24 June 2025: Articles 
Postoperative Dysphagia Management in Hemifacial Spasm: A Case Report of Combined Catheter Balloon and Neuromuscular Stimulation
Unusual setting of medical care, Patient complains / malpractice, Rare disease
Qian Zhang BCEF 1,2, Shuang Wu AD 1,2*, Yangmei Shi BC 1, Qian Chen CD 1, Jiajie Gao BC 1DOI: 10.12659/AJCR.948795
Am J Case Rep 2025; 26:e948795






Abstract
BACKGROUND: Hemifacial spasm is a frequently encountered cranial nerve disorder caused by vascular compression, and microvascular decompression is considered the criterion standard treatment, particularly for cases resistant to pharmacological or botulinum toxin therapy. Although microvascular decompression is generally safe, it carries the risk of cranial nerve complications. Glossopharyngeal and vagus nerve dysfunction can result in cricopharyngeal dysfunction, leading to significant postoperative dysphagia characterized by poor upper esophageal sphincter (UES) opening, aspiration, and pharyngeal residue. Early and effective rehabilitation is critical but rarely documented in such cases.
CASE REPORT: We present a case of a 58-year-old man who developed severe dysphagia following microvascular decompression for left-sided hemifacial spasm. Postoperative videofluoroscopic swallowing study (VFSS) confirmed cricopharyngeal dysfunction, showing delayed hyoid elevation and restricted UES opening. A comprehensive rehabilitation protocol was initiated, combining neuromuscular electrical stimulation (NMES) with balloon-guided volitional swallowing training (CBD). NMES targeted submental and laryngeal regions to facilitate muscle activation and enhance sensory feedback. CBD involved repeated, guided swallowing with balloon catheter assistance to promote UES opening. After 2 weeks of daily therapy, VFSS showed significant improvement in UES relaxation and pharyngeal clearance. The patient transitioned from nasogastric feeding to full oral intake, with a functional oral intake scale score of 6.
CONCLUSIONS: Cricopharyngeal dysfunction is a rare but disabling complication following microvascular decompression. This case demonstrates that early, combined rehabilitative approaches – especially integration of NMES and volitional CBD – can lead to meaningful recovery of swallowing function and better patient outcomes.
Keywords: Hemifacial Spasm, Rehabilitation, Treatment Outcome, Humans, Male, Deglutition Disorders, Middle Aged, Postoperative Complications, Electric Stimulation Therapy, Microvascular Decompression Surgery
Introduction
Hemifacial spasm (hemifacial spasm) is a prevalent primary cranial nerve disorder, with an incidence of approximately 11 per 100 000 individuals [1]. Microvascular decompression is currently acknowledged as the most efficacious treatment for the condition, particularly when pharmacological therapies and botulinum toxin injections prove ineffective [2]. According to the literature, the incidence of postoperative cranial nerve palsies ranges from 8% to 10% [3]. Among these, glossopharyngeal nerve dysfunction can lead to postoperative dysphagia, with a clinical incidence of approximately 0.2% [4]. This can result in cricopharyngeus muscle dysfunction, primarily presenting as dysphagia, aspiration, and choking [5], significantly impairing the patient’s quality of daily life.
