19 June 2025: Articles 
Surgical Outcomes of Right Traumatic Diaphragmatic Rupture with Grade 3 Liver Injury: A Report of 2 Cases
Challenging differential diagnosis, Management of emergency care, Rare disease, Educational Purpose (only if useful for a systematic review or synthesis), Rare coexistence of disease or pathology
Fatima M. AlSinanDOI: 10.12659/AJCR.948238
Am J Case Rep 2025; 26:e948238






Abstract
BACKGROUND: Traumatic diaphragmatic rupture (TDR) is a rare entity. Its diagnosis can be challenging due to its nonspecific clinical presentation. Therefore, diagnosis is often late or missed. This article presents 2 cases of right-sided TDR accompanied by intrathoracic herniation of the liver.
CASE REPORT: Case 1: A 42-year-old male construction worker sustained an injury caused by a falling metallic frame. Upon presentation, he had a paradoxical breathing pattern. The initial chest radiograph showed multiple right-sided rib fractures and pneumohemothorax drained by a thoracostomy tube. A computed tomography scan (CT scan) showed right hemi-diaphragmatic rupture accompanied by intrathoracic herniation of the liver and grade 3 liver injury. Case 2: A 22-year-old man sustained a crush injury. A chest X-ray (CXR) delineated a loop of bowel within the right hemithorax. A CT scan confirmed the diagnosis of right hemi-diaphragmatic rupture with herniation of the right hepatic lobe, hepatic flexure of colon into the right hemithorax, and grade 3 liver injury. Both patients underwent successful immediate emergency laparotomy and primary repair of the diaphragmatic injury.
CONCLUSIONS: TDR is a rare trauma entity that is difficult to recognize clinically and radiologically. Accurate diagnosis is crucial to establish the appropriate and immediate surgical management plan.
Keywords: diaphragmatic rupture, liver injury, Hepatothorax, Humans, Male, adult, Hernia, Diaphragmatic, Traumatic, young adult, Rupture, Liver, Diaphragm, Tomography, X-Ray Computed
Introduction
Traumatic diaphragmatic rupture (TDR) resulting from blunt thoraco-abdominal trauma is a rare entity. The incidence of TDR cannot be accurately estimated in the literature, as most patients have an indolent, delayed presentation [1]. However, its incidence has increased rapidly in the last few years, accounting for around 7–15% of all trauma patients [2,3]. The right side is less commonly affected, as it is protected by the anatomical location of the liver, which plays an important role in protecting the right hemidiaphragm. Therefore, diagnosis of right-sided TDR can be challenging, as patients are often asymptomatic and present late [1,4]. This delay in diagnosis exposes patients to complications, organ herniation, pulmonary dysfunction, and cardiovascular compromise. A higher mortality rate was observed in TDR patients with liver injury [5]. Computed tomography (CT) scans make diagnosis more feasible, with a high sensitivity, reaching 80% [6]. Surgical intervention is essential once a diagnosis is made. Herein, we report 2 cases of right-sided TDR accompanied by intrathoracic herniation of the liver. Our patients were diagnosed early, and immediate surgical management was carried out successfully.
Case Reports
CASE 1:
A 42-year-old male construction worker presented to our Emergency Department after sustaining an injury from a falling metallic frame from 3 meters height. Upon initial assessment, he was conscious and alert with a Glasgow coma scale of 13/15, blood pressure (BP) of 113/74 mmHg, pulse rate (PR) of 98 bpm, and oxygen saturation (SpO2) of 100% on 10 L oxygen delivered by a simple face mask. He appeared dyspneic, with an obvious paradoxical breathing pattern. A right hemothorax was treated by the referring hospital by insertion of an intercostal thoracostomy tube fixed in place with an output of 500 cc of blood in an underwater seal drainage system. Chest examination revealed decreased air entry on the right lower zone. Significant laboratory findings were pH 7.11, PCO2 70.8 mmHg, HCO3 16.9 mEq/L, Hgb 11.9g/dL, ALT 492 IU/L, and AST 500 IU/L. Following the Advanced Trauma Life Support (ATLS) protocol, a chest X-ray (CXR) was the first image obtained and showed multiple right-sided rib fractures in addition to pneumohemothorax (Figure 1). Extended focused assessment with sonography for trauma (eFAST) was negative for intra-abdominal bleeding.
