patients with OHVIRA do not require early surgical intervention, and they recommended that ultrasound screenings be performed on female babies with renal agenesis to identify the presence of OHVIRA syndrome. A timely diagnosis and presymptomatic elective surgery can prevent urogynecological complications, which can affect fertility and renal function [12].
Our patient presented with a primary concern of infertility, having attempted to conceive naturally for 3 years. As in most reported cases in the literature, the presenting symptoms were infertility and chronic pelvic pain, which are common with delayed diagnoses outside of adolescence [7,8]. Compared to the more common adolescent presentations with cyclic pelvic pain and hematocolpos after menarche, our case points to the less common clinical course when diagnosis is made in adult life during the evaluation of infertility, emphasizing the heterogeneity of symptom onset and timing of diagnosis.
The literature shows that most cases present within a brief period after menarche with symptoms such as pelvic pain, pelvic mass (hematocolpos), and, in some cases, vaginal discharge or acute urinary retention. Several young women developed hematometrosis, endometriotic ovarian cysts, pelvic adhesions, and genitourinary infections [10,13–19].
Our diagnosis was established with the help of an MRI, which has an added benefit in delineating Müllerian defects [2], as indicated in this case. Radiologic findings offer valuable insights that contribute to definitive diagnosis. Compared to other imaging modalities, MRI is more sensitive and provides an accurate assessment of uterine contour, intrauterine cavity shape, and septum characteristics, along with identifying endometriosis, pelvic inflammation, and adhesions. Anomalies of the urinary system can be detected using transabdominal ultrasound (US) and computed tomography (CT), especially in cases of renal agenesis. The integration of radiologic findings into the diagnostic process enhances diagnostic precision [20]. In cases presenting with pelvic infection or endometriosis, laparoscopic examination may be necessary for accurate diagnosis. A primary obstacle in the management of this condition is the overutilization of invasive surgical procedures, such as laparoscopy or open abdominal surgery, resulting from its rarity.
The preferred treatment for OHVIRA syndrome is removing the vaginal septum, mainly to restore vaginal continuity. This can be achieved either through a single-stage vaginoplasty with septum resection or a two-stage approach, which involves drainage of hematocolpos first, followed by septum resection [14,21,22].
The preferred treatment approach is single-stage vaginoplasty; however, a two-stage procedure may be chosen if infection or anatomical distortion is present [10].
Furthermore, surgery is not an emergency unless accompanied by infection, and pain can be managed with analgesics. If surgery is delayed, continuous hormonal treatment can prevent menstruation and reduce hematocolpos. A single-stage procedure minimizes infection risks and preserves fertility, making laparotomy unnecessary in most cases. Appropriate management yields favorable long-term outcomes, preserves fertility, and achieves successful future pregnancies [13,22].
A survey of 42 patients’ reproductive results following surgical treatment of a blocked hemivagina was conducted by Haddad et al. Nine of these women reported a total of 20 pregnancies [23]. Nine vaginal births and 4 cesarean sections were reported, yielding a 69% live birth rate [24]. Heinonen discovered that patients with uterine didelphys and longitudinal vaginal septum had high rates of preterm delivery (24%), malpresentation (51%), and cesarean section (84%) [25].
Complications after vaginoplasty are rare, but can arise from obstruction of menstrual outflow, leading to various sequelae affecting the reproductive and urinary systems. The most immediate complication of OHVIRA syndrome is hematocolpos, which results from menstrual blood accumulation in the obstructed hemivagina and uterus, thus increasing the risk of infections, pyocolpos, and pelvic inflammatory disease [26].
