04 August 2025: Articles 
Visceral Arterial Thrombosis Linked to Long-Term Oral Contraceptives and Smoking: A Case Report
Challenging differential diagnosis, Unusual setting of medical care, Patient complains / malpractice, Rare disease, Clinical situation which can not be reproduced for ethical reasons
Laura Leci Tahiri ABCDEF 1,2, Valdete Haxhibeqiri CDEF 1,3*DOI: 10.12659/AJCR.948398
Am J Case Rep 2025; 26:e948398






Abstract
BACKGROUND: This report describes the case of a 51-year-old woman with a history of smoking and oral contraceptive use presenting with thrombosis of the hepatic, superior mesenteric, splenic, and left renal arteries. Oral contraceptive use is associated with an increased risk of both venous and arterial thrombosis, including visceral arterial thrombosis. This report presents a rare case of extensive visceral arterial thrombosis potentially related to the combined risk factors of long-term oral contraceptive use and long-term smoking.
CASE REPORT: A 51-year-old woman presented with severe abdominal pain localized to the epigastrium and left flank pain, nausea, vomiting, and fever persisting for over 24 hours. Contrast-enhanced computed tomography (CT) revealed extensive thrombosis involving the hepatic, superior mesenteric, splenic, and left renal arteries. She had a 20-year history of continuous oral contraceptive use and long-term smoking but did not have a family history or laboratory evidence of a hypercoagulable disorder. She was treated successfully with anticoagulation and supportive care despite complications from heparin-induced thrombocytopenia (HIT).
CONCLUSIONS: This case illustrates the increased risk of extensive visceral arterial thrombosis in women using second-generation oral contraceptives and who are long-term smokers. It emphasizes the diagnostic and therapeutic challenges in managing multifocal visceral arterial thrombosis, particularly when driven by non-genetic, modifiable risk factors. Early recognition and timely initiation of appropriate anticoagulation therapy can lead to favorable outcomes, although clinicians must remain alert to complications such as HIT during treatment.
Keywords: Smoking, Thrombosis, Vasculitis, Humans, Female, Middle Aged, Contraceptives, Oral, Tomography, X-Ray Computed, Renal Artery, Anticoagulants, Risk Factors
Introduction
Multifocal visceral arterial thromboses are extremely rare and carry a high risk of morbidity and mortality. Predisposing factors include hypercoagulable states, malignancies, long-term use of hormonal therapies, and smoking. Many studies have established the use of oral contraceptives as a risk factor for venous and arterial thrombosis. Smoking is recognized as a contributor to both venous and arterial thrombosis. In the case of arterial conditions, smoking has been found to worsen the harmful effects of oral contraceptives [1–4]. Studies comparing coagulation changes in women who smoke and take oral contraceptives with those who do not smoke indicate that coagulation alterations are predominantly observed in smokers. Smoking not only causes direct damage to the blood vessel walls but may also elevate cardiovascular risk by promoting inflammation and raising fibrinogen levels. These processes can result in thrombotic events in arteries and veins [1,4–7]. Additionally, female reproductive hormones – whether produced naturally or supplied externally through contraceptives – can influence the vascular system by promoting thickening of the vessel lining and the formation of blood clots. While the roles of estrogen and progestogen components in contraceptives are important, smoking appears to be a key factor triggering thrombosis in susceptible women, particularly those with pre-existing vessel hyperplasia in visceral arteries [3,5,7–9]. Here, we present a unique case of extensive visceral arterial thrombosis associated with oral contraceptive use and smoking, emphasizing the importance of early diagnosis and multidisciplinary management. This report describes the case of a 51-year-old woman with a history of smoking and oral contraceptive use presenting with thrombosis of the hepatic, superior mesenteric, splenic, and left renal arteries.
Case Report
A 51-year-old woman presented to the Vascular Surgery Clinic with severe abdominal pain localized to the epigastrium and left flank pain, nausea, vomiting, and fever persisting for over 24 hours. She reported a similar episode the day before, partially relieved with analgesics.
She had no history of thromboembolic events, coagulopathy, or autoimmune disease, except for rare episodes of migraines. She also denied any thrombotic disorders in her family members. She had been using a second-generation combined oral contraceptive, Legravan, containing Levonorgestrel 0.15 mg/Ethinylestradiol 0.03 mg, for more than 20 years. Additionally, she was a long-term smoker, averaging over 15 cigarettes per day for the past 30 years. She was allergic to ceftriaxone and ibuprofen. On initial clinical evaluation, she was hemodynamically stable but in significant distress due to abdominal pain. Physical examination revealed diffuse abdominal tenderness without peritoneal signs.
