26 June 2025: Articles 
Esotropia Induced by Slipped Lateral Rectus Muscle After Orbital Fat Herniation Surgery: A Case Report
Unusual clinical course, Challenging differential diagnosis, Diagnostic / therapeutic accidents
Kie Iida ABCDEF 1,2, Toshiaki Goseki ADEG 3,4,5*, Toru Kawanobe B 4, Shinya TakahashiDOI: 10.12659/AJCR.948643
Am J Case Rep 2025; 26:e948643






Abstract
BACKGROUND: Strabismus and diplopia are well-documented complications following various ophthalmic surgeries; however, no prior reports have linked these complications to orbital fat herniation surgery. Here, we report a case of secondary esotropia resulting from lateral rectus muscle injury following orbital fat herniation surgery.
CASE REPORT: A man in his 60s presented to our hospital with diplopia during distance fixation, which he noticed a few days after undergoing orbital fat herniation surgery on his right eye. His visual acuity was 24/20 in both eyes. Alternate prism cover testing revealed esotropia of 30 prism diopters for both distance- and near-vision. Mild limitation of abduction in the right eye and conjunctival scarring near the lateral rectus muscle were noted. Injury to the lateral rectus muscle during the previous surgery was suspected. However, due to the mild degree of abduction limitation, transient diplopia was also considered, and the patient was initially observed. However, no improvement in abduction limitation or esotropia was noted over the following months. Consequently, strabismus surgery was performed 8 months after the initial procedure. Intraoperatively, a slipped lateral rectus muscle was identified, and the muscle was advanced to a position 7 mm posterior to the limbus on the sclera. The patient’s abduction improved, and satisfactory ocular alignment was achieved postoperatively.
CONCLUSIONS: When strabismus with ocular motility limitation is observed after orbital fat herniation surgery, the possibility of lateral rectus muscle injury should be considered. If observation does not show improvement, strabismus surgery may be necessary.
Keywords: Diplopia, Strabismus, Humans, Male, Oculomotor Muscles, Esotropia, Adipose Tissue, Ophthalmologic Surgical Procedures, Postoperative Complications, Middle Aged, herniorrhaphy, Orbital Diseases
Introduction
Orbital fat herniation typically presents as a subconjunctival yellowish mass located on the temporal side of the eye and is commonly observed in middle-aged or older individuals. This condition is typically associated with localized weakening or thinning of Tenon’s capsule, resulting from aging or surgical trauma, and tends to occur more often in men and individuals with obesity [1–4]. Various surgical management procedures are used [5], including transconjunctival excision of orbital fat prolapse [3,4,6] and conjunctival fixation to the sclera without excising the herniated fat [7,8]. Potential postoperative complications include infection, retrobulbar hemorrhage, hypolacrimation due to excessive manipulation or inadvertent excision of lacrimal gland ductules, and diplopia resulting from extraocular muscle involvement; however, these complications are exceedingly rare [5].
Postoperative diplopia and strabismus have been reported following various ocular surgeries, including those involving the eyelid, conjunctiva, cataracts, glaucoma, retina, and orbit [9–18]. Causes include sensory disturbance due to binocular dysfunction, adherence from scarring, direct extraocular muscle and orbital pulley injury, myotoxicity from local anesthetics, and malpositioning of the extraocular muscles and orbital pulleys due to implant materials [10,11,14,15,17,19]. The reported incidence of postoperative diplopia varies widely: 0.1–1.4% after cataract surgery, 3–9% after glaucoma drainage device implantation, and 3–23% after scleral buckling surgery [14,16,17,20–25]. Notably, 23.2% of surgeons reported observing diplopia in patients following lower blepharoplasty [11]. The frequency of diplopia and strabismus following extraocular surgery is higher than that following intraocular surgery due to the proximity of the operative site to the extraocular muscles.