Several comprehensive rehabilitation therapies for treating cricopharyngeal dysfunction exist, including swallowing training, neuromuscular electrical stimulation (NMES), cricopharyngeal balloon dilation (CBD), botulinum toxin injection, and cricopharyngeal myotomy rehabilitation [5]. A previous study evaluated the efficacy of a cricopharyngeal dysfunction rehabilitation protocol in which patients performed a voluntary, task-oriented swallowing exercise guided by a balloon with graded volumes. This balloon, which traverses the cricopharyngeus muscle during voluntary swallowing, moves as the muscle opens, in contrast to passive dilation, which has been shown to be less effective [6]. This approach resulted in long-term improvements in swallowing function, as evidenced by increased functional oral intake scale (FOIS) scores, enhanced cricopharyngeus muscle opening, and greater hyoid bone excursions, all measured via videofluoroscopy [7]. Additionally, manometry studies confirmed its efficacy in prolonging cricopharyngeus muscle relaxation time, strengthening pharyngeal propulsion, and restoring resting pressure of the cricopharyngeus muscle [8,9]. These results suggest that the observed improvements in swallowing and cricopharyngeal muscle function are attributed not only to mechanical changes in the cricopharyngeal sphincter but also to neuroplastic changes upstream. This hypothesis underpins the current investigation into the effects of combined CBD therapy on neural excitability in individuals with dysphagia following stroke. NMES is a form of low-frequency current stimulation that delivers predetermined electrical impulses of appropriate intensity to the neuromuscular junction or motor endplate. This stimulation induces depolarization of the axonal membrane in peripheral motor neurons, thereby generating action potentials that propagate along the axons to the muscle fibers. Through excitation-contraction coupling, NMES elicits muscle contractions or simulates voluntary motor activity, ultimately aiming to improve or restore the function of the stimulated muscle or muscle groups [10]. Furthermore, low-frequency electrical stimulation can activate ascending afferent pathways in sensory neurons, triggering reflex arcs and enhancing cortical electrical input. This mechanism plays a critical role in the re-establishment and recovery of swallowing reflex control, as well as in promoting functional reorganization of the motor cortex [10]. In addition, NMES has been shown to improve blood circulation in swallowing-related structures, facilitate the recovery of voluntary movement and sensory function in the orofacial and pharyngeal regions, and prevent disuse atrophy of the muscle groups involved in swallowing [11]. Electroencephalographic studies have demonstrated that both passive NMES alone and NMES combined with voluntary muscle contraction training significantly enhance cortical activity, with the latter inducing a markedly greater effect than NMES alone [12]. The enhanced efficacy observed with the combined approach may be attributed to additional stimulation involving the primary somatosensory cortex. This effect is likely due to the involvement of higher-order cognitive cortical control required during combined therapy, which may facilitate improved neuromuscular control of the stimulated skeletal muscles [12]. Transcranial magnetic stimulation (TMS) is a noninvasive technique used to assess treatment-induced neuroplastic changes. The amplitude of motor evoked potentials (MEP) induced by TMS is a well-established and reliable method for evaluating the impact of swallowing interventions on corticobulbar excitability [13]. Recent studies have shown that the amplitude of affected submental MEP evoked by ipsilateral cortical pulses significantly differs between dilation and control groups, suggesting that CBD therapy enhances excitability in the affected projections of patients with unilateral brainstem stroke [14].
The videofluorographic swallowing study (VFSS) is one of method to evaluate swallowing. Also known as the modified barium swallowing test, it is often considered the “criterion standard” to diagnose dysphagia by most swallowing clinicians [15]. Various volumes and textures of food and liquid are administered, and clinical impressions of the presence and degree of swallowing impairment are obtained from the radiographic images. Judgments are also made regarding the coordination and timing of swallowing events by this method [16]. FOIS is an observer-rated ordinal scale used to assess oral intake, with scores ranging from 1 (indicating the most severe impairment) to 7 (representing normal oral intake). It is primarily used to evaluate the level of oral intake in patients with swallowing disorders. A score of ≤5 on the FOIS indicates the presence of dysphagia, meaning that the patient is unable to consume regular food or requires modified diets or alternative feeding methods [17]. Postoperative dysphagia following microvascular decompression is clinically rare. To enhance recognition of this condition and to provide a series of effective rehabilitation strategies, we report and discuss this case in detail.
Case Report
NUTRITIONAL MANAGEMENT:
The patient’s daily caloric requirement was estimated to be approximately 9211–12979 kJ based on “Clinical Practice Guidelines for Oropharyngeal Dysphagia” [21]. This was converted into equivalent food portions: 100 g of eggs, 200 g of lean pork, 100 g of fish, 300 g of rice, and 500 g of vegetables, or other foods with similar caloric and nutritional content. The family was instructed to prepare the food into a puree using a blender and administer it via a nasogastric tube in 3 meals a day. Based on the patient’s assessment results, the feeding method was adjusted as needed. When oral intake is possible, the European Society for Swallowing Disorders’ volume-viscosity swallowing test guidelines were referenced [22]. The family was advised to offer 5 mL per mouthful as a safe swallowing volume, with each mouthful to be swallowed before the next. Water intake was provided via nasogastric tube at 200 to 300 mL per session, 4 to 5 times per day, with a 3-h interval between each. The water amount could be adjusted based on the liquid content in the solid foods provided at each meal.