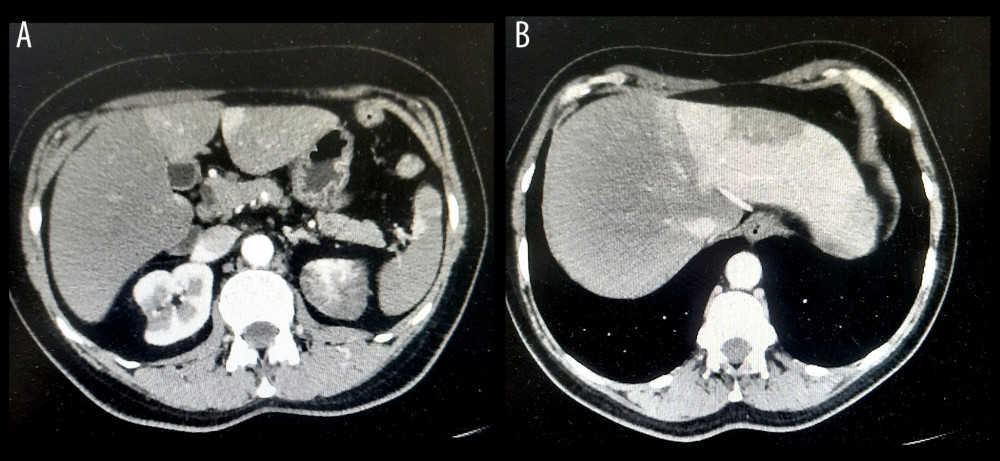
Laboratory tests revealed leukocyte count 23.1×109/L, platelet count 420×109/L, C-reactive protein (CRP) 48 mg/L, urea 7.49 mmol/L, and creatinine 99.9 μmol/L. A native abdominal X-ray showed no abnormalities. Due to the severity of symptoms, a contrast-enhanced CT scan of the abdomen and pelvis was performed, revealing multiple arterial thrombotic events: hepatic artery thrombosis with perfusion limited to the left hepatic lobe; superior mesenteric artery (SMA) thrombosis; evidence of collateral circulation; maintained perfusion in the post-thrombotic segment; splenic artery thrombosis resulting in splenic infarction; left renal artery thrombosis, with thrombus localized at the renal hilum; and a small arterial branch continued to supply a minor portion of the kidney, indicating partial renal infarction. Importantly, no signs of bowel ischemia, perforation, or intra-abdominal free fluid or air were noted (Figure 1).
Upon diagnosis, the patient was immediately started on therapeutic anticoagulation with unfractionated heparin, administered as a bolus of 10 000 IU, followed by 7500 IU every 6 hours. Supportive therapy included intravenous pantoprazole, crystalloid fluids, and analgesics for pain management. Combined oral contraceptives were discontinued immediately upon admission. The patient also reduced her tobacco consumption, though she did not achieve complete smoking cessation. On hospital day 3, she had a sudden and significant drop in platelet count to 34×109/L, raising suspicion for heparin-induced thrombocytopenia (HIT). Heparin was promptly discontinued. Anticoagulation was switched to a direct thrombin inhibitor, Orgaran (danaparoid sodium), 750 U/0.6 mL subcutaneously once daily. Her platelet count steadily improved, reaching 318×109/L by day 11.
Specialist consultations and additional investigations were conducted. Hematology consultation resulted in initiation of oral prednisone, 100 mg daily, for management of thrombocytopenia. Infectious Diseases consultation resulted in empiric broad-spectrum antibiotic therapy with meropenem 1 g IV every 8 hours. Rheumatology and Nephrology consultation resulted in an extensive autoimmune and thrombophilia workup, which returned normal results. Direct and indirect Coombs tests were both negative.
The patient showed rapid clinical improvement, with resolution of abdominal pain within 24 hours of initiating anticoagulation therapy. CRP levels normalized by day 11. After 12 days of treatment with Orgaran, anticoagulation was transitioned to oral rivaroxaban 15 mg once daily for 2 weeks. However, rivaroxaban plasma levels were found to be subtherapeutic, prompting an increase in dosage to 20 mg once daily.