A computed tomography (CT) scan revealed multiple displaced and nondisplaced right-sided rib fractures at multiple sites, given the diagnosis of flail chest, accompanied by hemopneumothorax, right hemi-diaphragmatic rupture with liver herniation, and grade 3 liver injury, without active contrast extravasation (Figure 2). The tip of the thoracostomy tube was noted within the liver parenchyma.
The patient was intubated and admitted to the intensive care unit (ICU). After trauma protocol resuscitation with intravenous fluid, he was taken a few hours later to the operating room for an urgent exploratory laparotomy. The decision was made to use an open abdominal approach to ensure better accessibility of the liver injury. Intraoperatively, the right hemidiaphragm was torn apart with a hepatothorax and intrahepatic thoracostomy tube. The tube was removed, and the liver laceration and diaphragm were both repaired primarily. The flail segments of the rib cage was addressed as well, fixed with plates and screws.
On the third postoperative day, the patient was extubated and discharged to the regular surgical ward, where he had an uneventful recovery. He remained recurrence-free on follow-up. Repeated CXR showed a maintained contour of the right dome of the diaphragm, without evidence of disruption or organ herniation.
CASE 2:
A 22-year-old man was referred to our hospital as a case of polytrauma. He sustained the injuries in a collision between a truck and a container. Upon arrival to our Emergency Department, he was conscious, with BP 110/70 mmHg, PR 95 bpm, and SpO2 of 100% on room air. He appeared dyspneic. Auscultation of the chest revealed bowel sounds over the right hemithorax. Initial investigations showed Hgb 12.7 g/dL, total bilirubin 8 umol/L, conjugated bilirubin 3 umol/L, AST 348 IU/L, ALT 413 IU/L, GGT 30 IU/L, ALP 83 IU/L, and INR 0.89. Again, as per ATLS sequence, CXR was obtained, showing a loop of bowel within the right chest, coupled with hemothorax (Figure 3), and eFAST was unremarkable.
A pan CT scan revealed right hemopneumothorax and pulmonary contusion, anterior and lateral rupture of right hemidiaphragm, with herniation of the right hepatic lobe, hepatic flexure of the colon into the right hemithorax, and grade 3 liver injury (Figure 4).
He needed immediate stabilization, for which he underwent exploratory laparotomy. Similar to the first patient, an open abdominal approach was used due to the liver injury. Intraoperatively, we found right hemi-diaphragmatic disruption, herniation of the right lobe of the liver and right colon, and liver injury with no active bleeding. Primary repair of the right hemidiaphragm was done. He was then transferred to the ICU intubated on mechanical ventilation.
His postoperative course was complicated by recurrent pleural effusion, which was managed by re-insertion of a chest tube. He was extubated successfully after 8 days and transferred to the regular ward in stable condition. Magnetic resonance cholangiopancreatography (MRCP) and endoscopic retrograde cholangiopancreatography (ERCP) were negative and excluded the suspicion of biliopleural fistula prior to removal of the chest tube. Subsequently, he was discharged in good health, without evidence of recurrence on follow-up. Follow-up plain X-rays remained normal.
Discussion
Despite the advances in radiographic modalities, diagnosis of right-sided TDR injury remains challenging. In acute trauma settings, CXR is the standard initial image to be obtained as part of the primary survey of the ATLS approach. TDR can be suspected when certain signs are observed, such as elevation of the right hemidiaphragm, intrathoracic herniation of abdominal organs, or recognition of a nasogastric tube tip higher than the level of the diaphragm [7]. However, these findings have low sensitivity and require further imaging. Abdominal ultrasound (US) has a limited role; it can occasionally detect displacement of the liver higher in the thoracic cavity [6,8,9]. Nevertheless, eFAST assessment in trauma patients involves concerns about free intra-abdominal, pericardial, and intrapleural fluid and detection of major injuries. To the best of our knowledge, right-sided diaphragmatic discontinuity was only identified once by using abdominal US, in a case reported by Fung et al [9].
