03 July 2025: Articles 
Adult Presentation of Anorectal Malformation: A 19-Year-Old Woman with a Delayed Diagnosis of Recto-Vestibular Fistula
Congenital defects / diseases
Brian Osiemo BichangaDOI: 10.12659/AJCR.948656
Am J Case Rep 2025; 26:e948656






Abstract
BACKGROUND: In developing countries, the diagnosis of anorectal malformations (ARM) is often made late, with patients presenting in their teenage years or beyond. This has been attributed to several factors, including ignorance, poverty, and weak social support systems. We report a rare case of adult ARM and the problems encountered in her surgical management.
CASE REPORT: A 19-year-old woman presented with symptoms of chronic constipation. During further clinical evaluation, she was diagnosed with ARM with a recto-vestibular fistula. Her preoperative work-up to rule out other associated anomalies included an ECHO, KUB ultrasound, and pelvic MRI. She underwent a 3-stage repair, with the initial stage being a diverting colostomy and then definitive surgery after 6 months. We closed her stoma 3 months after the definitive surgery. In the immediate postoperative period, she developed wound dehiscence that was managed conservatively. Later, she had incontinence of stool and flatus. With the support of a multidisciplinary team, she was placed on a bowel management program and guided through pelvic floor exercises. About 5 weeks later, she was discharged home to continue follow-up at the surgical outpatient clinic.
CONCLUSIONS: The case report offers lessons to surgeons on the management of ARM with delayed presentation. It describes intraoperative challenges, potential postoperative complications, and possible solutions while highlighting follow-up difficulties in low- and middle-income countries (LMICs) due to inadequate social support. We also stress the need to improve healthcare systems to facilitate early ARM diagnosis.
Keywords: Anorectal malformations, delayed diagnosis, Rectal Fistula, Case Reports, Humans, Female, young adult, Rectovaginal Fistula, Colostomy, Constipation
Introduction
Anorectal malformations (ARM) are a spectrum of congenital anomalies that affect both males and females, involving the distal anus and rectum as well as the urinary and genital tracts. ARM occurs in about 1/5000 live births and is more common in females [1,2]. In males, internal connections to the lower urinary tract, like the urethra or bladder, are often seen with complex anorectal malformations [3]. In females, the vestibular fistula is the most prevalent form of ARM. Adult presentation is rare since most of these cases are generally diagnosed and corrected at birth [4]. Delays in diagnosing ARM until the teenage years or later are common in developing countries, often due to a combination of factors, including insufficient awareness, incorrect diagnoses, illiteracy, poverty, and lack of social support.
Late diagnosis of ARM may be associated with persistent constipation and can also lead to social and psychological difficulties due to problems with defecation control and sexual functioning. As a result, individuals may experience social isolation, potentially leading to depression and a decline in self-esteem. Female patients may also encounter difficulties and adverse outcomes throughout pregnancy and the delivery process [5].
The transition from pediatric to adult care poses unique challenges for patients with undiagnosed or untreated congenital anomalies such ARM. This delay often results in a lack of coordinated care, as these patients fall outside the typical pediatric surgical pathway and may not seek medical attention until symptoms become more pronounced [4]. Moreover, adult healthcare providers may have limited exposure to congenital anorectal anomalies, leading to further delays in appropriate referral and management. This case underscores the need for heightened clinical awareness and multidisciplinary collaboration to bridge the gap in care and ensure timely diagnosis and intervention for ARM patients who present beyond childhood.
Case Report
We report the case of a 19-year-old woman who was reviewed at Kenyatta National Hospital (KNH), which is the largest referral hospital in Nairobi, as a referral from a county-level hospital. She had initially presented at the referring facility during infancy on one of her routine vaccination visits, where according to her mother she was noted to have an absent anal opening with stool passing through an opening in the vestibule. After the review, she was directed to seek definitive care at KNH, but this was not followed through, with the mother citing financial and later social reasons.