Diplopia associated with blepharoplasty and pterygium surgery has been well documented [10–12,19,26–28]. Similarly, orbital fat herniation surgery, an extraocular surgery, carries a risk of extraocular movement disorders due to excessive resection of Tenon’s capsule or improper suturing of the conjunctiva to the sclera [8]. However, despite the associated risks of extraocular muscle damage from transconjunctival approaches, a PubMed search using the terms “orbital fat herniation,” “orbital fat prolapse,” “diplopia,” and “strabismus” revealed no previous reports of postoperative diplopia or strabismus. Here, we report a case of strabismus following orbital fat herniation surgery caused by extraocular muscle injury, which showed a favorable outcome after surgical intervention.
Case Report
The patient was a man in his 60s who had undergone right orbital fat herniation surgery. A few days after the surgery, he noticed diplopia while driving a car and was subsequently referred to our clinic on the eighth day after surgery with diplopia as his chief concern. He did not report having near-vision diplopia in daily life, likely due to compensation with an adaptive head posture. His BMI was 27.5 and he had no previous medical history, including a history of orbital trauma. At the initial visit, his best-corrected visual acuity was 24/20 and intraocular pressure was 14 mmHg in both eyes. Alternate prism cover testing (APCT) revealed a 30-prism diopter (Δ) esotropia for both distance and near fixation, along with limited abduction in the right eye on both version and duction (Figure 1A). The Hess chart demonstrated abduction restriction of the right eye and incomitant esotropia (Figure 1B). A slit-lamp examination revealed scarring on the conjunctiva near the right lateral rectus muscle insertion, while the fundus examination was normal (Figure 2).
Although damage to the lateral rectus muscle due to orbital fat hernia surgery was suspected, the risk of it becoming a ‘lost muscle’ was considered low due to the preserved function of the inferior oblique muscle, and the restriction of extraocular movement was mild. Therefore, observation was chosen initially, as temporary extraocular muscle dysfunction due to inflammation was a possibility. However, as no improvement was seen in the restricted abduction or esotropia during follow-up conducted every few months until 5 months postoperatively, strabismus surgery was performed under general anesthesia 8 months postoperatively.
Figure 3 shows the strabismus surgery. During the procedure, a conjunctival incision was made at the fornix base on the temporal side of the right eye. Adhesions around the insertion of the lateral rectus muscle were carefully dissected. Upon exposing the muscle, it was found to be connected to the sclera by thin, translucent membranous tissue, and the muscle retracted posteriorly. After passing a single-armed 6-0 absorbable polyglycolic acid suture (Vsorb, Crownjun, Tokyo, Japan) through the superior and inferior ends of the lateral rectus muscle belly, the membranous tissue between the muscle and scleral attachment was excised. The lateral rectus muscle was then advanced anteriorly, and each end was securely sutured to the sclera 7 mm posterior to the corneal limbus using the same suture. The excised tissue measured approximately 7 mm in length. The defect in Tenon’s capsule, identified as the hernia orifice that had not been repaired in the previous surgery, was closed with 6-0 Vsorb sutures, and the conjunctiva was closed with 9-0 non-absorbable silk sutures to complete the surgery. Histopathological analysis of the excised tissue revealed that it consisted of collagen fibers and adipose tissue without muscle fibers (Figure 4). One month postoperatively, APCT showed 25 Δ exotropia and 10 Δ right hypertropia at distance, as well as 25 Δ intermittent exotropia and 3 Δ right intermittent near-vision hypertropia. A-2 limitation in right adduction was observed. By the fourth postoperative month, the limitation in right adduction had improved, and ocular alignment had improved to 6 Δ exophoria and 4 Δ right hyperphoria at distance, 8 Δ exophoria for near vision, with no diplopia, indicating a favorable outcome. At the final follow-up 1 year postoperatively, ocular alignment was 2 Δ exophoria and 1 Δ right hyperphoria at distance, and 8 Δ exophoria for near vision (Figure 5).
Discussion
This case is the first reported instance of esotropia resulting from a lateral rectus muscle injury following orbital fat herniation surgery. The patient’s ocular alignment and motility improved postoperatively, with a favorable outcome achieved through surgical intervention.