Similar to our patients, hemodynamically stable patients during and after primary survey usually proceed to a pan CT scan. This sequence of imaging investigation is universally accepted by trauma surgeons. Moreover, CT scans for diaphragmatic injuries have a sensitivity and specificity of 50–83% and 100%, respectively. Diagnostic signs include thickening of the right hemidiaphragm, loss of continuity of the right crus, and herniation of the liver and other abdominal viscera into the thoracic cavity. Rees et al described certain signs of right-sided TDR on CT scans: “collar sign” and “dependent viscera sign” [10]. The collar sign is a constriction of the herniated viscera at the site of the diaphragmatic tear. The dependent viscera sign is defined by the posterior position of the herniated viscera against the posterior chest wall. Both of our patients had an apparent liver herniation that confirmed the diagnosis of TDR. Several authors concluded that right-sided diaphragmatic rupture is less likely to be detected on a CT scan if there is no concomitant herniation of abdominal viscera [2,10].
Magnetic resonance imaging (MRI) is advantageous in assessing delayed presentation cases, in which differentiation of the injured diaphragm from other organs is beneficial. A major pitfall is that the diaphragm has same signal intensity as the liver and consolidated lung, rendering it more useful in diagnosing left-sided TDR than right [11,12].
Most trauma surgeons agree that once a diagnosis of diaphragmatic injury is made, surgical intervention is mandatory. The approach and timing of intervention widely vary. Diagnostic laparoscopy or thoracoscopy is indicated when images are inconclusive [2,13]. Surgical management routinely involves the reduction of abdominal organs and repair of the hernial defect, either primarily or with the enforcement of a prosthetic mesh, depending on the size of the defect and timing of presentation. This can be achieved either through open surgeries such as laparotomy/thoracotomy, or a minimally invasive approach with laparoscopy/thoracoscopy [3,6,14,15]. Laparotomy is preferred in patients with acute TDR, where exploration of the abdomen is necessary for evaluation and management of concomitant abdominal injuries, similar to our 2 cases. Thoracotomy is the recommended approach in patients with major thoracic injuries and late presentation, as these patients usually tend to develop adhesions between the herniated viscera and mediastinal structure, making the thoracic approach a safer option. A combined thoracotomy with laparotomy can be done when necessary due to difficult visualization or synchronous thoracic and abdominal injuries [3,16,17]. A minimally invasive repair through laparoscopy or thoracoscopy has been recently reported in the literature, but this is still controversial for acute trauma patients. Laparoscopic repair was used with successful outcomes for patients with delayed presentation of TDR, but it is still technically challenging, mainly due to the difficulty of retracting and mobilizing the liver [15]. Laparoscopy has demonstrated the advantage of shorter hospital stay in comparison to open surgery in a study by Liao et al [18]. There is no standard approach to management, and many successful approaches have been reported in the literature. Ultimately, the choice should be individualized for each patient, depending on clinical situation, time from trauma to presentation, and the surgeon’s experience [3,16]. Concomitant liver injury significantly increases mortality rates, and mortality has been attributed to the severity and concomitance of other trauma-related injuries rather than TDR itself [5,19].
Conclusions
TDR is a rare trauma entity that is difficult to recognize clinically and radiologically. Despite its rarity, accurate diagnosis is crucial to establish the appropriate and immediate surgical management plan. Either a thoracic or abdominal approach may be best for the patient’s condition, and thorough individualized surgical planning is essential for every case.
