23 June 2025: Articles 
Acute Acalculous Cholecystitis in a Child with COVID-19 and Influenza B: A Case Report
Unusual clinical course, Mistake in diagnosis
Abdul Khaliq Abdul Jalil ABDEF 1, Nafiza Mat NasirDOI: 10.12659/AJCR.948156
Am J Case Rep 2025; 26:e948156






Abstract
BACKGROUND: Acute acalculous cholecystitis (AAC) is a rare pediatric condition marked by gallbladder inflammation without gallstones. In children, symptoms are non-specific, making diagnosis and management challenging. Imaging, particularly ultrasound or computed tomography (CT) scan, often is the key to detection. Treatment typically involves supportive care and antibiotics, with surgery reserved for severe cases. This report describes the case of a 7-year-old Malaysian boy with a history of COVID-19 and influenza B infection presenting with acute acalculous cholecystitis.
CASE REPORT: A 7-year-old Malaysian boy presented with fever, vomiting, and abdominal pain, initially diagnosed as acute gastroenteritis at primary care clinic. As symptoms worsened, he went to the Emergency Department, where he tested positive for COVID-19 and influenza B and home quarantine was advised. He had another visit the next day in the same hospital and was given symptomatic treatment. On his fourth visit, due to worsening abdominal pain, he was found to have severe transaminitis and coagulopathy. A CT scan revealed AAC, which was managed conservatively. Treatment with intravenous immunoglobulin (IVIG) therapy led to marked clinical and biochemical improvement within 1 week.
CONCLUSIONS: This case highlights the importance of early identification of complications associated with COVID-19 and influenza B, as conditions such as acute acalculous cholecystitis can present with atypical symptoms in children, making diagnosis more challenging. Prompt recognition and proper referral from primary care settings are vital to prevent diagnostic delays, ensure effective management, and ultimately improve patient outcomes while preventing further complications.
Keywords: COVID-19, gallbladder diseases, general practice, Influenza A virus, Liver Failure, Acute, Pediatrics, Humans, Male, Acalculous Cholecystitis, Child, Influenza, Human, SARS-CoV-2, Tomography, X-Ray Computed, Pandemics, Influenza B virus, Coronavirus Infections, Pneumonia, Viral, Betacoronavirus, Immunoglobulins, Intravenous
Introduction
Acute acalculous cholecystitis is an inflammation of the gallbladder that occurs without the presence of gallstones [1]. In children, acalculous cholecystitis is the most common form of acute cholecystitis, unlike in adults, where gallstone formation is the primary cause of the disease [1]. Acalculous cholecystitis accounts for only 5–10% of all cases of cholecystitis in adults [1].
In acutely ill children, suspicion of acalculous cholecystitis often arises from biochemical abnormalities indicating cholestasis and liver dysfunction [2]. Clinical manifestations in children who can communicate their symptoms include abdominal pain (ranging from mild to severe), typically more intense in the right upper quadrant (RUQ), and fever. These symptoms can present alongside vomiting, diarrhea, jaundice, and hepatosplenomegaly. Jaundice is not always present, leading to a varied clinical presentation [2]. The diagnosis of acalculous cholecystitis is typically made through abdominal ultrasound (US), which may reveal increased gallbladder wall thickness, pericholecystic fluid, and mucosal membrane sludge [3]. A CT scan is preferred when there is concern for an intra-abdominal pathology that may not be adequately visualized on US [3].
Management of acalculous cholecystitis in previously healthy children, where the etiology is often infectious, generally involves conservative measures [1]. Identifying the infectious cause is crucial for prognosis, especially if bacterial, as appropriate antibiotic treatment can significantly improve outcomes [2]. Viral forms of acalculous cholecystitis typically have a better prognosis and are managed conservatively with supportive care, including intravenous fluids, analgesics, and sometimes antibiotics, until viral confirmation is established [1]. Distinguishing between bacterial and viral acalculous cholecystitis based on laboratory and ultrasound findings alone is challenging, as both can show overlapping features such as leukocytosis and elevated inflammatory markers [4]. Liver enzyme alterations are also commonly observed in all cases of acalculous cholecystitis [4].
