14 May 2025: Case Reports 
Understanding Brugada Pattern in Elderly Patients with COVID-19: A Case Study
Challenging differential diagnosis, Management of emergency care, Educational Purpose (only if useful for a systematic review or synthesis), Rare coexistence of disease or pathology
Kiera Brigh TurnerDOI: 10.12659/AJCR.948042
Am J Case Rep 2025; 26:e948042






Abstract
BACKGROUND: Brugada syndrome is a hereditary condition characterized by sudden cardiac death or electrocardiogram (EKG)-documented ventricular arrhythmias or arrhythmia-related symptoms in patients without structural cardiac pathology. Brugada phenocopy is a condition with EKG changes consistent with Brugada syndrome, without any hereditary cause. SARS-CoV-2 is a respiratory virus associated with many cardiovascular complications, one of which is new-onset arrhythmia, including Brugada phenocopy or the unmasking of the Brugada syndrome. PPublished cases have revealed the emergence of Brugada pattern among patients with afebrile SARS-CoV-2 infection, suggesting a link with the virus itself and not simply fever. Treatment for Brugada syndrome and Brugada phenocopy involves avoidance of modulating factors that can generate recurrent Brugada patterns. Additional therapy for Brugada syndrome may include implantable cardioverter-defibrillator (ICD) placement, but this treatment was considered unnecessary for a Brugada phenocopy and too risky for a nonagenarian man. Asymptomatic Brugada phenocopy in a COVID-19 patient requires close observation to manage.
CASE REPORT: A nonagenarian man with SARS-CoV-2 infection presented with chest pain, mild fever, and a Brugada pattern on EKG. He was treated with steroids, remdesivir, and antipyretics, before his Brugada phenocopy resolved.
CONCLUSIONS: Brugada phenocopy is characterized by fluctuating ST elevations triggered by modulating factors, including electrolyte derangements, fever, infection, and various medications or drugs. Prompt management of Brugada phenocopy is necessary to avoid the development of malignant arrhythmias or sudden cardiac death. Differentiation of Brugada phenocopy and Brugada syndrome is essential to avoid unnecessary ICD placement for Brugada phenocopy.
Keywords: Brugada syndrome, Cardiology, COVID-19, Humans, Male, Electrocardiography, Aged, 80 and over, SARS-CoV-2
Introduction
Brugada syndrome is a hereditary condition characterized by sudden cardiac death or ventricular arrhythmias in patients without structural cardiac pathology [1]. This condition is more prevalent in male than female patients [1]. Patients often have a familial history of sudden early cardiac death, and many have genetic mutations in cardiac ion channels [2]. About 30% of patients with Brugada syndrome have identified causative genetic mutations, most often in
Diagnosis of Brugada syndrome depends on specific electrocardiogram (EKG) changes in conjunction with ventricular arrhythmias or arrhythmia-related symptoms [1]. Brugada phenocopy describes EKG changes consistent with Brugada syndrome that occur in a patient without the hereditary condition, and are from a reversible cause, most often an electrolyte derangement such as hypokalemia [3]. These EKG changes can occur spontaneously in Brugada syndrome, or they can be unmasked by modulating factors, including bradycardia, sodium channel blockers, cocaine, tricyclic antidepressants, fluoxetine, or fever [1]. Brugada syndrome can be diagnosed by inducing EKG changes with flecainide or other sodium channel blockers [1]. EKG changes induced by any other modulating factor could be unmasked Brugada syndrome or Brugada phenocopy, without any genetic predisposition [3].
Management of Brugada syndrome and Brugada phenocopy includes avoiding these possible triggers and taking antipyretics when febrile. Implantable cardioverter-defibrillators (ICDs) are recommended for patients with subtype 1 Brugada syndrome who have also experienced syncope, sudden cardiac death, or agonal nocturnal respiration [1]. Asymptomatic patients with spontaneous Brugada syndrome may also undergo ICD placement, pending an electrophysiology study [1]. Patients with Brugada phenocopy are not recommended to have ICDs placed, because their elevated risk of sudden cardiac death does not persist when the reversible cause is resolved [4].
The prognosis of Brugada syndrome or phenocopy depends on its etiology. Fatal arrhythmias are more common with spontaneous or fever-induced Brugada syndrome, while drug-induced Brugada syndrome typically has a more benign course [5].