Figures
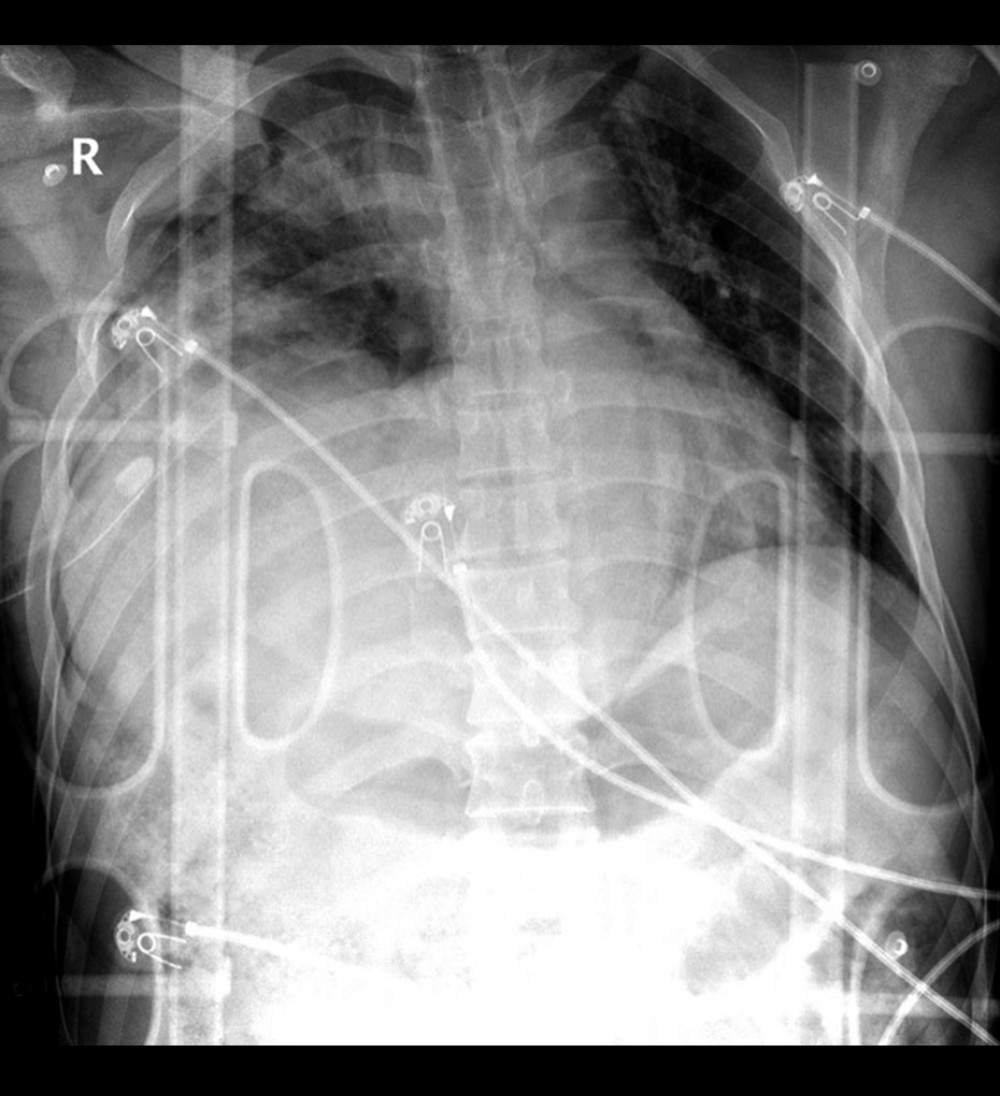 Figure 1. Chest radiograph showing right pneumohemothorax and intercostal chest tube in place. Note: The patient was not positioned well for the film.