Tuqan et al reported a case involving a 19-year-old woman who presented with abdominal pain and offensive vaginal discharge [27]. Diagnostic imaging demonstrated a didelphys uterus, obstructed right hemivagina (hematocolpos), and an absent right kidney. Surgical management involved incision, drainage of pyocolpos, and excision of the vaginal septum. Post-surgical follow-up showed successful conception and a full-term pregnancy delivered by cesarean section without complications. Both our case and Tuqan et al’s study emphasize critical similarities, including the presentation of a didelphic uterus, obstructed hemivagina, renal agenesis, and successful reproductive outcomes following surgical management. However, distinct clinical presentations are noted, such as acute symptomatic presentation in Tuqan’s case versus primary infertility presentation in our case [27]. Both cases employed MRI and ultrasound effectively for accurate diagnosis, underscoring their critical role in management planning. These comparative insights emphasize the variability in clinical presentations of OHVIRA syndrome and reinforce that timely surgical intervention can lead to favorable fertility outcomes and uncomplicated pregnancies.
Additionally, OHVIRA syndrome is associated with ipsilateral renal agenesis, placing the solitary kidney at higher risk of complications such as hydronephrosis or infection due to increased functional demands [10]. Early monitoring of renal function is essential to prevent long-term kidney damage. Compared to previous reports, the clinical course of our patient illustrates favorable fertility and pregnancy outcomes, which attest to the importance of early diagnosis and treatment. However, the need for ongoing monitoring remains necessary given the risks involved, such as fetal growth restriction, gestational diabetes, and preeclampsia in patients with concomitant renal anomalies [11].
This case presents a limitation in our postoperative evaluation. While hysterosalpingography (HSG) or sonohysterography is typically used to assess tubal patency following procedures, our patient’s circumstances precluded its performance. She lived over 2000 km from our center and, unfortunately, was lost to follow-up after her surgery. Consequently, the planned postoperative HSG could not be conducted. Her subsequent spontaneous pregnancy, while strongly suggestive of at least unilateral tubal patency, does not provide definitive information regarding the status of both fallopian tubes and the overall impact of the surgical intervention on tubal function. Although pregnancy is the ultimate desired outcome and a positive indicator, it does not replace the objective assessment afforded by HSG or sonohysterography. This case underscores the challenges inherent in managing patients from remote locations and highlights the need for improved follow-up strategies to ensure comprehensive postoperative assessment.
This case report offers several advantages compared to the existing literature. While a substantial body of research addresses the diagnosis and surgical management of OHVIRA syndrome, a relative paucity of data exists regarding long-term reproductive outcomes following surgical intervention, particularly with detailed descriptions of the specific surgical approach employed. Much of the published work focuses on the syndrome’s clinical presentation, imaging features, and surgical techniques for septum resection and drainage of the obstructed hemivagina. However, comprehensive information on subsequent fertility and pregnancy is often limited. This case report addresses this gap by providing a detailed account of a successful pregnancy achieved after 11 months. This focus on reproductive outcomes is crucial for counseling patients with OHVIRA who desire future fertility.
In summary, while the current literature provides a strong foundation for understanding and treating OHVIRA, this case report contributes valuable real-world data on pregnancy outcomes following surgical intervention, offering practical insights for clinicians and patients.
Conclusions
This case highlights the successful full-term pregnancy in a case of OHVIRA syndrome, which is a rare congenital anomaly characterized by uterus didelphys, obstructed hemivagina, and ipsilateral renal agenesis. Early recognition and accurate diagnosis of OHVIRA syndrome using appropriate imaging are essential for timely surgical intervention, which can significantly improve reproductive outcomes. The patient’s natural conception and delivery of a healthy infant underscore the potential for favorable reproductive outcomes with appropriate treatment. This case emphasizes the importance of recognizing Müllerian anomalies in women presenting with infertility and menstrual abnormalities, particularly when associated with renal agenesis. Further research is needed to explore long-term reproductive and renal outcomes in OHVIRA patients, as well as the impact of different treatment approaches on fertility and overall health.