Although SARS-CoV-2 is well-known as a respiratory virus, established studies have revealed how this virus directly affects the cardiovascular system, including cases of myocardial infarction, heart failure, myocarditis, and arrhythmia [6]. The mechanism of myocardial injury for patients with COVID-19, the disease caused by SARS-CoV-2 infection, can be due to direct viral damage to the myocardium, systemic inflammation, or hypoxia, although the exact mechanism is not yet known [7].
New-onset arrhythmia is also linked to SARS-CoV-2 infection [8]. However, the arrhythmogenic potential of SARS-CoV-2 is controversial because fever is present in 88.7% of patients with this virus, and there is extensive evidence of fever inciting arrhythmias [2]. Whether this effect is due to fever alone or the virus itself, there are many reported cases of COVID-19 unmasking patients with arrhythmogenic syndromes, such as Brugada syndrome, long QT syndrome, and catecholaminergic polymorphic ventricular tachycardia [6]. While there are several published cases of COVID-19 with fever unmasking Brugada pattern, there are also a few demonstrating Brugada pattern in patients with afebrile SARS-CoV-2 infection, suggesting a connection separate from fever alone [9].
We present a case of a nonagenarian man with SARS-CoV-2 infection and mild fever presenting with cough, chest pain, and Brugada pattern on EKG. This case suggests a correlation between COVID-19 with minimal fever and Brugada phenocopy in a patient with no prior history of Brugada despite his advanced age.
Case Report
This case examines a nonagenarian man with a past medical history of hypertension, hyperlipidemia, chronic kidney disease, and dementia who presented with intermittent chest pain and cough. His family medical history was negative for arrhythmias or sudden death. He had been evaluated in the Emergency Department (ED) 2 days prior, at which time SARS-CoV-2 infection had been diagnosed. He had been in sinus rhythm and was discharged home without admission. He developed intermittent chest pains at home lasting for 1 h before he returned to the ED with ST-segment elevation myocardial infarction alert (STEMI). The emergency medical services team performed an EKG, which showed apparent ST-segment elevations. A repeat EKG done in the ED confirmed these changes (Figure 1).
His vital signs were within normal limits, apart from a mild fever of 38°C. His physical examination was otherwise benign, with no obvious murmurs identified. His troponin levels were negative, and his SARS-CoV-2 test result was positive. A comprehensive metabolic panel showed no electrolyte derangements. A chest X-ray was unremarkable. His echocardiogram showed a left ventricular ejection fraction of 55% to 59%, with mild mitral regurgitation and no other structural heart abnormalities. His chest pain and fever resolved with acetaminophen in the ED, and he was admitted to a medical floor for further evaluation and treatment.
The inpatient Cardiology Department was consulted, and his EKG changes were identified as a Brugada pattern rather than an acute coronary syndrome or myocarditis, due to negative serial troponin levels, without any structural changes on echocardiography. His chest pain was attributed to musculoskeletal strain from coughing, and he did not undergo any further ischemic evaluation. Inflammatory markers, including C-reactive protein and erythrocyte sedimentation rate, were not measured, because there was low clinical suspicion for pericarditis in a patient with non-pleuritic chest pain that resolved with acetaminophen, and any elevation in these markers could be attributed to acute SARS-CoV-2 infection. Similar EKG changes can also be caused by electrolyte derangements, which were not present in this case.
The SARS-CoV-2 infection was treated with dexamethasone, remdesivir, and supportive care. A repeat EKG done on the third day of admission showed resolution of Brugada pattern (Figure 2), consistent with Brugada phenocopy. The patient declined further workup, including genetic testing. He was discharged home from the hospital.
Discussion
Brugada syndrome or phenocopy can result in 3 distinct subtypes based on EKG findings. Type 1 (coved type), which has ECG tracings of a ≥2-mm ST-segment elevation in one or more leads (V1 to V3), followed by an inverted T wave (Figure 3). This type is the only one that is diagnostic for Brugada syndrome in an asymptomatic patient without other arrhythmias or sudden cardiac death [1]. Type 2 (saddle-back type) has ≥0.5-mm ST-segment elevation in one or more precordial leads, followed by a saddle-back morphology to the ST elevation (Figure 3). Type 3 can show either coved or saddle-back; however, it is consistent with a <2-mm ST-segment elevation (Figure 3).