Figure 1. Chest radiograph showing right pneumohemothorax and intercostal chest tube in place. Note: The patient was not positioned well for the film. 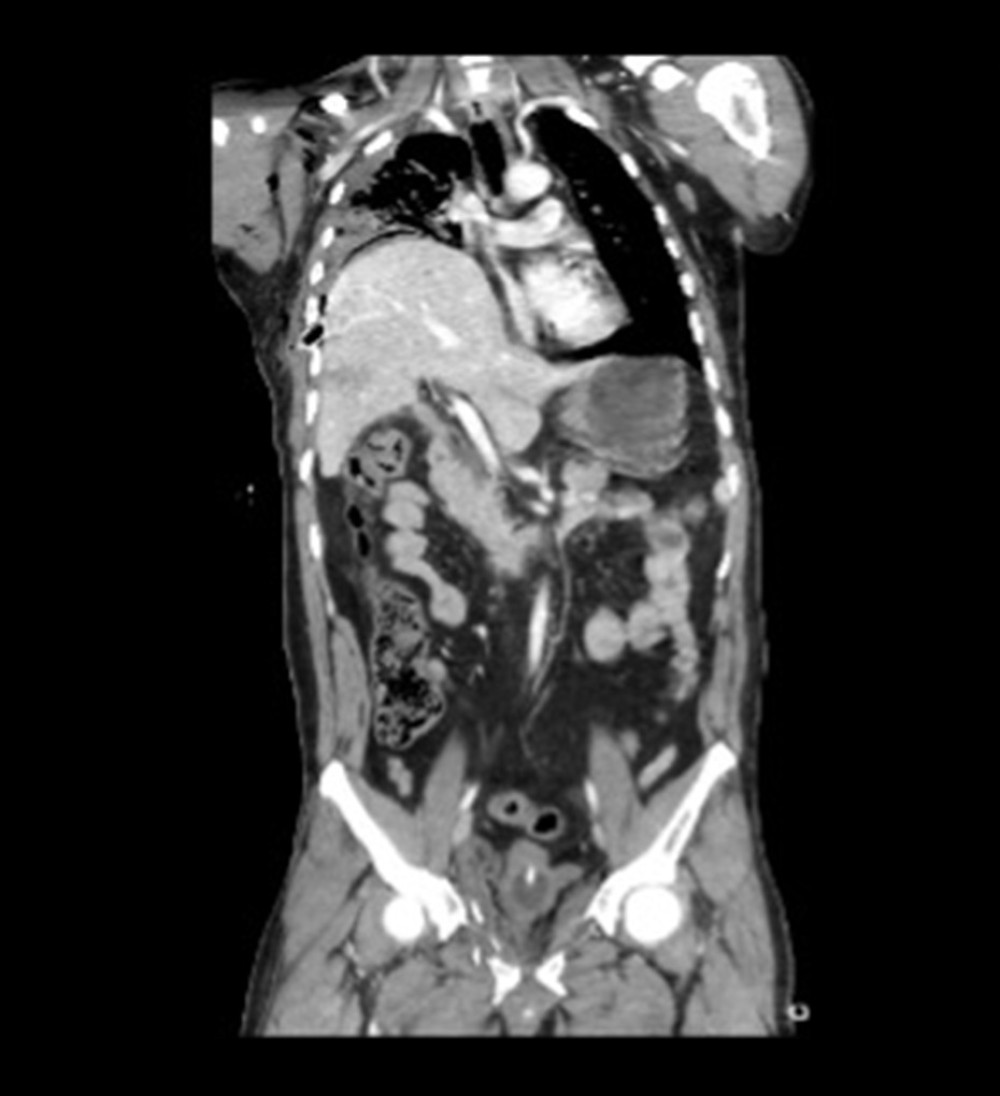 Figure 2. Coronal computed tomography scan showing the herniation of the liver to right hemithorax with intercostal chest tube noted in the liver parenchyma.