This report describes the case of a 7-year-old Malaysian boy with a history of COVID-19 and influenza B infection presenting with acute acalculous cholecystitis, experiencing symptoms of acute gastroenteritis. Despite multiple visits to healthcare centers, the symptoms were initially attributed to a viral infection and did not prompt further investigation. It was only when the symptoms worsened, resulting in dehydration, that blood tests uncovered biochemical abnormalities.
Case Report
A 7-year-old boy with no known medical illness presented with a 2-day history of fever, vomiting, abdominal pain, and reduce oral intake. The pain was over the epigastric area and right upper quadrant. It was pricking in nature. He did not have any loose stool or any contacts with people with similar symptoms. He was brought to a primary care clinic and was diagnosed with uncomplicated acute gastroenteritis and given symptomatic treatment. As the fever and abdominal discomfort persisted, he then went to the Emergency Department on the next day. A nasopharyngeal swab-PCR and influenza antigen test was positive for SARS-CoV-2 and influenza B infection. A complete blood count did not show any problems. He was diagnosed with COVID-19 with concomitant influenza B and home quarantine was advised. He had another visit to the Emergency Department a few days later due to reduced oral intake, abdominal discomfort, and loose stool. He was again diagnosed with acute gastroenteritis, advised to increase fluid intake, and to quarantine at home, as upon assessment he did not have any signs of dehydration or warning signs to warrant admission. He came to the Emergency Department again a few days later with lethargy and worsening abdominal pain. Clinically, he looked septic but was not tachypneic or jaundiced. His tongue appeared dry and coated. His oral temperature was 36.7°C, oxygen saturation was 97% on room air, respiratory rate was 19 breaths per minute, and his pulse was regular at 103 beats per minute, with no radio-radial delay. He had abdominal guarding with tenderness over the right hypochondriac region, and the liver was palpable 5 cm below the costal margin. Otherwise, examination of other system showed no abnormalities.
An abdominal X-ray was performed, which showed an enlarged liver. No bowel dilatation or pneumoperitoneum was noted. The following blood tests were ordered: full blood count (FBC), C-reactive protein (CRP), renal profile (RP), and liver function tests (LFT). At this point in time, the differential diagnosis considered was suspected perforated viscus with 10% dehydration.
Oral intake was stopped and he was given hydration for maintenance and correction. An hour later, the laboratory investigations showed a white cell count (WCC) of 24×103 (4.0–10.0×103/μL), Hb 14 (13.0–17.0 g/dL), and platelet count 476 (150–410×109/L). The venous blood gas analysis showed pH 7.46 (7.32–7.42), pCO2 30 (38–52 mmHg), HC03 21 (19–25 mEg/L), Na 130 (136–145 mmol/L), K 3.7 (3.5–5.1 mmol/L), glucose 6.5 (3.5–6.0 mmol/L), and lactate 2 (≤2 mmol/L). A bedside scan was done, which revealed free fluids at the rectovesical, thickened gallbladder wall, and pericholecystic collection with associated sonographic Murphy sign. The inferior vena cava was flat, with no stones seen. The lung scan was A-profile with no effusion. A cardiac scan showed good contractility with no pericardial effusion.