This patient had a subtype 1 Brugada pattern on his EKG, which would be diagnostic for Brugada syndrome if a hereditary cause was present, without needing any additional factors, such as ventricular arrhythmia, cardiac death, or cardiac symptoms [1]. Brugada syndrome is characterized by incomplete penetrance and variable expressivity [1]. Therefore, a known family history of Brugada syndrome, sudden cardiac death, or malignant arrhythmias is not necessary for a diagnosis. When a reversible modulating factor is present, such as ischemia, drugs, electrolyte abnormalities, or fevers, the presence or absence of a hereditary component for the patient’s condition makes the determination between a diagnosis of Brugada phenocopy or unmasked Brugada syndrome [3].
In the present case, the patient had no known family medical history that would suggest the possibility of Brugada syndrome, so he had not received any testing for this condition earlier in life. During this admission, the patient was offered genetic testing to evaluate for potential
Brugada syndrome is a sodium channelopathy, and about 30% of these patients have mutations in
The most appropriate treatment for Brugada phenocopy is resolution of its reversible cause, including reperfusion after ischemia, cessation of a culprit drug or medication, correction of electrolyte abnormalities, or antipyretic therapy [4]. In this case, the patient’s SARS-CoV-2 infection was treated with supportive care and antipyretic therapy inpatient for 1 day before he had a repeat EKG performed, which revealed resolution of Brugada phenocopy in normal sinus rhythm. If a repeat EKG had been done on admission shortly after his fever had resolved, this test may have provided more evidence toward the cause of his Brugada phenocopy being either fever or SARS-CoV-2. This patient was advised to avoid sick contacts, mask appropriately, and use over-the-counter antipyretics as needed to prevent recurrent Brugada phenocopy.
The main difference in treatment between Brugada phenocopy and unmasked Brugada syndrome is ICD placement [4]. ICDs are recommended for symptomatic patients with type 1 Brugada pattern with symptoms defined as cardiac arrest or syncope, neither of which this patient experienced [1]. ICD can also be considered for asymptomatic patients, following an electrophysiology study [1]. For patients with Brugada phenocopy, their risk of sudden cardiac death is not significantly elevated after their reversible cause is corrected [4]. Therefore, ICD placement is unnecessary for Brugada phenocopy, and this intervention would have been especially high risk for this nonagenarian patient. Differentiating between Brugada phenocopy and Brugada syndrome is vital when Brugada EKG pattern is present, because a mistaken diagnosis can lead to unnecessary or missed ICD implantation.
Conclusions
Brugada phenocopy can be incited by many modulating factors, including fevers and SARS-CoV-2 infection. Close attention to electrolytes, medications, and familial history is important for a patient with asymptomatic Brugada pattern, to differentiate between Brugada syndrome and Brugada phenocopy to avoid unnecessary ICD implantation, especially in an elderly population.
Figures
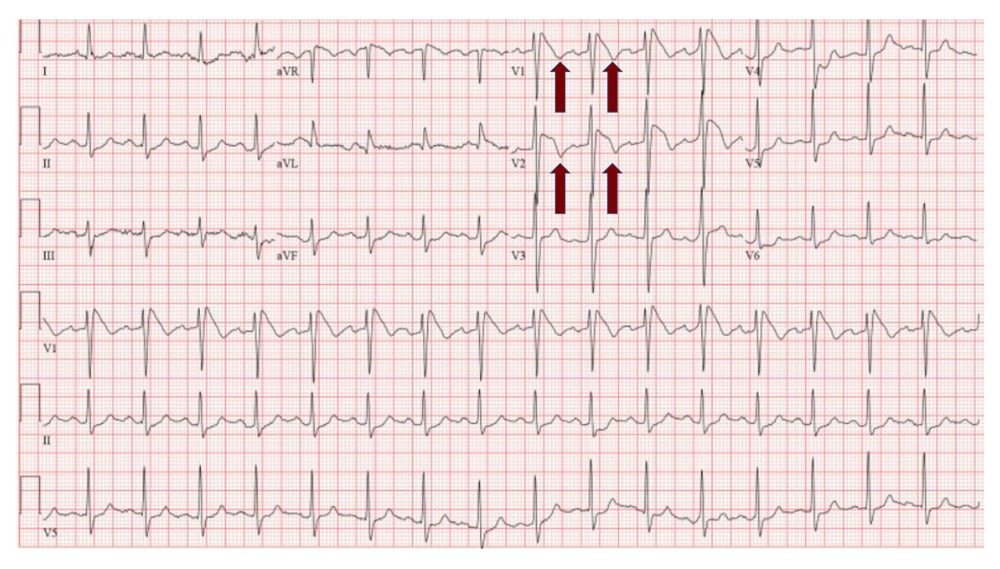 Figure 1. Electrocardiogram on admission showing ST elevation in leads V1 and V2 with inverted T waves.