Figure 2. Coronal computed tomography scan showing the herniation of the liver to right hemithorax with intercostal chest tube noted in the liver parenchyma. 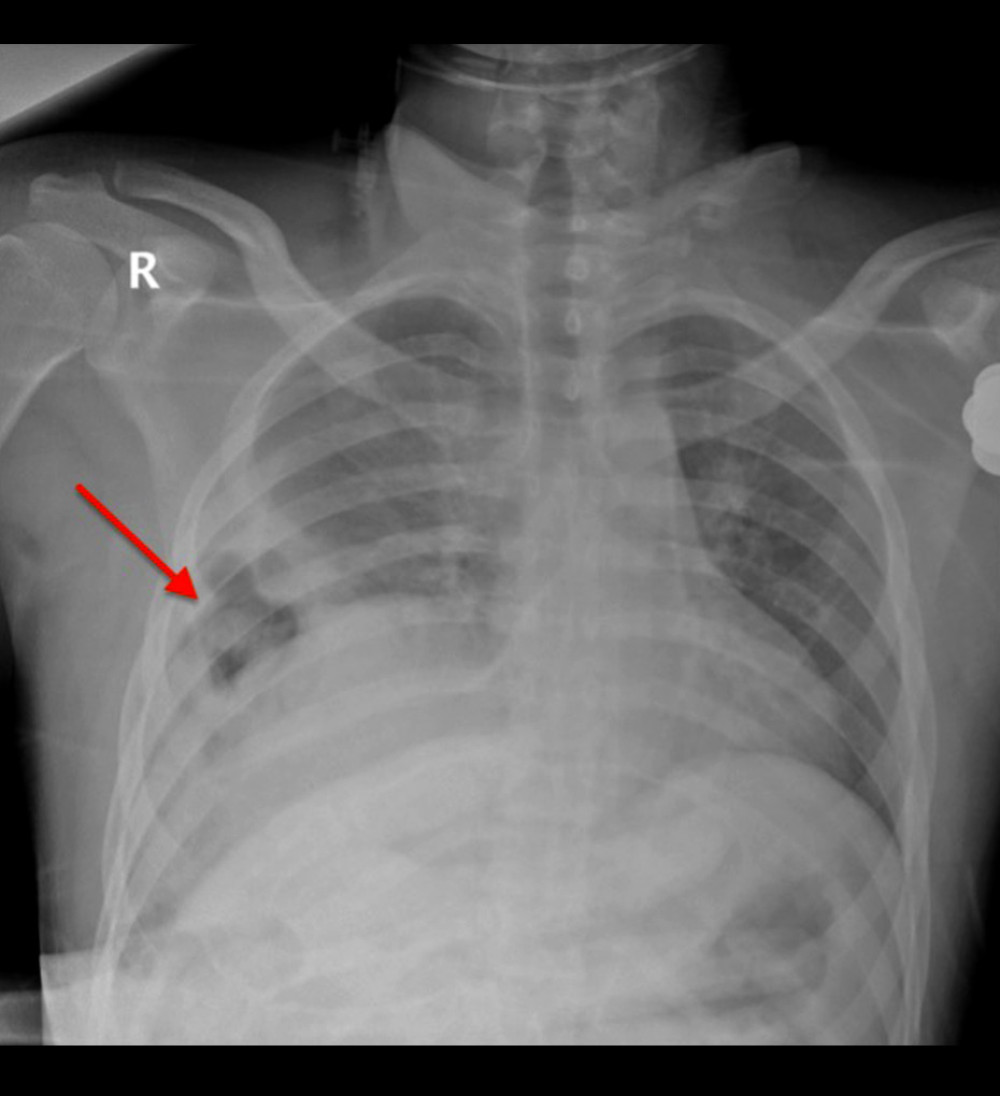 Figure 3. Chest radiograph showing lucent bowel loop (arrow) within the right chest coupled with hemothorax.