Abnormal extraocular muscle insertions in secondary strabismus can be categorized morphologically into 3 types: lost muscle (complete absence of muscle attachment to the sclera), slipped muscle (where a thin, translucent membrane attaches to the sclera while the muscle itself is displaced posteriorly), and stretched scar (where the rectus muscle is attached to the sclera by a segment of amorphous scar tissue, known as a pseudo-tendon) [29–31]. In all these conditions, the force generated by muscle contraction does not transmit effectively to the globe, resulting in limited eye movement in the direction of the affected muscle. The onset of lost or slipped muscles typically occurs immediately postoperatively, accompanied by significant movement restrictions, whereas stretched scar formations often present months later or more with milder restrictions [31]. Direct surgical exploration is often necessary for a definitive diagnosis because differentiating these conditions through clinical observation alone is challenging, and MRI may not reliably differentiate between slipped muscles and stretched scars [29,32]. In this case, which involved early-onset diplopia following orbital fat herniation surgery, intraoperative findings revealed that the lateral rectus muscle was connected to the sclera by thin, translucent membranous tissue, with the muscle itself retracted posteriorly, confirming the diagnosis of a slipped muscle. The excised membranous tissue measured approximately 7 mm in length, and the absence of muscle fibers within it further supported this diagnosis [31,33,34]. The relatively mild limitation in abduction likely resulted from the lateral rectus muscle’s retraction halting near the inferior oblique muscle.
Transient extraocular muscle dysfunction due to postoperative inflammation or edema should be considered as a differential diagnosis. Diplopia following surgery can result from temporary muscle paralysis caused by intramuscular hemorrhage or inflammation, or from permanent damage due to direct muscle injury [35,36]. A study on diplopia after lower blepharoplasty reported that diplopia resolved within 1 month in 24% of cases, within 1–3 months in 33%, and after more than 3 months in 37% [11]. In cases of diplopia following transconjunctival blepharoplasty, some patients required over 8 months for resolution [28]. Since transient extraocular muscle dysfunction can also take time to recover, distinguishing it from permanent diplopia caused by extraocular muscle injury is challenging. Early reoperation is recommended for slipped muscle cases, as delayed surgery lowers the success rate due to muscle contracture and tightening of both the affected muscle and its antagonist [29,37]. Early intervention is particularly crucial for the medial rectus muscle, which lacks support from surrounding oblique muscles, making recovery more challenging. However, other rectus muscles may be retrievable, justifying an initial observation period to determine if the dysfunction is temporary. Given that over 50% of transient diplopia cases resolve within 3 months, surgical intervention is advisable if no improvement is observed after this period. Although surgery in this case was performed 8 months postoperatively, successful recovery of the lateral rectus muscle and improved ocular motility were achieved.
Additionally, from a clinical perspective, this case underscores the importance of careful intraoperative handling of the conjunctiva and Tenon’s capsule during orbital fat herniation surgery to prevent extraocular muscle injuries. In this patient, the conjunctival scar was located near the lateral rectus muscle insertion. Surgeons should be aware of the risk of extraocular muscle injury during orbital fat herniation surgery, and approaching from the superior-temporal conjunctiva in the fornix region may help minimize this risk.
Conclusions
This report highlights a case involving esotropia caused by a slipped lateral rectus muscle following orbital fat herniation surgery. When strabismus with restricted extraocular movement is observed after orbital fat herniation surgery, the possibility of lateral rectus muscle injury should be considered. If the affected muscle is the lateral rectus and no improvement occurs after 3 months of observation, surgery may be warranted to address the muscle injury.