Figure 1. Electrocardiogram on admission showing ST elevation in leads V1 and V2 with inverted T waves. 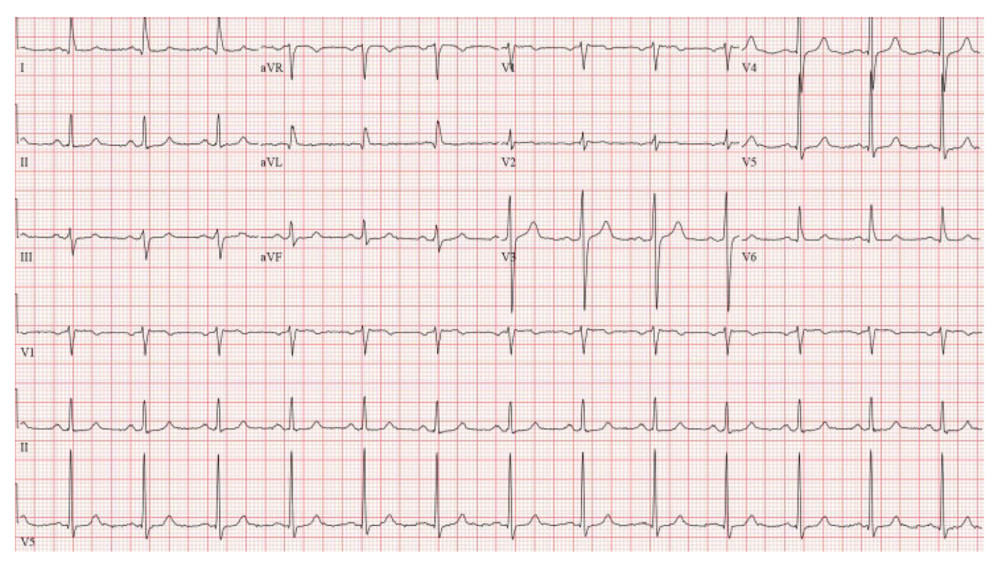 Figure 2. Electrocardiogram pathology resolved, and at discharge the patient had normal sinus rhythm.
Figure 2. Electrocardiogram pathology resolved, and at discharge the patient had normal sinus rhythm. 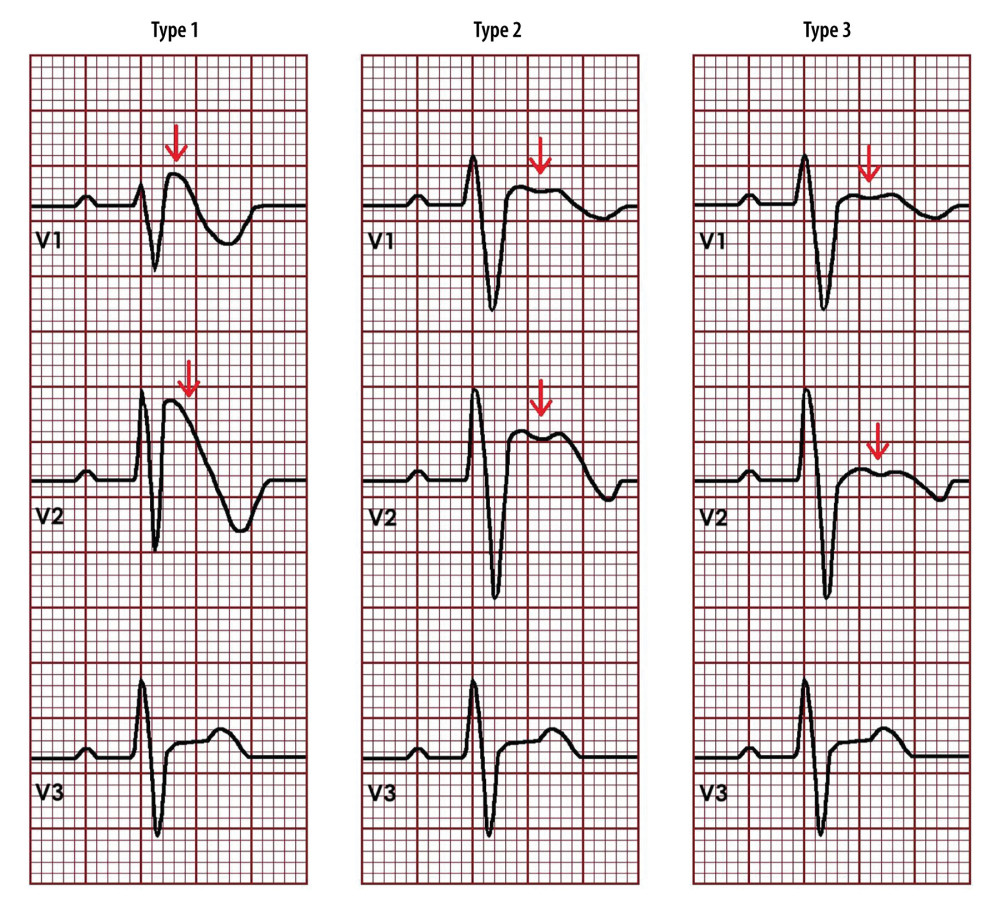 Figure 3. Schematic of Brugada pattern subtypes. Subtype 1 shows a coved ST segment elevation at the thick red line of ≥2-mm in one or more chest leads (V1 to V3), followed by an inverted T wave. Subtype 2 has ≥0.5-mm ST-segment elevation in one or more precordial leads, followed by a saddle-back morphology (thick red arrow) to the ST elevation. Subtype 3 can demonstrate either coved or saddleback (thin red line) morphology, but it is consistently <2-mm ST-segment elevation.
Figure 3. Schematic of Brugada pattern subtypes. Subtype 1 shows a coved ST segment elevation at the thick red line of ≥2-mm in one or more chest leads (V1 to V3), followed by an inverted T wave. Subtype 2 has ≥0.5-mm ST-segment elevation in one or more precordial leads, followed by a saddle-back morphology (thick red arrow) to the ST elevation. Subtype 3 can demonstrate either coved or saddleback (thin red line) morphology, but it is consistently <2-mm ST-segment elevation. References
1. Brugada J, Campuzano O, Arbelo E, Sarquella-Brugada G, Brugada R, Present status of Brugada syndrome: JACC state-of-the-art review: J Am Coll Cardiol, 2018; 72; 1046-59
2. Wu C-I, Postema PG, Arbelo E, SARS-CoV-2, COVID-19, and inherited arrhythmia syndromes: Heart Rhythm, 2020; 17; 1456-62
3. Baranchuk A, Nguyen T, Ryu MH, Brugada phenocopy: New terminology and proposed classification: Ann Noninvasive Electrocardiol, 2012; 17(4); 299-314