Figure 3. Chest radiograph showing lucent bowel loop (arrow) within the right chest coupled with hemothorax. 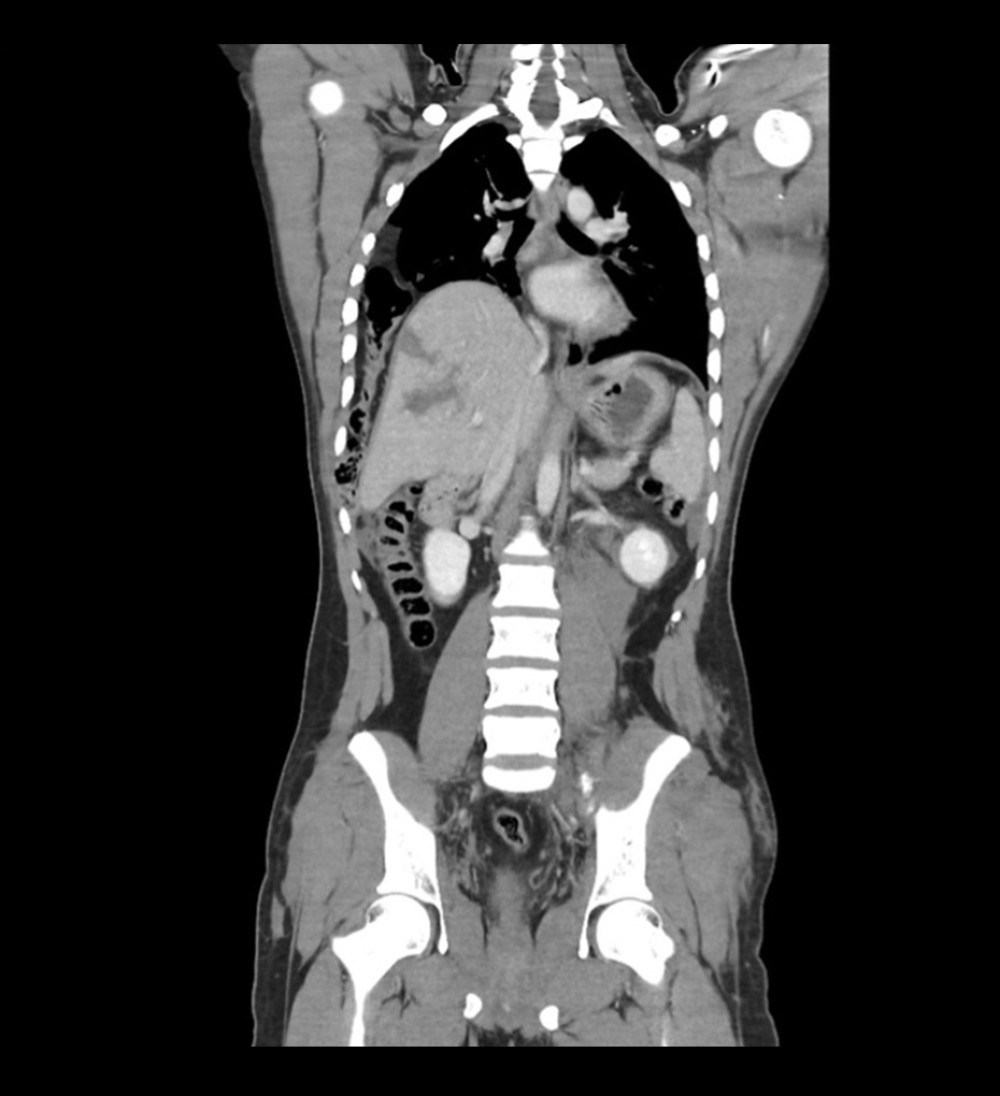 Figure 4. Coronal computed tomography showing herniation of the right hepatic lobe and hepatic flexure of colon to the right hemithorax.