He was given intravenous (i.v.) morphine 1 mg STAT, i.v. cefoperazone 1 g twice a day, and i.v. metronidazole 315 mg 3 times a day based on his bodyweight. The case was reviewed by the surgical team, with the impression of perforated viscus. Blood investigation review showed ammonia 76 (11–32 umol/L) and D-Dimer 9060 (<250 μg/ml). The coagulation profile was PT 26.9 (12–14), INR 2.1 (<1.2), APTT 36.7 (25–36) LFT AST 1151 (<37 U/L), ALT 1666, (<50 U/L) ALP 283 (40–129 U/L), and total bilirubin 55 (< 21 umol/L). Viral screening, including assays for hepatitis B, hepatitis C, and Epstein-Barr virus, which are common viral etiologies of transaminitis, yielded negative results. Hepatitis A testing was not performed, as the patient’s presentation was acute, occurring within a 5-day period, which is shorter than the typical course of hepatitis A [5]. Furthermore, there is no documented history of exposure to hepatitis A.
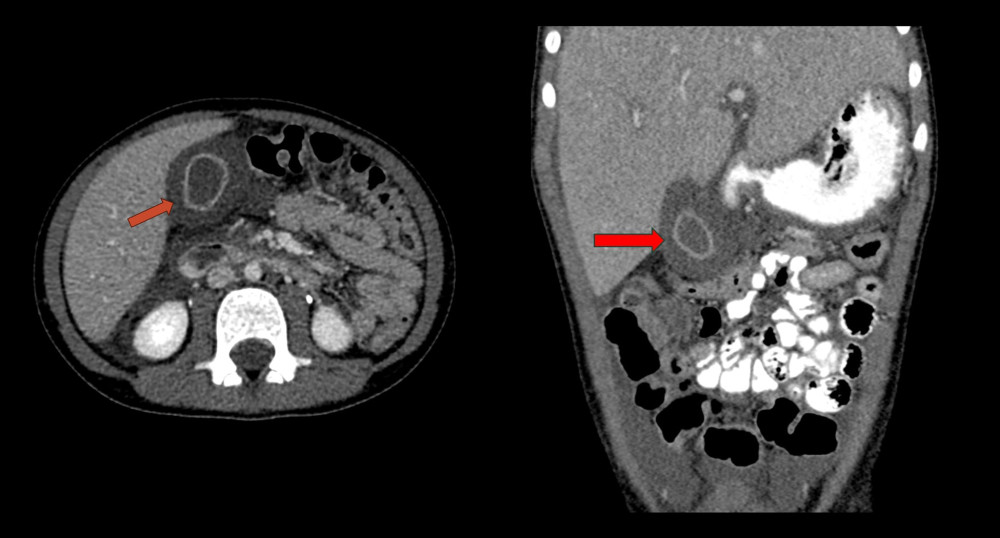
A CT abdomen scan was performed during the same visit due to suspicion of a perforated viscus based on the initial ultrasound findings, showing acalculous cholecystitis with moderate ascites and pleural effusion (Figure 1). There was no evidence of perforated viscus or pneumoperitoneum.
The diagnosis was revised to acalculous cholecystitis with acute hepatitis and impending liver failure likely caused by COVID-19 infection alongside concomitant influenza B. The impending liver failure was considered to be due to isolated elevated INR but without jaundice or encephalopathy. He was admitted to the Intensive Care Unit and received intravenous immunoglobulin following consultation with a pediatric gastroenterologist. During his hospital stay, his condition improved, and his liver enzyme levels showed signs of improvement. He had significant clinical and biochemical improvement with treatment; therefore, a liver biopsy was deemed unnecessary. Laboratory investigations of the patient in the course of hospitalization are presented in Table 1.
After his symptoms resolved and a reassessment confirmed his stable condition, he was discharged after 8 days. He was scheduled for a follow-up appointment in 1 week with appropriate safety precautions. Subsequently, he underwent several follow-up visits and was eventually discharged in good health with no long-term complications.