SWALLOWING TRAINING:
Swallowing training involved oropharyngeal muscle strengthening exercises, sensory stimulation, and tongue retraction exercises. The exercises focused on improving muscle strength, resistance, or both. For example, tongue exercises required the patient to hold the tongue gently between the teeth and then swallow saliva while maintaining the tongue in a straight position [23]. Other techniques included the Mendelsohn maneuver and Shaker exercises [24], as well as oral taste training, temperature training, and proprioception stimulation through food additives, ice cubes, and air pulses for 10 min.
CBD SYNCHRONIZED NMES:
VitalStim neuromuscular electrical stimulation equipment (Chattanooga Ltd, Hixson, TN, USA) was used for this patient. Prior to treatment, the patient’s neck skin was cleaned with 75% medical alcohol (or saline for those allergic to alcohol), to reduce interference and improve conductivity. The treatment electrodes were placed on both sides of the anterior neck, between the chin and the upper part of the suprahyoid muscles. Before starting CBD synchronized NMES, the nasogastric tube was removed. A 14 Fr balloon catheter was inserted through the patient’s nostrils into the esophagus. At the esophageal inlet, water was gradually injected into the balloon in accordance with the patient’s dilation tolerance (refer to Table 2 for volume). The patient was instructed to perform a swallowing action as the intensity of electrical stimulation on the suprahyoid muscles reached its peak at the same time. The balloon was then swallowed, and the therapist gently retracted the balloon, repeating the process multiple times. This intermittent traction of the cricopharyngeus muscle was designed to progressively dilate the cricopharyngeal muscle. Each session lasted 20 min, once daily, for a total of 10 sessions. This case report was written in accordance with the SCARE guidelines [25].
Discussion
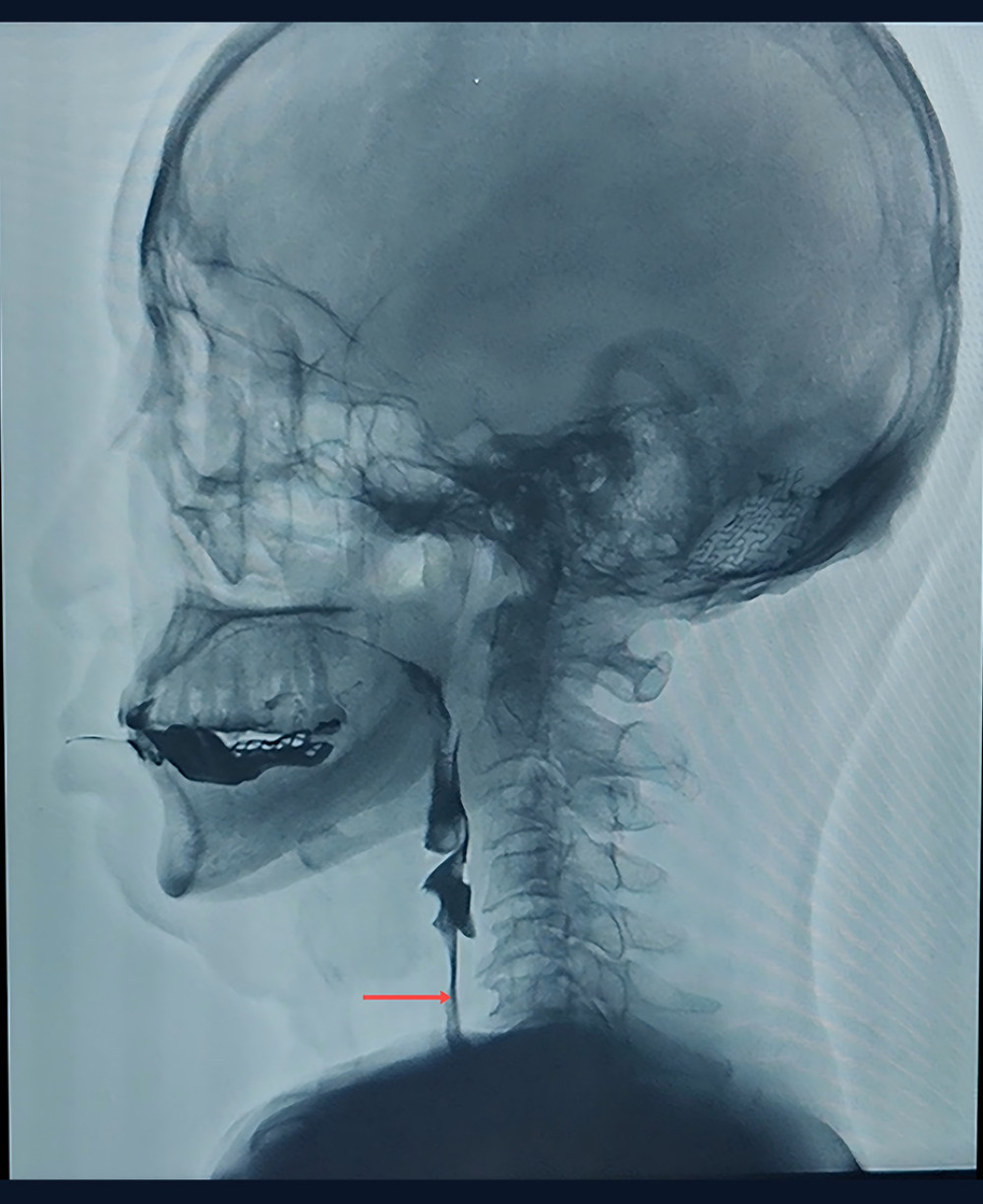
In this case, post-treatment assessments showed improvements in swallowing function. VFSS revealed increased cricopharyngeus muscle opening and successful passage of the bolus (see Figures 1, 2). The issues of cricopharyngeus muscle relaxation, insufficient tongue-pharyngeal complex movement, poor epiglottic inversion, and delayed laryngeal closure were all markedly improved. The FOIS score reached level 6, indicating complete oral intake with no special preparation required, although occasional coughing still occurred with drinking.