Figure 4. Coronal computed tomography showing herniation of the right hepatic lobe and hepatic flexure of colon to the right hemithorax. References
1. Furák J, Athanassiadi K, Diaphragm and transdiaphragmatic injuries: J Thorac Dis, 2019; 11(Suppl 2); S152-S57
2. Somford MP, Nuytinck HK, Vos DI, A case of delayed diagnosis of a right-sided diaphragm rupture with a review of the literature: Eur J Trauma Emerg Surg, 2009; 35(5); 499-502
3. Igai H, Yokomise H, Kumagai K, Delayed hepatothorax due to right-sided traumatic diaphragmatic rupture: Gen Thorac Cardiovasc Surg, 2007; 55(10); 434-36
4. Rashid F, Chakrabarty MM, Singh R, Iftikhar SY, A review on delayed presentation of diaphragmatic rupture: World J Emerg Surg, 2009; 4; 32
5. Kaya S, Altın Ö, Altuntaş YE, Factors affecting mortality in patients with traumatic diaphragmatic injury: An analysis of 92 cases: Ulus Travma Acil Cerrahi Derg, 2020; 26(1); 80-85
6. Fatima A, Shadin G, Salem A, Incidental traumatic right diaphragmatic rupture: A missed case after trauma: J Trauma Inj, 2023; 36(1); 56-59
7. Vilallonga R, Pastor V, Alvarez L, Right-sided diaphragmatic rupture after blunt trauma. An unusual entity: World J Emerg Surg, 2011; 6; 3
8. De Maeseneer M, Vandendriessche M, Schoofs E, De Hert S, Right diaphragmatic rupture following blunt abdominal injury – a case report: Injury, 1985; 16(6); 389-90
9. Fung HM, Vickar DB, Traumatic rupture of the right hemidiaphragm with hepatic herniation. Real-time ultrasound demonstration: J Ultrasound Med, 1991; 10(5); 295-98
10. Rees O, Mirvis SE, Shanmuganathan K, Multidetector-row CT of right hemidiaphragmatic rupture caused by blunt trauma: A review of 12 cases: Clin Radiol, 2005; 60(12); 1280-89
11. Barbiera F, Nicastro N, Finazzo M, The role of MRI in traumatic rupture of the diaphragm. Our experience in three cases and review of the literature: Radiol Med, 2003; 105(3); 188-94
12. Carter EA, Cleverley JR, Delany DJ, Lea RE, Case report: Cine MRI in the diagnosis of a ruptured right hemidiaphragm: Clin Radiol, 1996; 51(2); 137-40
13. Schummer W, Schummer C, Gottschall R, Schumann M, Delayed diagnosis of right-sided diaphragmatic rupture: Accid Emerg Nurs, 2003; 11(1); 2-4
14. Sato M, Kosaka S, Minimally invasive diagnosis and treatment of traumatic rupture of the right hemidiaphragm with liver herniation: Jpn J Thorac Cardiovasc Surg, 2002; 50(12); 515-17
15. Shichiri K, Imamura K, Takada M, Anbo Y, Minimally invasive repair of right-sided blunt traumatic diaphragmatic injury: BMJ Case Rep, 2020; 13(11); e235870
16. Kozak O, Mentes O, Harlak A, Late presentation of blunt right diaphragmatic rupture (hepatic hernia): Am J Emerg Med, 2008; 26(5); 638e3-5
17. Baldwin M, Dagens A, Sgromo B, Laparoscopic management of a delayed traumatic diaphragmatic rupture complicated by bowel strangulation: J Surg Case Rep, 2014; 2014(7); rju073
18. Liao CH, Chu CH, Wu YT, The feasibility and efficacy of laparoscopic repair for chronic traumatic diaphragmatic herniation: Introduction of a novel technique with literature review: Hernia, 2016; 20(2); 303-9
19. Tokgöz S, Akkoca M, Uçar Y, Factors affecting mortality in traumatic diaphragm ruptures: Ulus Travma Acil Cerrahi Derg, 2019; 25(6); 567-74
Figures
Figure 1. Chest radiograph showing right pneumohemothorax and intercostal chest tube in place. Note: The patient was not positioned well for the film.Figure 2. Coronal computed tomography scan showing the herniation of the liver to right hemithorax with intercostal chest tube noted in the liver parenchyma.Figure 3. Chest radiograph showing lucent bowel loop (arrow) within the right chest coupled with hemothorax.Figure 4. Coronal computed tomography showing herniation of the right hepatic lobe and hepatic flexure of colon to the right hemithorax. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952428
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952854
Most Viewed Current Articles
07 Dec 2021 : Case report  22,760,204
22,760,204
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,117
176,117
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,604
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,593
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133