At presentation, she appeared to be well-nourished, with evident secondary female characteristics, weighing 60 kg. The presenting concerns were chronic constipation associated with soiling, which she had been managing with intermittent use of stool softeners.
She was a reserved and introverted young woman residing with her parents, hesitant about using public toilet facilities and, when possible, opting to use the toilet at home. Following her recent admission to a boarding secondary school with more communal areas, including washrooms, she made the decision to seek medical care.
Physical examination confirmed the absent anal opening and a recto-vestibular fistula, with hard stools on digital rectal examination. Her blood work was normal. An echocardiography and kidneys, ureter, and bladder (KUB) ultrasound were part of the preoperative assessment and yielded normal results.
A staged surgical repair was scheduled, starting with examination under anaesthesia (EUA), whose findings confirmed the recto-vestibular fistula (Figure 1). The urethral opening was normal, and a vaginal examination found a uterine prolapse, with the cervix visualized in the lower part of the vagina (Figure 2). This incidental finding was attributed to chronic constipation, which is a known risk factor for prolapse of pelvic organs [6].
A divided sigmoid colostomy was fashioned, and the patient allowed to return home on day 5 after surgery. Prior to discharge, she was referred to a social worker and they had regular contact to ensure the patient attended her clinic follow-up visits.
As part of preoperative planning for the definitive surgery, a pelvic MRI was done, which detailed the anatomy and ruled out associated anomalies in the spinal and lumbo-sacral regions (Figure 3). An anorectoplasty through a posterior sagittal approach was scheduled 6 months after the first surgery.
Patient positioning was a key challenge in our case, as the prone jack-knife position is the standard for PSARP. A few adjustments were made, including placing the patient in a prone position and suspending the legs in lithotomy stirrups, with padding at pressure points for protection (Figure 4). An electro-stimulator was then used for anal mapping of the sphincter muscle complex. The surgery, conducted while standing at the foot of the bed, took approximately 6 hours to complete. Challenges during the surgery included the difficult mobilization of the rectum due to the extensive dissection, accompanied by increased bleeding that required the team to wear eye protection. The uterus, previously prolapsed, was manually repositioned and remained in place for the duration of the surgery. It had no impact on the complexity of the surgery.
The fistula was first circumferentially mobilized (Figure 5), and the rectum was then meticulously separated from the vagina, creating a neoanus calibrated at 20 mm Hegar (Figure 6). The surgery was completed with no intraoperative adverse events. A rectal pack left in-situ was removed after 24 hours. The patient was treated postoperatively with intravenous antibiotics for 7 days. With the presence of a diverting colostomy, feeding was initiated as soon as she had fully recovered from the effects of anaesthesia. Pain control posed a significant postoperative challenge, requiring the use of opioids for 1 week. As a result, the initiation of sitz baths, usually begun within 72 hours, was delayed. Given the size of the neoanus, it was decided to forgo postoperative dilatation, which is typically started on postoperative day 14.
Ten days after the surgery, she was scheduled for an EUA to address concerns regarding wound dehiscence. The EUA findings included a dehiscence at the 6 o’clock position about 4 cm inferior to the neoanus, which was healing well by secondary intention, with evidence of granulation tissue. No intervention was provided.
After a follow-up at the surgical clinic, where wound healing and general well-being was assessed, a stoma reversal was done 3 months after the PSARP. Postoperatively, the patient was incontinent for both feces and flatus for about 5 weeks. During this time, her case was managed by a multidisciplinary team that included nutritionists, counsellors, and a social worker. Interventions to resolve this problem included a bowel management program and pelvic floor exercises. She was discharged home on the stool softeners after 5 weeks, and advised to continue to perform pelvic floor exercises. During the short-term follow-up period of 4 months, she has stayed continent and has recently transitioned from daily to occasional stool softener use.