At the 1-month follow-up, the patient remained asymptomatic. Results of repeat biochemical testing, including liver and renal function tests, were all within normal limits. We conducted a comprehensive evaluation for other potential causes of thrombosis, including tests for inherited thrombophilia (Factor V Leiden and prothrombin gene mutation), antiphospholipid syndrome, malignancy, and vasculitis, all of which yielded negative results. The patient remained clinically stable, with no recurrent symptoms or complications. She reported a return to normal daily activities, including work and physical activity, and maintained compliance with anticoagulation and lifestyle modifications.
At 2 months, a follow-up contrast-enhanced CT angiography of the abdominal aorta and visceral branches revealed the following: partial infarction of the spleen with persistent thrombosis in multiple branches of the splenic artery; complete occlusion of the main trunk of the superior mesenteric artery, with recanalization of distal mesenteric branches; compensatory hypertrophy of the inferior mesenteric artery, maintaining mesenteric perfusion; improved perfusion of the left kidney, but with reduced size and function, now compensated by the right kidney; and no new visceral abnormalities or bowel ischemia.
Discussion
In this case study, we found that the combined use of oral contraceptives and long-term smoking increased the overall risk of extensive visceral thrombosis. Abdominal organ infarcts and ischemia can manifest as acute abdominal pain, making early diagnosis essential to reduce morbidity and mortality. Unfortunately, many of these patients arrive at the emergency department in critical condition, highlighting the importance of imaging specialists in achieving the best possible outcomes. CT with intravenous contrast is the primary diagnostic tool for diagnosing and managing infarcts [4,6,10–12].
The effect of smoking is also more pronounced in women than in men. A recent prospective cohort study reported that cigarette smoking is linked to an increased risk of arterial thromboembolic events (ATE) and poorer prognosis in patients with thrombotic antiphospholipid syndrome (TAPS) [3,5,11,13]. An explanation is our finding of a synergistic effect of smoking with oral contraceptive use, which agrees with the results of studies on myocardial infarction done by Tanis et al [2,7]. Studies assessing how oral contraceptives affect blood clotting have found that changes are greatest in women who smoke while using these contraceptives, compared to nonsmokers [5]. The progestogen part of oral contraceptives is likely linked to a higher risk of arterial disease, partly because progestogens can influence blood pressure levels [3,5,9]. Our results are consistent with earlier research showing that the use of oral contraceptives is associated with an increased risk of arterial thrombosis, with the magnitude of this risk closely linked to the ethinyl estradiol dose [2,5,6,9]. In this case, even low-dose oral contraceptives appeared to act as an independent risk factor for visceral arterial thrombosis. Additionally, prior research has shown that young female smokers have a significantly higher risk of acute myocardial infarction, approximately 2–5 times higher when smoking fewer than 10 cigarettes per day, and 5–10 times higher when smoking more than 10 cigarettes per day. Our patient reported smoking more than 15 cigarettes daily, further supporting this dose-dependent relationship and reinforcing the synergistic prothrombotic effect of smoking combined with hormonal contraceptive use [3–6].
An additional layer of complexity in our case was the development of heparin-induced thrombocytopenia (HIT). Heparin-induced thrombocytopenia is an immune-mediated condition associated with high mortality in cardiac surgery patients, even when promptly diagnosed and treated with direct thrombin inhibitors [14–17]. In our patient, timely recognition and a switch to danaparoid sodium (Orgaran), a direct thrombin inhibitor, resulted in a successful clinical outcome. Transitioning to an alternative anticoagulation regimen was critical to prevent further thrombosis.
All these factors likely predisposed the patient to multifocal visceral arterial thromboses. Hepatic infarction is a very uncommon condition because the liver receives blood from 2 sources: the hepatic artery and the portal vein. This type of infarction typically happens only when blood flow is blocked in both the hepatic artery and the portal vein, although in most cases it results from a sudden blockage in the portal vein. In our case, portal vein circulation was normal. Treatment for hepatic infarct focuses on addressing the underlying cause, managing symptoms, and preventing further complications. Our patient was managed with anticoagulation therapy and supportive symptomatic treatment, as provided in current clinical recommendations [10,12,15]. The patient’s clinical condition improved and her recovery was uneventful.
From a management perspective, this case illustrates the importance of individualized anticoagulation strategies and multidisciplinary collaboration, including internal medicine, vascular surgery, radiology, and hematology. The patient’s favorable outcome was achieved through coordinated care, appropriate imaging, timely diagnosis, and personalized therapeutic decisions.