4. Adytia GJ, Sutanto H, Brugada phenocopy vs. Brugada syndrome: Delineating the differences for optimal diagnosis and management: Curr Probl Cardiol, 2024; 49(6); 102566
5. Mizusawa Y, Morita H, Adler A, Prognostic significance of fever-induced Brugada syndrome: Heart Rhythm, 2016; 13; 1515-20
6. Adedeji OM, Falk Z, Tracy CM, Batarseh A, Brugada pattern in an afebrile patient with acute COVID-19: BMJ Case Rep, 2021; 14(7); e242632
7. Magadum A, Kishore R, Cardiovascular manifestations of COVID-19 infection: Cells, 2020; 9(11); 2508
8. Kang Y, Chen T, Mui D, Cardiovascular manifestations and treatment considerations in COVID-19: Heart, 2020; 106; 1132-41
9. Zimmermann P, Aberer F, Braun M, The arrhythmogenic face of COVID-19: Brugada ECG pattern in SARS-CoV-2 infection: J Cardiovasc Dev Dis, 2022; 9(4); 96
10. Amin AS, Asghari-Roodsari A, Tan HL, Cardiac sodium channelopathies: Pflugers Arch, 2010; 460(2); 223-37
Figures
Figure 1. Electrocardiogram on admission showing ST elevation in leads V1 and V2 with inverted T waves.Figure 2. Electrocardiogram pathology resolved, and at discharge the patient had normal sinus rhythm.Figure 3. Schematic of Brugada pattern subtypes. Subtype 1 shows a coved ST segment elevation at the thick red line of ≥2-mm in one or more chest leads (V1 to V3), followed by an inverted T wave. Subtype 2 has ≥0.5-mm ST-segment elevation in one or more precordial leads, followed by a saddle-back morphology (thick red arrow) to the ST elevation. Subtype 3 can demonstrate either coved or saddleback (thin red line) morphology, but it is consistently <2-mm ST-segment elevation. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133