Figures
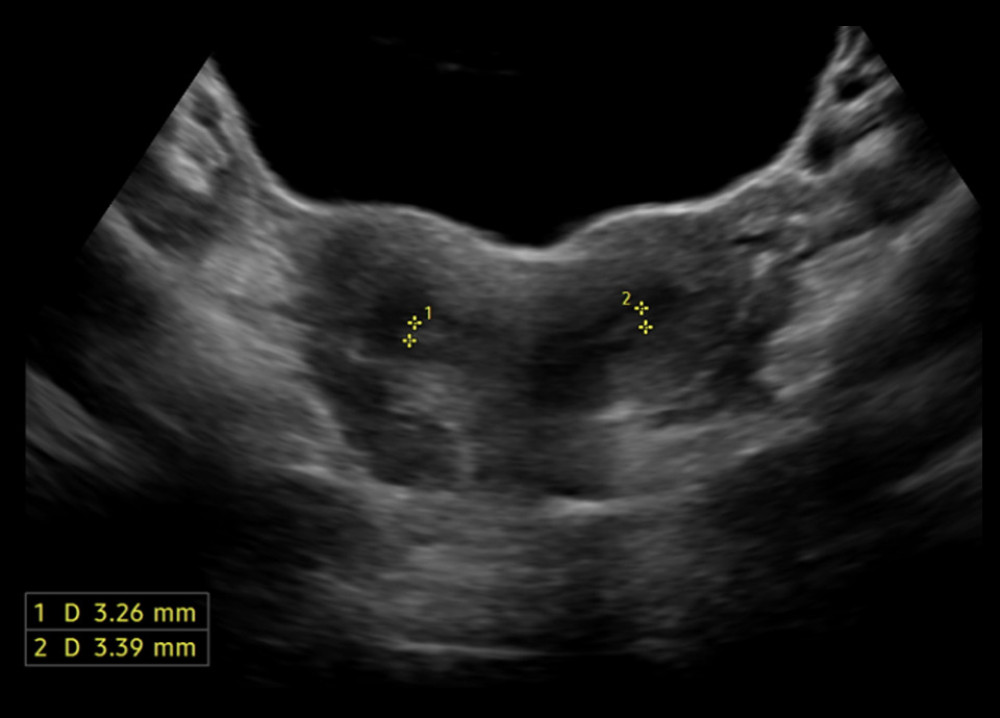 Figure 1. Didelphys uterus on pelvic ultrasoundPelvic ultrasound showing 2 separate endometrial cavities, confirming uterine didelphys. The uterus is anteverted and normal in size.
Figure 1. Didelphys uterus on pelvic ultrasoundPelvic ultrasound showing 2 separate endometrial cavities, confirming uterine didelphys. The uterus is anteverted and normal in size.  Figure 2. Vaginal fluid collection on ultrasoundUltrasound image showing a fluid collection within the vaginal canal measuring 36.0×17.3 mm, indicative of possible obstruction or hematocolpus.