The patient developed dysphagia after undergoing microvascular decompression for hemifacial spasm. Glossopharyngeal nerve palsy is a potential cause of the dysphagia and is considered a rare postoperative complication. The primary symptoms included dysphagia, aspiration, and choking. The assessment revealed several issues, including the absence of the pharyngeal reflex, impaired cricopharyngeus muscle relaxation, bolus leakage, aspiration, insufficient tongue-pharyngeal complex movement, poor epiglottic inversion, delayed laryngeal closure, insufficient pharyngeal peristalsis, and pharyngeal contraction. These findings indicate a primarily pharyngeal-phase neurogenic dysphagia. Based on these characteristics, a comprehensive rehabilitation approach combining CBD and synchronous NMES of the suprahyoid muscles was developed. Research on this synchronous therapy is rare. However, CBD has been confirmed as effective in treating cricopharyngeal dysfunction caused by various neurological conditions, like stroke and traumatic brain injury [26]. Moreover, the nasally inserted CBD catheter avoids further restricting the patient’s tongue movement, which would be a concern with an oral insertion method.
A recent study has shown that CBD improves swallowing function via 2 mechanisms. One is passive dilation, which increases muscle compliance by mechanical stretching, promoting the elongation of muscle fibers and reducing the opening resistance of the cricopharyngeus muscle. The other is active dilation, in which the patient actively swallows during balloon inflation, triggering the active contraction of the suprahyoid muscles, resulting in upward and forward movement of the tongue-pharyngeal complex [27]. This active movement helps stretch the cricopharyngeus muscle and facilitates its opening. By stimulating the local muscles and training the opening and closing of the cricopharyngeus muscle, the therapy activates both sides of the cortical areas and rebuilds the cortical-brainstem swallowing reflex pathway, ultimately promoting swallowing recovery [27].
In the present case, the patient’s FOIS improved from level 1 to level 6, with marked reductions in aspiration and choking. The post-treatment activation effect, which promotes swallowing recovery, was reflected in the MEP of the suprahyoid muscles on both sides, as induced by TMS. CBD-induced dilation likely reconstructs or repairs the damaged neuromuscular connections of the cortical pathways, modulating neuroplasticity and leading to increased bilateral MEP after treatment, which correlated with positive therapeutic outcomes. These findings align with previous research in which patients with aspiration often show a decline in ipsilateral and contralateral MEPs, as opposed to patients without aspiration [18]. Karatzetzou et al [28] further explored the correlation between the MEP of the suprahyoid muscles and swallowing function after stroke and found that MEP amplitudes were significantly associated with the severity of dysphagia.