Conclusions
This case highlights the rare occurrence of multiple visceral arterial thromboses in a previously healthy woman, likely precipitated by the synergistic prothrombotic effects of long-term combined oral contraceptive use and long-term smoking. Despite the absence of underlying thrombophilia or autoimmune disease, the patient experienced extensive arterial thrombotic events involving the hepatic, mesenteric, renal, and splenic arteries. Prompt diagnosis, discontinuation of estrogen-containing contraceptives, and individualized anticoagulation management – including early recognition and treatment of heparin-induced thrombocytopenia – were critical to the favorable outcome.
This case underscores the importance of considering arterial thrombosis in the differential diagnosis of acute abdominal pain, particularly in patients with modifiable risk factors. It highlights the need for vigilance when prescribing hormonal therapies in long-term smokers. Beyond its clinical relevance, this case report offers valuable educational insights into the diagnosis and management of complex thrombotic events, contributing to the fields of vascular medicine, pharmacology, and clinical practice.
References
1. Farmer RD, Lawrenson RA, Thompson CR, Population-based study of risk of venous thromboembolism associated with various oral contraceptives: Lancet, 1997; 349(9045); 83-88
2. Tanis BC, van den Bosch MA, Kemmeren JM, Oral contraceptives and the risk of myocardial infarction: N Engl J Med, 2001; 345(25); 1787-93
3. Lidegaard O, Smoking and use of oral contraceptives: Impact on thrombotic diseases: Am J Obstet Gynecol, 1999; 180(6 Pt 2); S357-63
4. Pomp ER, Rosendaal FR, Doggen CJ, Smoking increases the risk of venous thrombosis and acts synergistically with oral contraceptive use: Am J Hematol, 2008; 83(2); 97-102
5. Fruzzetti F, Ricci C, Fioretti P, Haemostasis profile in smoking and nonsmoking women taking low-dose oral contraceptives: Contraception, 1994; 49(6); 579-92
6. Carr BR, Ory H, Estrogen and progestin components of oral contraceptives: Relationship to vascular disease: Contraception, 1997; 55(5); 267-72
7. Lamy AL, Roy PH, Morissette JJ, Cantin R, Intimal hyperplasia and thrombosis of the visceral arteries in a young woman: Possible relation with oral contraceptives and smoking: Surgery, 1988; 103(6); 706-10
8. El-Reshaid K, Al-Bader S, Sallam H, Multiple visceral venous thromboses associated with oral contraceptive use: Saudi J Kidney Dis Transpl, 2016; 27(6); 1256-59
9. Meade TW, Risks and mechanisms of cardiovascular events in users of oral contraceptives: Am J Obstet Gynecol, 1988; 158(6 Pt 2); 1646-52
10. Takayama T, Miyata T, Shirakawa M, Nagawa H, Isolated spontaneous dissection of the splanchnic arteries: J Vasc Surg, 2008; 48(2); 329-33
11. Saad E, Awadelkarim A, Agab M, Babkir A, Extensive aortic thrombosis and renal infarction in association with an active flare-up of Crohn’s disease: Gastroenterology Res, 2022; 15(2); 100-5
12. Zeina AR, Nachtigal A, Mahamid A, Isolated spontaneous dissection of a visceral artery: A rare cause of epigastric pain: Emerg Radiol, 2015; 22(3); 215-20
13. Jiang H, Huang C, Shi Y, Effect of smoking on thrombotic antiphospholipid syndrome: A 10-year prospective cohort study: Rheumatology (Oxford), 2024; 63(7); 1917-22
14. Warkentin TE, Laboratory diagnosis of heparin-induced thrombocytopenia: Int J Lab Hematol, 2019; 41(1); 15-25
15. Brück S, Skrabal C, Liebold A, Intrahepatic hematoma and pulmonary embolism in a young woman with oral contraceptives complicated by type II heparin-induced thrombocytopenia requiring ECMO therapy: A case report: Anasthesiol Intensivmed Notfallmed Schmerzther, 2019; 54(4); 295-300
16. Warkentin TE, Sheppard JI, Smith JW, Combination of two complementary automated rapid assays for diagnosis of heparin-induced thrombocytopenia (HIT): J Thromb Haemost, 2020; 18(6); 1435-46
17. Kramer R, Oberg-Higgins P, Russo L, Braxton JH, Heparin-induced thrombocytopenia with thrombosis syndrome managed with plasmapheresis: Interact Cardiovasc Thorac Surg, 2009; 8(4); 439-41
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133