Figure 2. Vaginal fluid collection on ultrasoundUltrasound image showing a fluid collection within the vaginal canal measuring 36.0×17.3 mm, indicative of possible obstruction or hematocolpus. 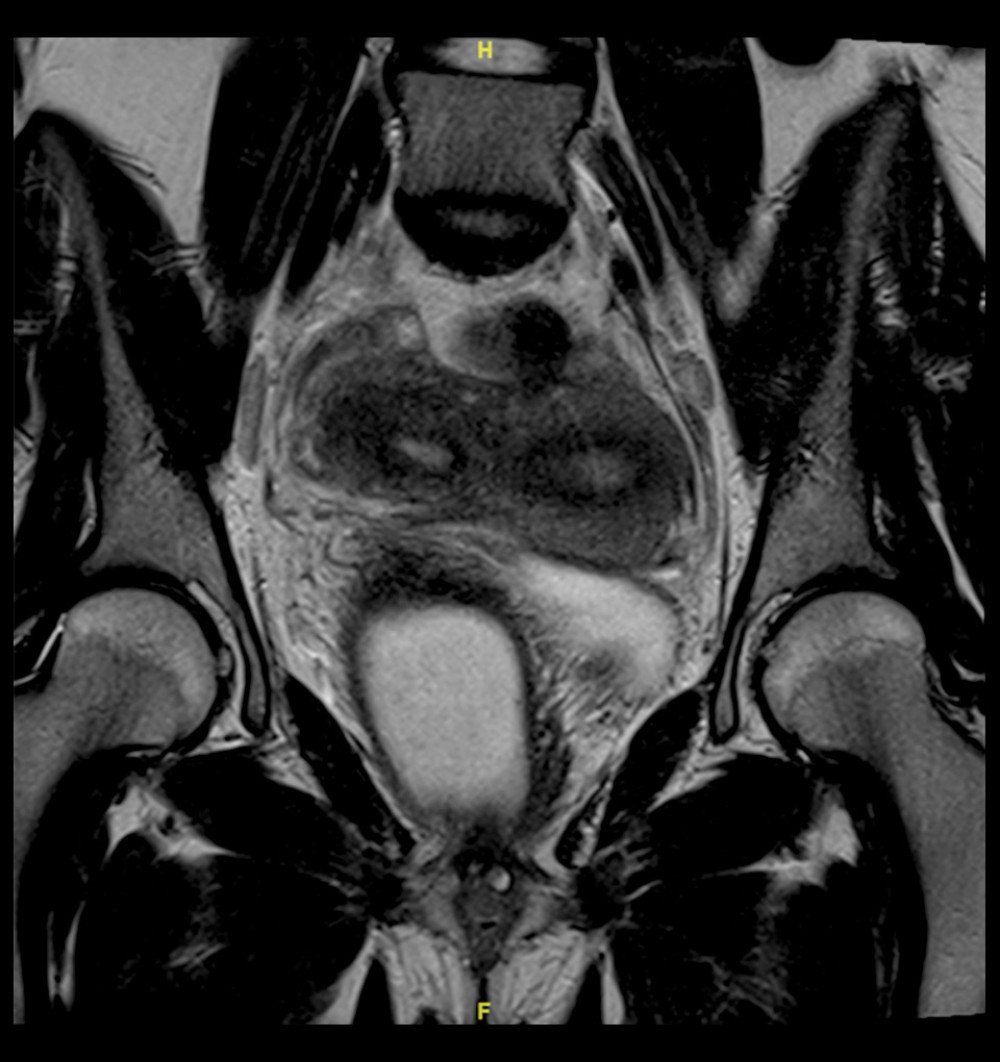 Figure 3. Duplicated uterus and vagina on pelvic magnetic resonance imaging (MRI)MRI showing a didelphic uterus with 2 uterine cavities and 2 cervices. A vertically-oriented vaginal septum is also visible, confirming a duplicated vagina and explaining the associated vaginal fluid collection.
Figure 3. Duplicated uterus and vagina on pelvic magnetic resonance imaging (MRI)MRI showing a didelphic uterus with 2 uterine cavities and 2 cervices. A vertically-oriented vaginal septum is also visible, confirming a duplicated vagina and explaining the associated vaginal fluid collection. 