NMES enhances the strength and coordination of swallowing-related muscles by reversing the typical motor unit recruitment order – preferentially activating fast-twitch type II muscle fibers. In the present case, NMES was applied synchronously with CBD to facilitate cricopharyngeal muscle opening. The electrically induced rapid contraction of the suprahyoid muscles contributed to mechanical traction on the cricopharyngeus, augmenting the effect of balloon dilation [29]. This combined intervention not only achieves mechanical expansion but also leverages NMES-induced muscle training effects and improves local blood circulation to compensate for suprahyoid muscle weakness, which is often associated with reduced pharyngeal motility and impaired swallowing function. Furthermore, NMES activates afferent sensory pathways via stimulation of the glossopharyngeal, trigeminal, and vagus nerves, thereby enhancing swallowing central pattern generator responsiveness and promoting neural reorganization essential for swallowing recovery [11].
Electroencephalographic studies have shown that NMES combined with volitional muscle contraction induces greater cortical activation – particularly within the primary sensory cortex – than does passive NMES alone. This enhanced cortical engagement likely facilitates improved control of stimulated skeletal muscles and promotes neuroplasticity, contributing to the functional restoration of deglutition [29].
A previous study has shown that combining CBD with NMES for the treatment of dysphagia in patients following nasopharyngeal cancer radiation resulted in more significant improvements in swallowing function than did either treatment method alone [30]. This finding further supports the effectiveness of this combined approach for managing dysphagia.
Conclusions
Although swallowing disorders after microvascular decompression for hemifacial spasm are rare, their occurrence can significantly affect a patient’s quality of life. Clinically, a comprehensive rehabilitation approach combining catheter balloon dilation with synchronous neuromuscular electrical stimulation NMES of the suprahyoid muscles may offer a promising and effective treatment strategy to rapidly alleviate the patient’s distress.

References
1. Chaudhry N, Srivastava A, Joshi L, Hemifacial spasm: The past, present and future: J Neurol Sci, 2015; 356(1–2); 27-31
2. Xiang G, Sui M, Jiang N, The progress in epidemiological, diagnosis and treatment of primary hemifacial spasm: Heliyon, 2024; 10(19); e38600
3. Luzzi S, Del Maestro M, Trovarelli D, Endoscope-assisted microneurosurgery for neurovascular compression syndromes: Basic principles, methodology, and technical notes: Asian J Neurosurg, 2019; 14(1); 193-200
4. Blue R, Li C, Spadola M, Complication rates during endoscopic microvascular decompression surgery are low with or without petrosal vein sacrifice: World Neurosurg, 2020; 138; e420-e25
5. Kocdor P, Siegel ER, Tulunay-Ugur OE, Cricopharyngeal dysfunction: A systematic review comparing outcomes of dilatation, botulinum toxin injection, and myotomy: Laryngoscope, 2016; 126(1); 135-41
6. Yabunaka K, Konishi H, Nakagami G, Videofluoroscopy-guided balloon dilatation for treatment of severe pharyngeal dysphagia: Diagn Interv Radiol, 2015; 21(2); 173-76
7. Dou Z, Zu Y, Wen H, The effect of different catheter balloon dilatation modes on cricopharyngeal dysfunction in patients with dysphagia: Dysphagia, 2012; 27(4); 514-20
8. Lan Y, Xu GQ, Dou ZL, Effect of balloon dilatation on upper esophageal sphincter in brainstem stroke patients with dysphagia: an investigation using high-resolution solid-state manometry: Zhonghua Yi Xue Za Zhi, 2013; 93(33); 2631-36
9. Lan Y, Xu G, Dou Z, Biomechanical changes in the pharynx and upper esophageal sphincter after modified balloon dilatation in brainstem stroke patients with dysphagia: Neurogastroenterol Motil, 2013; 25(12); e821-29
10. Diehl P, Kliesch U, Dietz V, Impaired facilitation of motor evoked potentials in incomplete spinal cord injury: J Neurol, 2006; 253(1); 51-57