Discussion
ARMs in developing countries may not be detected at birth, and their initial presentation can occur during infancy or later in childhood, especially if there is no acute intestinal obstruction or related congenital malformations. Iram et al reported a case in India of a 23-year-old woman diagnosed with a recto-vestibular fistula. For years, she had lived with her condition, and only sought medical assistance when she decided to get married [7]. Oyania et al, from Uganda, documented a case of a 15-year-old girl with a recto-vestibular fistula who was lost to follow-up after a diversion colostomy was fashioned when she was 2 months old. Rejected by her community and thought to be cursed, she finally sought assistance when a well-wisher learned of her plight [8].
This delayed presentation may be attributed to factors such as late diagnosis, poverty, insufficient social support, inadequate medical facilities, low literacy, and lack of neonatal care [7]. There also remains a significant gap between the management protocols followed in high-middle-income countries and the practical limitations in low-middle-income countries, where surgeons work with fewer specialists, nurses, and technological resources [9].
Researchers have a varied definition of delayed presentation, although a diagnosis made after 24 hours of life is generally seen as late [10]. Some studies classify delayed presentation as situations where newborns with ARM are sent home from the hospital without a diagnosis [11].
The literature proposes a variety of diagnostic tests in the evaluation of patients with ARM, such as radiographic imaging of the sacrum and spine, voiding cystourethrogram (VCUG), magnetic resonance imaging (MRI), contrast enema, and colonoscopy. These examinations are essential for detecting other potential associated anomalies [2].
There are various options for surgical management of late-presenting ARM with perineal and vestibular fistulae, classified as either a primary repair or a staged repair, which typically consists of separate surgeries. The main appeal of primary repair is its potential to eliminate the morbidity associated with stomas [12]. In cases involving megarectum, positioning the enlarged rectum within the sphincter complex during the pull-through procedure is challenging, making it a major obstacle for primary definitive surgery. Therefore, an initial decompressing colostomy is often required, with tapering proctoplasty of the dilated segment a possible alternative for the pull-through [13,14].
A colostomy during repair is an effective strategy for reducing perineal wound complications and ensuring proper function of the perineal and sphincter muscles afterward.
Gupta et al provided evidence supporting a staged repair approach when they compared the outcomes of 1-stage vs the traditional 3-stage surgeries on female patients with variable ages up to 14 years who presented with perineal and vestibular fistulae. They concluded that primary 1-stage definitive surgery was associated with significantly more complications [14]. Bokhari et al describe performing a primary repair on a 23-year old with a recto-vestibular fistula, noting several postoperative complications, including flatus and fecal incontinence after 4 weeks, and later anal stenosis, which had to be surgically corrected [7].
Compared to infants and children, surgery for adult patients with ARM presents greater technical challenges. Sham et al cite several factors contributing to this difficulty, such as the convex shape of the adolescent sacrum, the thick neurovascular bundle that must be divided to achieve sufficient rectal length, which can lead to potential damage to pelvic nerves and significant bleeding. Additionally, fitting the dilated rectum within the sphincter muscle complex can be challenging. The duration of the operation is also considerably longer, typically lasting 2–5 hours [15].
In our case, we opted for a 3-stage repair starting with a diverting sigmoid colostomy followed 6 months later by an anorectoplasty, then colostomy closure. The initial surgery provided decompression and relief of the obstructive symptoms that she presented with. The interval between the first and second surgery allowed for multidisciplinary consultation and patient counselling regarding the definitive surgery and its anticipated outcomes.
The psychological impact of a delayed diagnosis of anorectal malformation in adulthood is profound, particularly in terms of body image, self-esteem, and social functioning [16]. Our patient reported long-standing feelings of embarrassment, social isolation, and anxiety, particularly around intimate relationships and routine social activities. Following her diagnosis, she was referred to a clinical psychologist with experience in chronic illness and body-focused conditions. Cognitive behavioral therapy (CBT) sessions were initiated to address negative thought patterns and to develop healthier coping strategies. Additionally, psychological education was provided to help her better understand the condition and normalize her emotional responses. Feedback from the patient indicated that psychological support was instrumental in reducing anxiety, improving her confidence, and helping her engage more comfortably in social settings. This holistic, multidisciplinary approach was essential in her overall recovery and adjustment following surgical management.