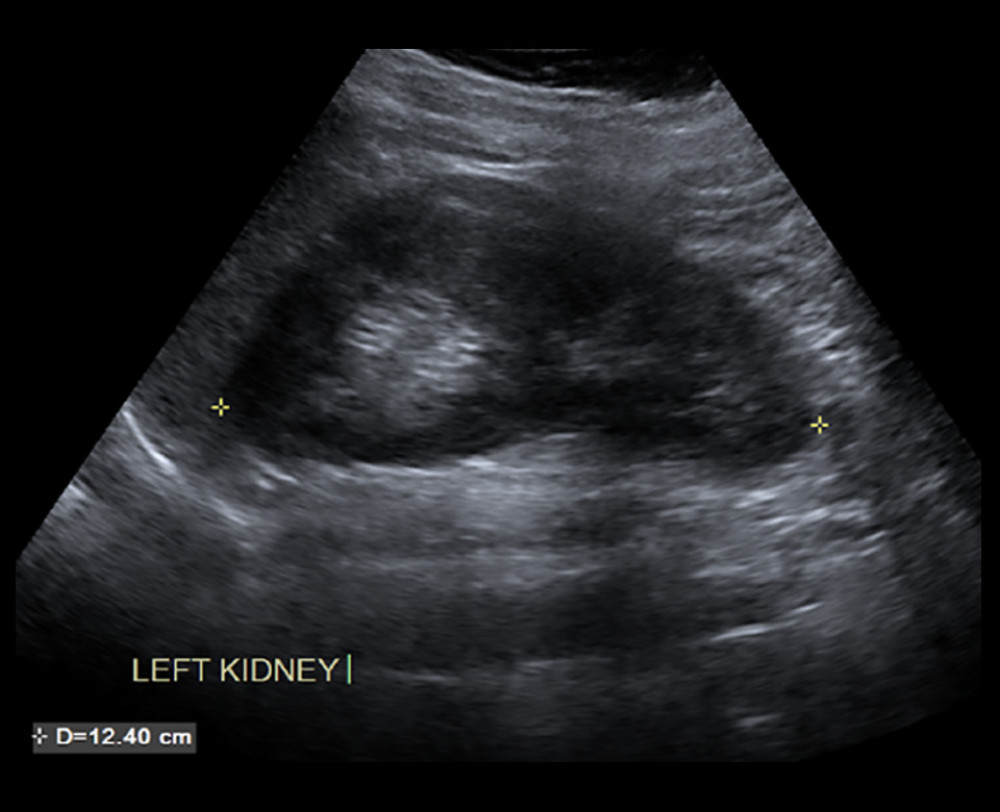 Figure 4. Solitary left kidney on renal ultrasoundRenal ultrasound showing a single left kidney of normal size (12.40×5.86 cm) and echogenicity. No right kidney is visualized.
Figure 4. Solitary left kidney on renal ultrasoundRenal ultrasound showing a single left kidney of normal size (12.40×5.86 cm) and echogenicity. No right kidney is visualized. 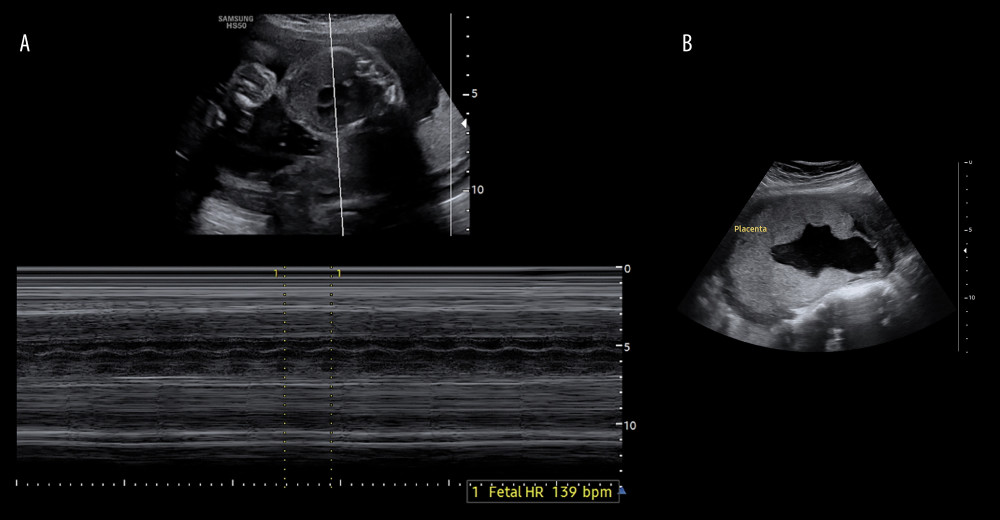 Figure 5. Ultrasound images(A). Ultrasound showing fetal heart rate of 139 beats per minute within an intrauterine gestational sac. (B) Ultrasound showing placenta attached to the anterior uterine wall.