11. Kim E, Wu F, Wu X, Generation of craniofacial myogenic progenitor cells from human induced pluripotent stem cells for skeletal muscle tissue regeneration: Biomaterials, 2020; 248; 119995
12. Bickel CS, Gregory CM, Dean JC, Motor unit recruitment during neuromuscular electrical stimulation: A critical appraisal: Eur J Appl Physiol, 2011; 111(10); 2399-407
13. Michou E, Hamdy S, Harris M, Characterization of corticobulbar pharyngeal neurophysiology in dysphagic patients with Parkinson’s disease: Clin Gastroenterol Hepatol, 2014; 12(12); 2037.45e1-4
14. Wei X, Yu F, Dai M, Change in excitability of cortical projection after modified catheter balloon dilatation therapy in brainstem stroke patients with dysphagia: A prospective controlled study: Dysphagia, 2017; 32(5); 645-56
15. Fransson J, Thorén S, Selg J, Validity and reliability of dysphagia outcome severity scale (DOSS) when used to rate flexible endoscopic evaluations of swallowing (FEES): Dysphagia, 2025; 40(2); 343-52
16. Matsuo K, Palmer JB, Video fluoroscopic techniques for the study of Oral Food Processing: Curr Opin Food Sci, 2016; 9; 1-10
17. Crary MA, Mann GD, Groher ME, Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients: Arch Phys Med Rehabil, 2005; 86(8); 1516-20
18. Gallas S, Moirot P, Debono G, Mylohyoid motor-evoked potentials relate to swallowing function after chronic stroke dysphagia: Neurogastroenterol Motil, 2007; 19(6); 453-58
19. Alcantara CC, García-Salazar LF, Silva-Couto MA, Post-stroke BDNF concentration changes following physical exercise: A systematic review: Front Neurol, 2018; 9; 637
20. Hoogendam JM, Ramakers GM, Di Lazzaro V, Physiology of repetitive transcranial magnetic stimulation of the human brain: Brain Stimul, 2010; 3(2); 95-118
21. Yang S, Park JW, Min K, Clinical practice guidelines for oropharyngeal dysphagia: Ann Rehabil Med, 2023; 47(Suppl 1); S1-S26
22. Rofes L, Arreola V, Clavé P, The volume-viscosity swallow test for clinical screening of dysphagia and aspiration: Nestle Nutr Inst Workshop Ser, 2012; 72; 33-42
23. Bath PM, Lee HS, Everton LF, Swallowing therapy for dysphagia in acute and subacute stroke: Cochrane Database Syst Rev, 2018; 10(10); CD000323
24. Mendelsohn MS, McConnel FM, Function in the pharyngoesophageal segment: Laryngoscope, 1987; 97(4); 483-89
25. Sohrabi C, Mathew G, Maria N, The SCARE 2023 guideline: Updating consensus Surgical CAse REport (SCARE) guidelines: Int J Surg, 2023; 109(5); 1136-40
26. Solt J, Bajor J, Moizs M, Primary cricopharyngeal dysfunction: treatment with balloon catheter dilatation: Gastrointest Endosc, 2001; 54(6); 767-71
27. Arenaz Búa B, Olsson R, Westin U, Treatment of cricopharyngeal dysfunction: A comparative pilot study: BMC Res Notes, 2015; 8; 301
28. Karatzetzou S, Tsiptsios D, Terzoudi A, Transcranial magnetic stimulation implementation on stroke prognosis: Neurol Sci, 2022; 43(2); 873-88
29. Zhang Q, Wu S, Effects of synchronized neuromuscular electrical stimulation (NMES) on the submental muscles during ingestion of a specified volume of soft food in patients with mild-to-moderate dysphagia following stroke: Med Sci Monit, 2021; 27; e928988
30. Long YB, Wu XP, A randomized controlled trail of combination therapy of neuromuscular electrical stimulation and balloon dilatation in the treatment of radiation-induced dysphagia in nasopharyngeal carcinoma patients: Disabil Rehabil, 2013; 35(6); 450-54
Figures
Tables
 Table 1. Comparison of functional assessment before and after treatment.
Table 1. Comparison of functional assessment before and after treatment. Table 2. The volume of water administered per catheter balloon dilation treatment.Table 1. Comparison of functional assessment before and after treatment.Table 2. The volume of water administered per catheter balloon dilation treatment.
Table 2. The volume of water administered per catheter balloon dilation treatment.Table 1. Comparison of functional assessment before and after treatment.Table 2. The volume of water administered per catheter balloon dilation treatment. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133