Discussion
This case highlights the diagnostic challenges commonly encountered by frontline doctors when assessing patients with abdominal pain, particularly in the pediatric population, where symptoms are often non-specific [6]. The symptoms may include abdominal pain, fever, nausea, vomiting, and lethargy, which are not unique to this condition and can be seen in a variety of other gastrointestinal or systemic diseases [6]. They also might present with symptoms such as irritability or generalized discomfort rather than localized right upper-quadrant pain, which can further obscure the diagnosis [6]. This aligns with other reported cases in which an initial alternative diagnosis was made before AAC was accurately identified [7]. In this case, AAC was suspected based on the presence of symptoms and biochemical abnormalities suggestive of cholestatic and liver dysfunction, consistent with findings in previously reported cases [2]. However, jaundice was not present, which is also consistent with other reported instances of AAC associated with COVID-19 [8,9]. Additionally, COVID-19 is a relatively new disease that has been associated with various medical conditions and gastrointestinal manifestation [10,11]. Therefore, maintaining a high index of suspicion for potential complications, especially in children, is crucial. Acute acalculous cholecystitis (AAC) is the most common type of acute cholecystitis in children, whereas in adults it accounts for only about 5% to 10% of cases. In the pediatric population, AAC is estimated to account for at least 50–70% of all acute cholecystitis cases [1]. The causes of acalculous cholecystitis in children are usually secondary to systemic illness or other underlying conditions. Common causes include bacterial, viral, and parasitic infection. Other causes are critical illness such as sepsis and immune-mediated disorders [1].
There have been multiple reports of acute acalculous cholecystitis (AAC) in patients with COVID-19. Several hypotheses have been proposed to explain the potential link between SARS-CoV-2 infection and AAC. One such theory suggests that immune system alterations triggered by the virus, along with the ensuing systemic inflammation and its treatment, can activate proinflammatory pathways, leading to delayed-onset cholecystitis [12]. Additionally, the coagulopathy and prothrombotic state induced by SARS-CoV-2 can result in small-vessel thrombosis and ischemia of the gallbladder wall [13]. The pathogenesis of AAC in the context of COVID-19 remains incompletely understood, and further research is necessary to clarify the impact of SARS-CoV-2 on the hepato-biliary system [14].
In such cases, imaging can be challenging. Acalculous cholecystitis is diagnosed by imaging such as ultrasound, which is the initial imaging modality of choice and may show gallbladder wall thickening or pericholecystic fluid [15]. However, it does not always show clear signs of acalculous cholecystitis, as the sensitivity is equal to or greater than 80% for AAC, while CT scans are reported to have a sensitivity close to 90% [15]. In this case, an ultrasound performed in the Emergency Department revealed gallbladder distension with free fluid, raising the suspicion of a possible perforated viscus. Consequently, a CT abdomen scan was conducted to identify other potential pathologies, in line with findings reported in similar cases [3]. Additionally, younger children might not cooperate fully during imaging studies, leading to suboptimal results [16]. As ultrasound imaging might be inconclusive in some cases, patients might need a more advanced imaging techniques such as computed tomography (CT) scan or even magnetic resonance imaging (MRI) if necessary [17]. These are not always readily available and may require sedation in young children, posing further challenges [16]. Given these challenges, a high index of suspicion and a thorough evaluation are necessary when a child presents with compatible symptoms.
Treatment of AAC in adults is predominantly surgical, typically involving cholecystectomy. However, as previously reported, the epidemiology and etiology of pediatric AAC differ significantly from those in adults. Consequently, the therapeutic approach in children also varies, with surgical intervention being less commonly required compared to in adults or children with ACC, and management of AAC in children is usually conservative [1]. While most cases of acute calculous cholecystitis (ACC) in children are managed conservatively with appropriate antibiotics [2,8,14], our patient developed acute hepatitis with deranged coagulation parameters, raising the concern for impending liver failure. Therefore, intravenous immunoglobulin (IVIG) was administered as part of the treatment. As shown in Table 1, there was a marked improvement in his biochemical markers and clinical condition following the therapy. Multidisciplinary collaboration, including input from pediatric surgeons, radiologists, and gastroenterologists, often plays a critical role in the accurate and timely diagnosis of acalculous cholecystitis in children.