Figure 5. Ultrasound images(A). Ultrasound showing fetal heart rate of 139 beats per minute within an intrauterine gestational sac. (B) Ultrasound showing placenta attached to the anterior uterine wall. References
1. Moufawad G, Giannini A, D’Oria O, Obstructed hemivagina and ipsilateral renal anomaly syndrome: A systematic review about diagnosis and surgical management: Gynecol Minim Invasive Ther, 2023; 12(3); 123-29
2. Jomaa S, Tawashi K, All Rass FA, A challenging diagnosis and management of Herlyn-Werner-Wunderlich Syndrome in low-resource settings: A case report complicated with hydronephrosis: Ann Med Surg (Lond), 2021; 70; 102843
3. Drosdzol-Cop A, Skowronek K, Wilk K, OHVIRA syndrome in 14-year-old girl: Ginekol Pol, 2021 [Online ahead of print]
4. Sijmons A, Broekhuizen S, van der Tuuk K, OHVIRA syndrome: Early recognition prevents genitourinary complications: Ultrasound, 2023; 31; 61-64
5. Heinonen PK, Renal tract malformations associated with Müllerian duct anomalies: Clin Obstet Gynecol Reprod Med, 2018; 4(1); 1-5
6. Pinsonneault O, Goldstein DP, Obstructing malformations of the uterus and vagina: Fertil Steril, 1985; 44; 241-47
7. Mabuchi Y, Hirayama J, Ota N, Ino K, OHVIRA syndrome pre-operatively diagnosed using vaginoscopy and hysteroscopy: A case report: Med Int (Lond), 2021; 1(5); 20
8. Arakaki R, Yoshida K, Imaizumi J, Obstructed hemivagina and ipsilateral renal agenesis (OHVIRA) syndrome: A case report: Int J Surg Case Rep, 2023; 107; 108368
9. Malarazhagan V, Veerasingham M, Sivanesan K, Right-sided obstructed hemivagina ipsilateral renal agenesis (OHVIRA): A case report: Case Rep Womens Health, 2020; 26; e00185
10. Smith NA, Laufer MR, Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome: Management and follow-up: Fertil Steril, 2007; 87; 918-22
11. Candiani M, Vercellini P, Ferrero-Caroggio C, Conservative treatment of Herlyn-Werner-Wunderlich syndrome: Analysis and long-term follow-up of 51 cases: Eur J Obstet Gynecol Reprod Biol, 2022; 275; 84-90
12. Tan YG, Laksmi NK, Yap TL, Preventing the O in OHVIRA (Obstructed Hemivagina Ipsilateral Renal Agenesis): Early diagnosis and management of asymptomatic Herlyn-Werner-Wunderlich Syndrome: J Pediatr Surg, 2020; 55; 1377-80
13. Capito C, Echaieb A, Lortat-Jacob S, Pitfalls in the diagnosis and management of obstructive uterovaginal duplication: A series of 32 cases: Pediatrics, 2008; 122; e891-97
14. Tong J, Zhu L, Lang J, Clinical characteristics of 70 patients with Herlyn-Werner-Wunderlich syndrome: Int J Gynecol Obstet, 2013; 121; 173-75
15. Gholoum S, Puligandla PS, Hui T, Management and outcome of patients with combined vaginal septum, bifid uterus, and ipsilateral renal agenesis (Herlyn-Werner-Wunderlich syndrome): J Pediatr Surg, 2006; 41; 987-92
16. Han JH, Lee YS, Im YJ, Clinical implications of Obstructed Hemivagina and Ipsilateral Renal Anomaly (OHVIRA) syndrome in the prepubertal age group: PLoS One, 2016; 11; e0166776
17. Kapczuk K, Friebe Z, Iwaniec K, Kędzia W, Obstructive Müllerian anomalies in menstruating adolescent girls: A report of 22 cases: J Pediatr Adolesc Gynecol, 2018; 31; 252-57
18. Noviello C, Romano M, Nino F, Clinical and radiological findings for early diagnosis of Herlyn-Werner-Wunderlich syndrome in pediatric age: Experience of a single center: Gynecol Endocrinol, 2018; 34; 56-58