The logistics of neo-anal dilatations to prevent strictures, particularly in adults, is more complicated than may be expected. While Sham et al describe a strict protocol that starts 10–14 days after surgery and continues for 6–12 weeks after colostomy closure, they do not provide details of how this was carried out and the general acceptance among their adolescent patients [15]. Lopez et al, in their case series of 8 women who presented with ARM, faced compliance issues with weekly to bi-weekly dilatations, although the impact on outcomes was not addressed [17].
The repair of ARMs is associated with a range of complications. Sinha et al reported that constipation, anal excoriation, and occasional soiling were prominent postoperative concerns [18]. With regards to long-term outcomes, despite late presentation, patients with vestibular fistula who undergo surgical treatment can still attain sexual activity and fertility. Patients with recto-perineal and recto-vestibular fistulas are expected to have normal fertility [19]. Adejuyigbe et al reported a case of a 15-year old who, after surgery, was able to conceive and carry the pregnancy to term [20]. Similarly, Iwai et al described the cases of 4 teenage patients who, after undergoing ARM repair, were able to conceive and deliver children through the normal vaginal route [4].
Studies report that up to 50–70% of females with corrected ARMs experience some degree of sexual dysfunction, including dyspareunia, reduced sexual satisfaction, or fear of intercourse, often due to altered perineal anatomy, scarring, or psychological factors such as embarrassment and poor body image [21,22]. In our case, although the patient had not yet attempted conception, she expressed concerns regarding her reproductive future and the potential impact of surgical correction on sexual function.