Figures
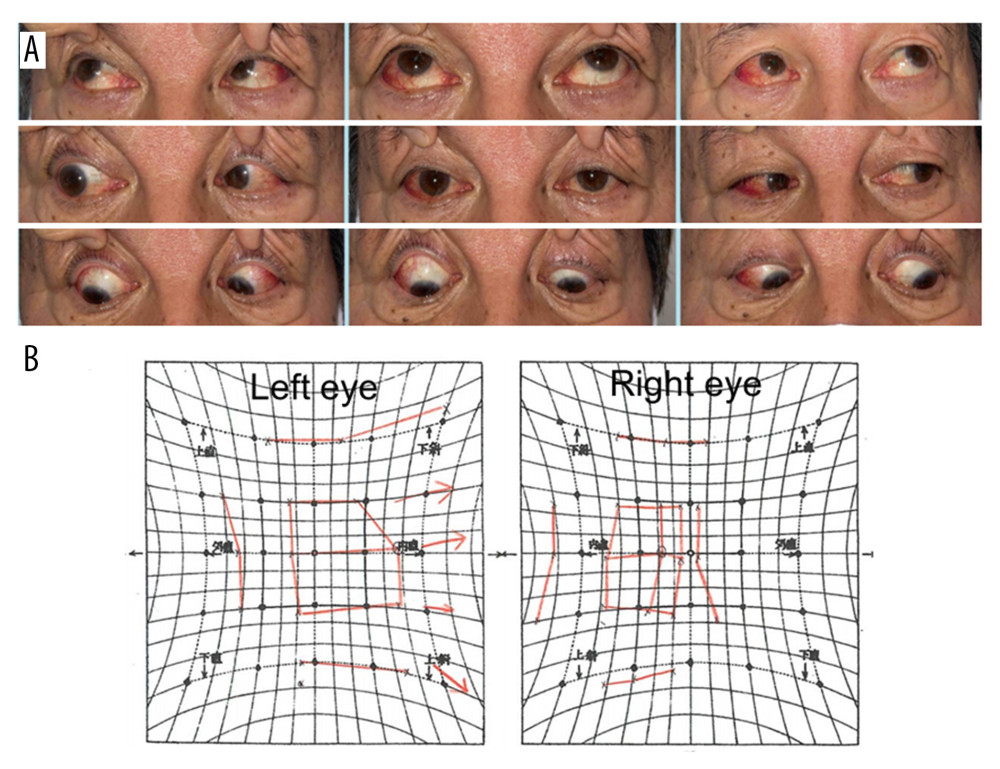 Figure 1. Preoperative extraocular movement test. (A) At the initial medical examination, mild limitation of the right eye’s abduction can be observed.(B) Hess chart at 1 month after the initial medical examination, showing persistent limitation of right eye’s abduction.
Figure 1. Preoperative extraocular movement test. (A) At the initial medical examination, mild limitation of the right eye’s abduction can be observed.(B) Hess chart at 1 month after the initial medical examination, showing persistent limitation of right eye’s abduction. 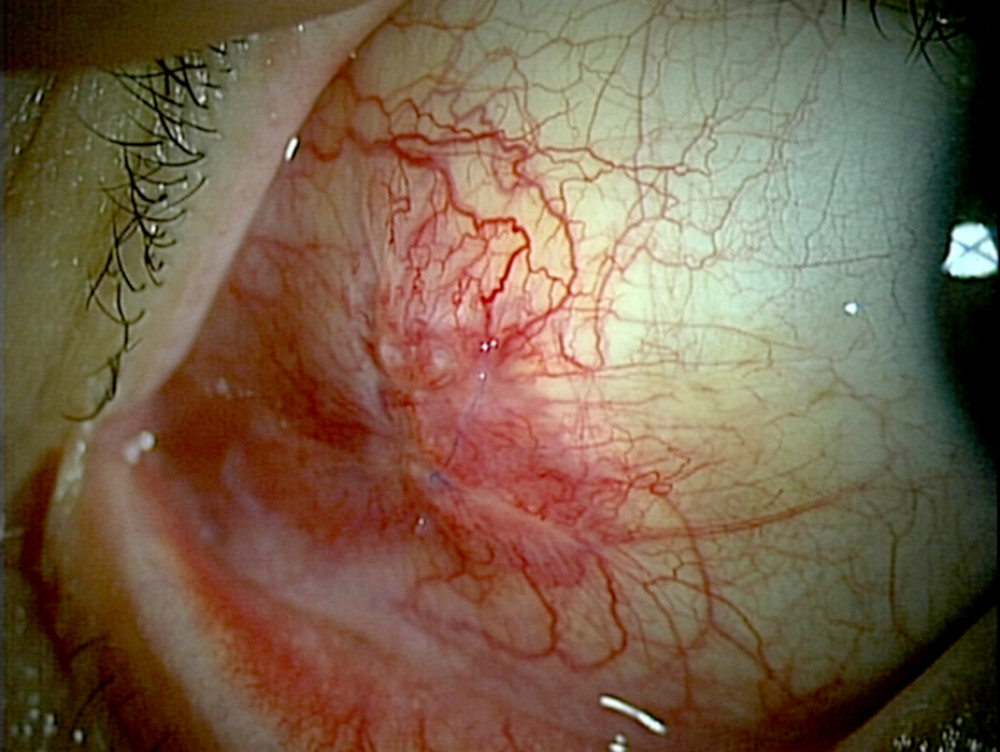 Figure 2. External eye photograph at initial medical examination. A scar can be observed near the insertion of the lateral rectus muscle of the right eye.