Conclusions
This case report shows the diagnostic challenges faced by healthcare providers when evaluating pediatric patients with abdominal pain, particularly in diagnosing acute acalculous cholecystitis. The condition presents with vague, non-specific symptoms that can mimic other common illnesses, making early identification difficult. Additionally, imaging challenges, such as suboptimal ultrasound results and the need for advanced imaging techniques, further complicate diagnosis. The lack of physician awareness about acalculous cholecystitis in children can lead to delays in diagnosis and poorer outcomes. A high index of suspicion, thorough evaluation, and collaboration among multidisciplinary teams are essential for timely and accurate diagnosis, ensuring better patient outcomes.

References
1. Poddighe D, Sazonov V, Acute acalculous cholecystitis in children: World J Gastroenterol, 2018; 24(43); 4870-79
2. Poddighe D, Cagnoli G, Mastricci N, Bruni P, Acute acalculous cholecystitis associated with severe EBV hepatitis in an immunocompetent child: BMJ Case Rep, 2014; 2014; bcr2013201166
3. Huffman JL, Schenker S, Acute acalculous cholecystitis: A review: Clin Gastroenterol Hepatol, 2010; 8(1); 15-22
4. Poddighe D, Tresoldi M, Licari A, Marseglia GL, Acalculous acute cholecystitis in previously healthy children: General overview and analysis of pediatric infectious cases: Int J Hepatol, 2015; 2015; 459608
5. Girish V, Grant LM, John S, Hepatitis A: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing [Updated 2024 Oct 6]
6. Reust CE, Williams A, Acute abdominal pain in children: Am Fam Physician, 2016; 93(10); 830-36
7. Simões AS, Marinhas A, Coelho P, Ferreira S, Acalculous acute cholecystitis during the course of an enteroviral infection: BMJ Case Rep, 2019; 12(4); e228306
8. D’Introno A, Gatti P, Manca G, Acute acalculous cholecystitis as an early manifestation of COVID-19: Case report and literature review: Acta Biomed, 2022; 93(S1); e2022207
9. Mattone E, Sofia M, Schembari E, Acute acalculous cholecystitis on a COVID-19 patient: A case report: Ann Med Surg (Lond), 2020; 58; 73-75
10. Bourgonje AR, Abdulle AE, Timens W, Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19): J Pathol, 2020; 251(3); 228-48
11. Silva FAFD, Brito BB, Santos MLC, COVID-19 gastrointestinal manifestations: A systematic review: Rev Soc Bras Med Trop, 2020; 53; e20200714
12. Lovece A, Asti E, Bruni B, Bonavina L, Subtotal laparoscopic cholecystectomy for gangrenous gallbladder during recovery from COVID-19 pneumonia: Int J Surg Case Rep, 2020; 72; 335-38
13. Bruni A, Garofalo E, Zuccalà V, Histopathological findings in a COVID-19 patient affected by ischemic gangrenous cholecystitis: World J Emerg Surg, 2020; 15(1); 43
14. Thomaidou E, Karlafti E, Didagelos M, Acalculous cholecystitis in COVID-19 patients: A narrative review: Viruses, 2024; 16(3); 455
15. Shafiq M, Zafar Y, Acute acalculous cholecystitis in the setting of negative ultrasound and computed tomography scan of the abdomen: Cureus, 2018; 10(2); e2243
16. Thukral BB, Problems and preferences in pediatric imaging: Indian J Radiol Imaging, 2015; 25(4); 359-64
17. Wee NK, Cheong WSC, Low HM, CT and MRI findings of acute calculous cholecystitis and its complications in Singapore: A pictorial review: Med J Malaysia, 2021; 76(5); 706-13
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952107
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952658
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953243
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952989
Most Viewed Current Articles
07 Dec 2021 : Case report
22,640,312
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,831
174,831
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,997
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,925
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133