Conclusions
The report draws attention to the challenges of managing an ARM patient with a late diagnosis, with a special focus on the technical demands of surgery, complications, and postoperative care. The case also calls attention to the challenges faced in developing countries, particularly the lack of social support and its impact on follow-up care after treatment. It underscores the need to enhance basic healthcare and increase awareness of congenital anomalies among the public and medical professionals, which could improve early detection and help prevent similar cases in the future.
Figures
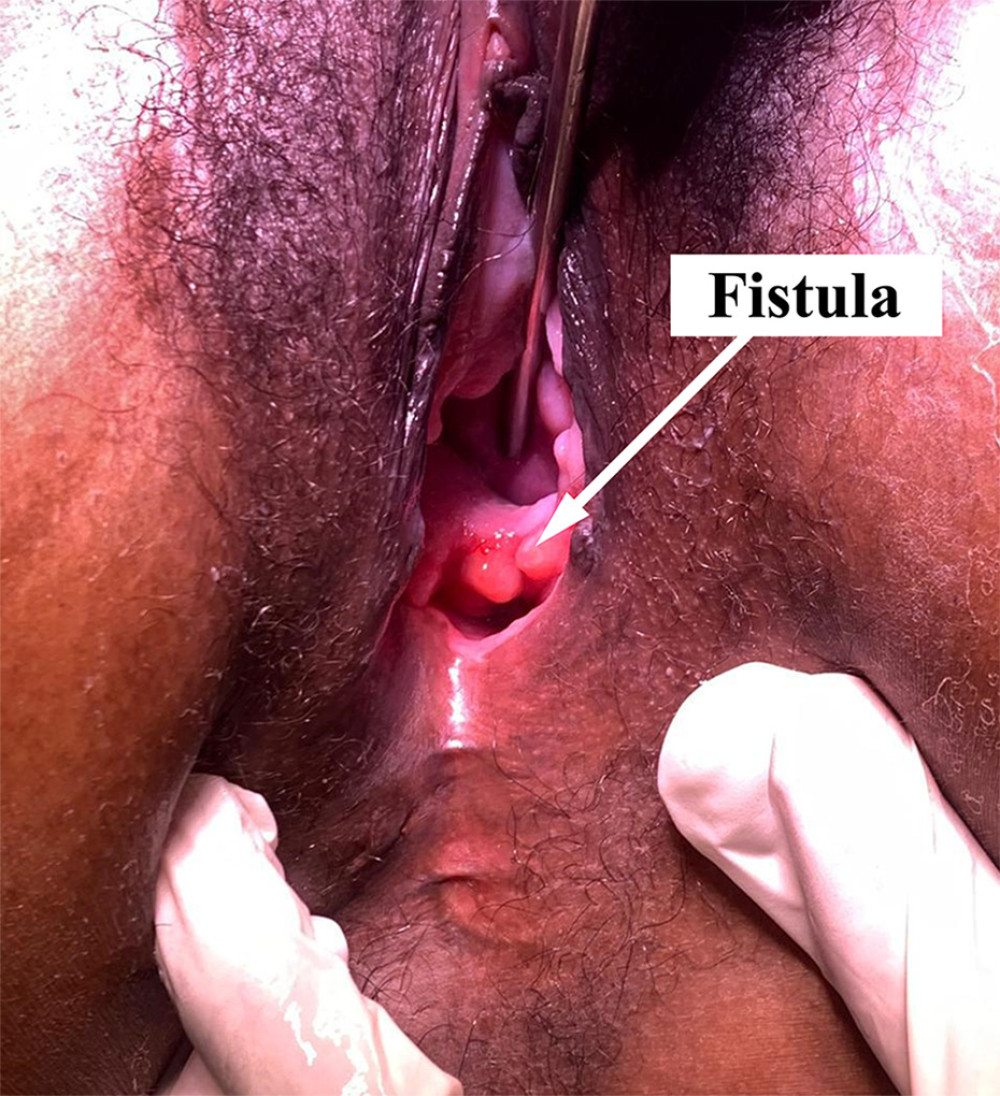 Figure 1. The image shows a recto-vestibular fistula (marked by an arrow). The anus is absent in the normal position. This photograph was taken during the preoperative examination.
Figure 1. The image shows a recto-vestibular fistula (marked by an arrow). The anus is absent in the normal position. This photograph was taken during the preoperative examination.  Figure 2. A photograph illustrating the prolapsed cervix (indicated by the arrow) and a clear view of the external genitalia.
Figure 2. A photograph illustrating the prolapsed cervix (indicated by the arrow) and a clear view of the external genitalia.  Figure 3. Pelvic magnetic resonance imaging shows a fistulous tract originating from the rectum extending anteriorly toward the vestibule. Surrounding pelvic structures are well visualized.
Figure 3. Pelvic magnetic resonance imaging shows a fistulous tract originating from the rectum extending anteriorly toward the vestibule. Surrounding pelvic structures are well visualized.  Figure 4. Patient positioned in a modified prone jack-knife position with both legs suspended.