Figure 2. External eye photograph at initial medical examination. A scar can be observed near the insertion of the lateral rectus muscle of the right eye. 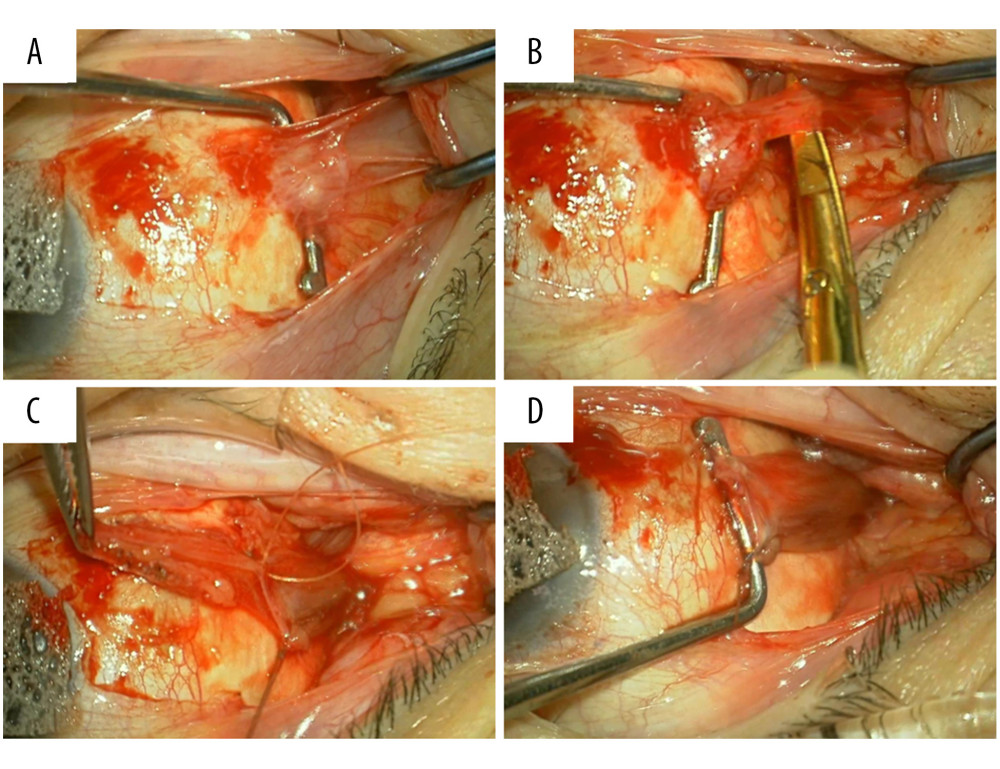 Figure 3. Right lateral rectus muscle advancement. (A) Fat adhesion and scar formation observed in the lateral rectus muscle insertion area. (B) A translucent membrane tissue extends posteriorly from the muscle insertion. (C) The lateral rectus muscle belly posterior to the membrane tissue has been sutured, and the membrane tissue has been detached. The excised membrane tissue is held in the forceps. The muscle belly is posterior to the suture. (D) The muscle belly has been sutured to the sclera 7 mm from the corneal limbus.