19. Zurawin RK, Dietrich JE, Heard MJ, Edwards CL, Didelphic uterus and obstructed hemivagina with renal agenesis: Case report and review of the literature: J Pediatr Adolesc Gynecol, 2004; 17; 137-41
20. Del Vescovo R, Battisti S, Di Paola V, Herlyn-Werner-wunderlich syndrome: MRI findings, radiological guide (two cases and literature review), and differential diagnosis: BMC Med Imaging, 2012; 12; 4
21. Gungor Ugurlucan F, Dural O, Diagnosis, management, and outcome of obstructed hemivagina and ipsilateral renal agenesis (OHVIRA syndrome): Is there a correlation between MRI findings and outcome?: Clin Imaging, 2020; 59; 172-78
22. Fedele L, Motta F, Frontino G, Double uterus with obstructed hemivagina and ipsilateral renal agenesis: Pelvic anatomic variants in 87 cases: Hum Reprod, 2013; 28; 1580-83
23. Santos XM, Dietrich JE, Obstructed hemivagina with ipsilateral renal anomaly: J Pediatr Adolesc Gynecol, 2016; 29; 7-10
24. Haddad B, Barranger E, Paniel BJ, Blind hemivagina: Long-term follow-up and reproductive performance in 42 cases: Hum Reprod, 1999; 14; 1962-64
25. Heinonen PK, Pregnancies in women with uterine malformation, treated obstruction of hemivagina and ipsilateral renal agenesis: Arch Gynecol Obstet, 2013; 287; 975-78
26. Elgohary MA, Naik R, Elkafafi M, Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome: A case report: J Pediatr Surg Case Rep, 2023; 95; 102662
27. Tuqan AR, Salahaldin RR, Abubaker ME, Successful pregnancy in a woman with Herlyn-Werner-Wunderlich syndrome: A case report and literature review: Case Rep Womens Health, 2024; 43; e00647
Figures
Figure 1. Didelphys uterus on pelvic ultrasoundPelvic ultrasound showing 2 separate endometrial cavities, confirming uterine didelphys. The uterus is anteverted and normal in size.Figure 2. Vaginal fluid collection on ultrasoundUltrasound image showing a fluid collection within the vaginal canal measuring 36.0×17.3 mm, indicative of possible obstruction or hematocolpus.Figure 3. Duplicated uterus and vagina on pelvic magnetic resonance imaging (MRI)MRI showing a didelphic uterus with 2 uterine cavities and 2 cervices. A vertically-oriented vaginal septum is also visible, confirming a duplicated vagina and explaining the associated vaginal fluid collection.Figure 4. Solitary left kidney on renal ultrasoundRenal ultrasound showing a single left kidney of normal size (12.40×5.86 cm) and echogenicity. No right kidney is visualized.Figure 5. Ultrasound images(A). Ultrasound showing fetal heart rate of 139 beats per minute within an intrauterine gestational sac. (B) Ultrasound showing placenta attached to the anterior uterine wall. Tables
 Table 1. Laboratory evaluation of hematologic and endocrine function.
Table 1. Laboratory evaluation of hematologic and endocrine function. Table 2. Semen parameters and quality assessment of the patient’s husband.
Table 2. Semen parameters and quality assessment of the patient’s husband. Table 3. Diagnostic and management workflow for OHVIRA syndrome.Table 1. Laboratory evaluation of hematologic and endocrine function.Table 2. Semen parameters and quality assessment of the patient’s husband.Table 3. Diagnostic and management workflow for OHVIRA syndrome.
Table 3. Diagnostic and management workflow for OHVIRA syndrome.Table 1. Laboratory evaluation of hematologic and endocrine function.Table 2. Semen parameters and quality assessment of the patient’s husband.Table 3. Diagnostic and management workflow for OHVIRA syndrome. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133