Figure 4. Patient positioned in a modified prone jack-knife position with both legs suspended. 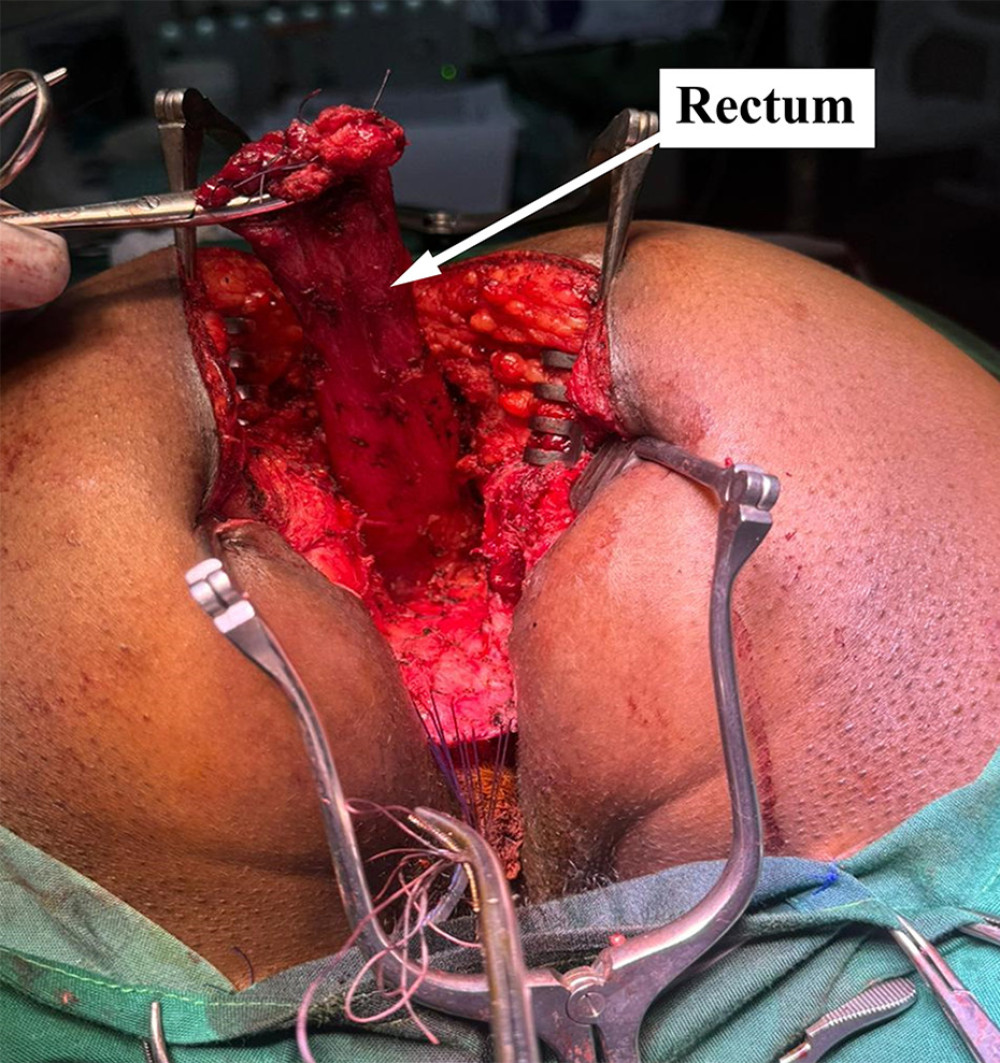 Figure 5. Intraoperative photograph showing the rectum (arrow) after complete circumferential dissection with adequate length achieved to allow tension-free anorectoplasty.
Figure 5. Intraoperative photograph showing the rectum (arrow) after complete circumferential dissection with adequate length achieved to allow tension-free anorectoplasty.  Figure 6. Image shows the neoanus (arrow) following definitive surgical repair. It is located centrally within the sphincter muscle complex.