Figure 3. Right lateral rectus muscle advancement. (A) Fat adhesion and scar formation observed in the lateral rectus muscle insertion area. (B) A translucent membrane tissue extends posteriorly from the muscle insertion. (C) The lateral rectus muscle belly posterior to the membrane tissue has been sutured, and the membrane tissue has been detached. The excised membrane tissue is held in the forceps. The muscle belly is posterior to the suture. (D) The muscle belly has been sutured to the sclera 7 mm from the corneal limbus. 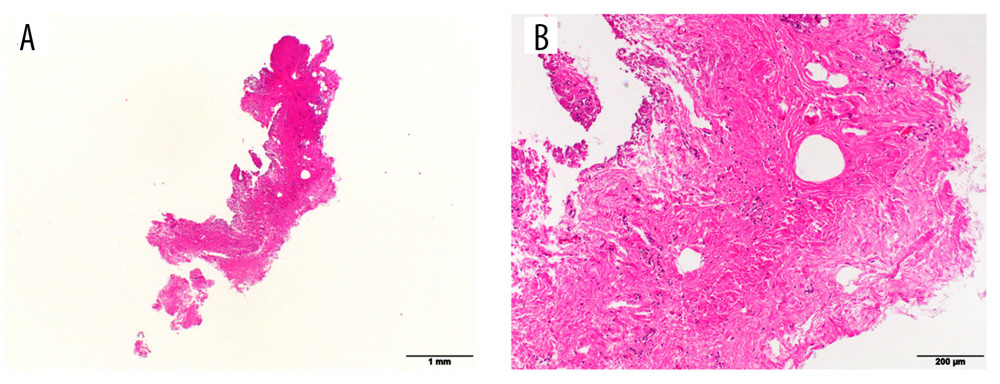 Figure 4. Hematoxylin and eosin staining image of excised tissue. (A) Low-power view of the excised tissue. (B) High-power view of the same tissue. The tissue consists of collagen fibers and adipose tissue, with poor vascularity and no muscle fibers.
Figure 4. Hematoxylin and eosin staining image of excised tissue. (A) Low-power view of the excised tissue. (B) High-power view of the same tissue. The tissue consists of collagen fibers and adipose tissue, with poor vascularity and no muscle fibers. 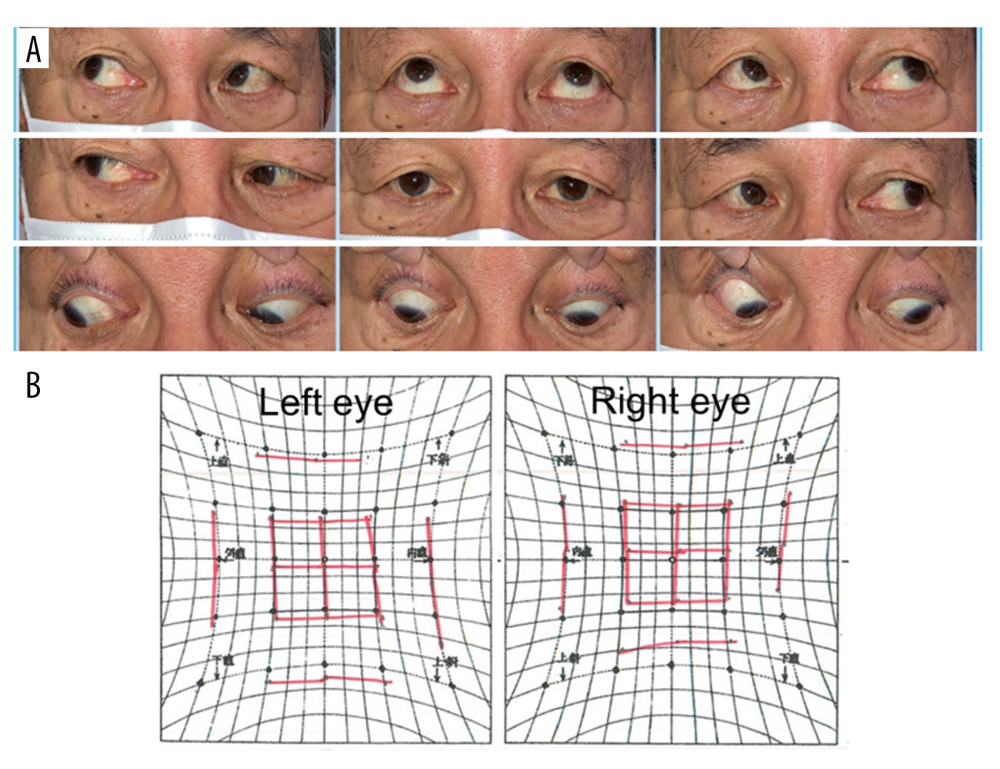 Figure 5. Extraocular movements 1 year after surgery. (A) Extraocular movement photograph. (B) Hess chart showing the improvement in the limitation of the right eye’s abduction and the adduction after surgery.
Figure 5. Extraocular movements 1 year after surgery. (A) Extraocular movement photograph. (B) Hess chart showing the improvement in the limitation of the right eye’s abduction and the adduction after surgery. References
1. Glover AT, Grove AS, Subconjunctival orbital fat prolapse: Ophthalmic Plast Reconstr Surg, 1987; 3(2); 83-86
2. Jordan DR, Tse DT, Herniated orbital fat: Can J Ophthalmol, 1987; 22(3); 173-77
3. McNab AA, Subconjunctival fat prolapse: Aust N Z J Ophthalmol, 1999; 27(1); 33-36
4. Siban M, Weijtens O, van den Bosch W, Paridaens D, Efficacy of transconjunctival excision of orbital fat prolapse: A long-term follow-up study: Acta Ophthalmol, 2014; 92(3); 291-93
5. Secondi R, Sánchez España JC, Castellar Cerpa J, Ibáñez Flores N, Subconjunctival orbital fat prolapse: An update on diagnosis and management: Semin Ophthalmol, 2019; 34(2); 69-73
6. Wang X, Yan J, Subconjunctival orbital fat prolapse: An unsuspecting rare lesion: J Craniofac Surg, 2015; 26(2); e92-94
7. Nakamura N, Akiyama K, Shigeyasu C, Yamada M, Surgical repair of orbital fat prolapse by conjunctival fixation to the sclera: Clin Ophthalmol, 2015; 9; 1741-44
8. Otaka I, Kyu N, A new surgical technique for the management of orbital fat prolapse: Am J Ophthalmol, 2001; 131(2); 267-69
9. Hamed LM, Strabismus presenting after cataract surgery: Ophthalmology, 1991; 98(2); 247-52
10. Baxter SL, Nguyen BJ, Kinori M, Identification and correction of restrictive strabismus after pterygium excision surgery: Am J Ophthalmol, 2019; 202; 6-14
11. Becker BB, Diplopia following lower blepharoplasty: J AAPOS, 2020; 24(6); 363e1-e4
12. Jenkins PF, Stavis MI, Jenkins DE, Esotropia following pterygium surgery: Binocul Vis Strabismus Q, 2002; 17(3); 227-28
13. Rossel-Zemkouo MJ, Bergholz R, Salchow DJ, Strabismus patterns after cataract surgery in adults: Strabismus, 2021; 29(1); 19-25
14. Sobol EK, Rosenberg JB, Strabismus after ocular surgery: J Pediatr Ophthalmol Strabismus, 2017; 54(5); 272-81
15. Guo S, Wagner R, Gewirtz M, Diplopia and strabismus following ocular surgeries: Surv Ophthalmol, 2010; 55(4); 335-58
16. Costa PG, Debert I, Passos LB, Polati M, Persistent diplopia and strabismus after cataract surgery under local anesthesia: Binocul Vis Strabismus Q, 2006; 21(3); 155-58
17. MacDonald IM, Reed GF, Wakeman BJ, Strabismus after regional anesthesia for cataract surgery: Can J Ophthalmol, 2004; 39(3); 267-71
18. Robbins L, Goseki T, Law SK, Strabismus after Ahmed Glaucoma valve implantation: Am J Ophthalmol, 2021; 222; 1-5
19. Sen P, Kumar A, Jain E, Mohan A, Slipped medial rectus muscle with stretched scar after pterygium surgery: J Pediatr Ophthalmol Strabismus, 2019; 56; e34-e37
20. Corboy JM, Jiang X, Postanesthetic hypotropia: A unique syndrome in left eyes: J Cataract Refract Surg, 1997; 23(9); 1394-98
21. Hong CH, Arosemena A, Zurakowski D, Ayyala RS, Glaucoma drainage devices: A systematic literature review and current controversies: Surv Ophthalmol, 2005; 50(1); 48-60
22. Goezinne F, Berendschot TT, van Daal EW, Diplopia was not predictable and not associated with buckle position after scleral buckling surgery for retinal detachment: Retina, 2012; 32(8); 1514-24
23. Fison PN, Chignell AH, Diplopia after retinal detachment surgery: Br J Ophthalmol, 1987; 71(7); 521-25