Figure 6. Image shows the neoanus (arrow) following definitive surgical repair. It is located centrally within the sphincter muscle complex. References
1. Wu VK, Poenaru D, Poley MJ, Burden of surgical congenital anomalies in Kenya: A population-based study: J Trop Pediatr, 2013; 59(3); 195-202
2. Rintala RJ, Congenital anorectal malformations: Anything new?: Journal of Pediatric Gastroenterology and Nutrition, 2009; 48(S2); S79-82
3. Moore SW, Alexander A, Sidler D, The spectrum of anorectal malformations in Africa: Pediatr Surg Int, 2008; 24(6); 677-83
4. Iwai N, Deguchi E, Kimura O, Social quality of life for adult patients with anorectal malformations: J Pediatr Surg, 2007; 42(2); 313-17
5. Haider N, Fisher R, Mortality and morbidity associated with late diagnosis of anorectal malformations in children: Surgeon, 2007; 5(6); 327-30
6. Leung L, Riutta T, Kotecha J, Rosser W, Chronic constipation: An evidence-based review: J Am Board Fam Med, 2011; 24(4); 436-51
7. Bokhari I, Ali SU, Farooq AR, Khan A, Late presentation of a patient with an anorectal malformation (ARM): J Coll Physicians Surg Pak, 2010; 20(12); 825-27
8. Oyania F, Kotagal M, Situma M, 15-year-old with neglected recto-vestibular fistula in western Uganda: A case report: J Med Case Rep, 2021; 15(1); 96
9. Bokova E, Elhalaby I, Svetanoff WJ, Global strategies for postoperative care and bowel management in patients with anorectal malformations: Varied practices and barriers: J Pediatr Surg, 2024; 59(12); 161697
10. Divya G, Kundal VK, Debnath PR, Delayed presentation of anorectal malformations in a tertiary care hospital in India: Pediatr Surg Int, 2021; 37(4); 451-56
11. Kim HLN, Gow KW, Penner JG, Presentation of low anorectal malformations beyond the neonatal period: Pediatrics, 2000; 105(5); e68
12. Pena A, Migotto-Krieger M, Levitt MA, Colostomy in anorectal malformations: A procedure with serious but preventable complications: J Pediatr Surg, 2006; 41(4); 748-56 discussion 748–56
13. Negm M, Khedre M, Two-stage repair for delayed presentation of anorectal malformation with vestibular and perineal fistulae in females: Egypt J Surg, 2020; 39(2); 401
14. Gupta A, Agarwala S, Sreenivas V, Primary definitive procedure versus conventional three-staged procedure for the management of low-type anorectal malformation in females: A randomized controlled trial: J Indian Assoc Pediatr Surg, 2017; 22(2); 87
15. Sham M, Singh D, Phadke D, Anorectal malformations: Definitive management during and beyond adolescence: J Indian Assoc Pediatr Surg, 2012; 17(3); 120-23
16. Diseth TH, Emblem R, Long-term psychosocial consequences of surgical congenital malformations: Seminars in Pediatric Surgery, 2017; 26(5); 286-94
17. Lopez MPJ, Encila VI, Alamo SG, Anorectal malformations: Definitive surgery during adulthood: Tech Coloproctol, 2017; 21(2); 111-18
18. Sinha SK, Kanojia RP, Wakhlu A, Delayed presentation of anorectal malformations: J Indian Assoc Pediatr Surg, 2008; 13(2); 64-68
19. Huibregtse ECP, Draaisma JMTh, Hofmeester MJ, The influence of anorectal malformations on fertility: A systematic review: Pediatr Surg Int, 2014; 30(8); 773-81
20. Adejuyigbe O, Sowande OA, Olayinka OS, Fasubaa OB, Rectovestibular fistula with absent distal vagina in an adolescent Nigerian girl: J Pediatr Surg, 2002; 37(10); 1479-80
21. Rintala RJ, Pakarinen MP, Outcome of anorectal malformations and Hirschsprung’s disease beyond childhood: Semin Pediatr Surg, 2010; 19(2); 160-67
22. Levitt MA, Peña A, Anorectal malformations: Orphanet J Rare Dis, 2007; 2; 33
Figures
Figure 1. The image shows a recto-vestibular fistula (marked by an arrow). The anus is absent in the normal position. This photograph was taken during the preoperative examination.Figure 2. A photograph illustrating the prolapsed cervix (indicated by the arrow) and a clear view of the external genitalia.Figure 3. Pelvic magnetic resonance imaging shows a fistulous tract originating from the rectum extending anteriorly toward the vestibule. Surrounding pelvic structures are well visualized.Figure 4. Patient positioned in a modified prone jack-knife position with both legs suspended.Figure 5. Intraoperative photograph showing the rectum (arrow) after complete circumferential dissection with adequate length achieved to allow tension-free anorectoplasty.Figure 6. Image shows the neoanus (arrow) following definitive surgical repair. It is located centrally within the sphincter muscle complex. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,422
22,759,422
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  175,936
175,936
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,499
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,510
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133