24. Akbari MR, Mirmohammadsadeghi A, Makateb A, Ocular movement disorders following scleral buckling surgery: A case series study: J Curr Ophthalmol, 2019; 31(2); 195-200
25. Smiddy WE, Loupe D, Michels RG, Extraocular muscle imbalance after scleral buckling surgery: Ophthalmology, 1989; 96(10); 1485-89 discussion 1489–90
26. Syniuta LA, Goldberg RA, Thacker NM, Rosenbaum AL, Acquired strabismus following cosmetic blepharoplasty: Plast Reconstr Surg, 2003; 111(6); 2053-59
27. Ugrin MC, Molinari A, Disinsertion of the medial rectus following pterygium surgery: Signs and management: Strabismus, 1999; 7(3); 147-52
28. Ghabrial R, Lisman RD, Kane MA, Diplopia following transconjunctival blepharoplasty: Plast Reconstr Surg, 1998; 102(4); 1219-25
29. Plager DA, Parks MM, Recognition and repair of the “lost” rectus muscle. A report of 25 cases: Ophthalmology, 1990; 97(1); 131-36 discussion 136–37
30. Parks MM, Bloom JN, The “slipped” muscle: Ophthalmology, 1979; 86(8); 1389-96
31. Ludwig IH, Chow AY, Scar remodeling after strabismus surgery: J AAPOS, 2000; 4(6); 326-33
32. Negishi T, Hikoya A, Isoda H, Magnetic resonance imaging of the medial rectus muscle of patients with consecutive exotropia after medial rectus muscle recession: Ophthalmology, 2010; 117(10); 1876-82
33. Al-Haddad C, Abdul Fattah M, Slipped extraocular muscles: Characteristics and surgical outcomes: Can J Ophthalmol, 2017; 52(1); 42-47
34. Plager DA, Parks MM, Recognition and repair of the slipped rectus muscle: J Pediatr Ophthalmol Strabismus, 1988; 25(6); 270-74
35. Hayworth RS, Lisman RD, Muchnick RS, Smith B, Diplopia following blepharoplasty: Ann Ophthalmol, 1984; 16(5); 448-51
36. Rees TD, Wood-Smith D: Cosmetic facial surgery, 1973; 52, Philadelphia, W B Saunders
37. Lenart TD, Lambert SR, Slipped and lost extraocular muscles: Ophthalmol Clin North Am, 2001; 14(3); 433-42
Figures
Figure 1. Preoperative extraocular movement test. (A) At the initial medical examination, mild limitation of the right eye’s abduction can be observed.(B) Hess chart at 1 month after the initial medical examination, showing persistent limitation of right eye’s abduction.Figure 2. External eye photograph at initial medical examination. A scar can be observed near the insertion of the lateral rectus muscle of the right eye.Figure 3. Right lateral rectus muscle advancement. (A) Fat adhesion and scar formation observed in the lateral rectus muscle insertion area. (B) A translucent membrane tissue extends posteriorly from the muscle insertion. (C) The lateral rectus muscle belly posterior to the membrane tissue has been sutured, and the membrane tissue has been detached. The excised membrane tissue is held in the forceps. The muscle belly is posterior to the suture. (D) The muscle belly has been sutured to the sclera 7 mm from the corneal limbus.Figure 4. Hematoxylin and eosin staining image of excised tissue. (A) Low-power view of the excised tissue. (B) High-power view of the same tissue. The tissue consists of collagen fibers and adipose tissue, with poor vascularity and no muscle fibers.Figure 5. Extraocular movements 1 year after surgery. (A) Extraocular movement photograph. (B) Hess chart showing the improvement in the limitation of the right eye’s abduction and the adduction after surgery. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133