16 December 2025: Articles 
Subdural Empyema and Pneumocephalus From Chronic Polypoid Sinusitis in an Elderly Woman With Rapid Neurological Recovery: A Report of a Rare Case
Challenging differential diagnosis, Management of emergency care, Rare coexistence of disease or pathology
John Martinez ABCDEF 1*, Elizabeth Nagidi BCEF 1, Mark RigbyDOI: 10.12659/AJCR.949999
Am J Case Rep 2025; 26:e949999






Abstract
BACKGROUND: Subdural empyema (SDE) is a rare, life-threatening intracranial infection characterized by pus accumulation between the dura and arachnoid mater. It is most commonly associated with sinusitis, typically affecting young males. The presence of pneumocephalus without trauma or surgery is exceedingly rare and should raise concern for intracranial infection. Early diagnosis through neuroimaging and prompt multidisciplinary intervention are crucial for preventing morbidity and mortality.
CASE REPORT: We present a case of SDE and atraumatic pneumocephalus in a 76-year-old woman who was found unresponsive at home. Laboratory tests revealed leukocytosis, elevated inflammatory markers, and fever. Non-contrast computed tomography (CT) showed a 2-3 mm subdural collection with intracranial air foci, along with evidence of otitis media, mastoiditis, and pansinusitis. Lumbar puncture revealed xanthochromic cerebrospinal fluid (CSF) with elevated protein and white blood cells (WBC). Streptococcus pneumoniae was confirmed by CSF culture and urine antigen. She underwent emergency craniotomy, draining 75 cc of purulent material, followed by the ear, nose, and throat (ENT) intervention with maxillary antrostomy, ethmoidectomy, and tympanostomy. She experienced a full neurological recovery.
CONCLUSIONS: This case underscores the importance of high clinical suspicion and early imaging in elderly patients with altered mental status and sinus pathology. Atraumatic pneumocephalus in non-surgical patients may signal severe intracranial infection. Timely, multidisciplinary management led to rapid recovery, and this case adds to the limited literature on pneumococcal SDE with pneumocephalus in elderly women with chronic sinusitis.
Keywords: Craniotomy, Empyema, Subdural, infections, Pneumocephalus, Sinusitis, Streptococcus pneumoniae, Humans, Female, Aged, Tomography, X-Ray Computed, Chronic Disease, Pneumococcal Infections
Introduction
SDE is a rare but potentially devastating complication of intracranial infection, marked by the accumulation of purulent material between the dura and arachnoid mater [1]. The condition is typically secondary to contiguous infections such as sinusitis, otitis media, or mastoiditis [1,2]. SDE is more common in males in the second decade of life, with a 3: 1 ratio of affected males to females [3]. Early diagnosis and aggressive treatment are critical, as untreated SDE carries a mortality rate exceeding 40% [4]. However, with advances in imaging and early neurosurgical intervention, mortality rates have significantly decreased to below 10% [4]. Notably, the presence of pneumocephalus in the absence of trauma or recent surgical intervention is extremely rare, occurring in approximately 7% of cases [5]. It should raise concern for infectious etiologies, particularly when seen in conjunction with signs of sinus or middle ear disease [6]. Intracranial gas formation can occur due to gas-forming organisms, rapid tissue necrosis, or air tracking from infected paranasal sinuses or mastoid air cells [7,8]. CT imaging remains the cornerstone of early detection, often revealing crescentic subdural collections, meningeal enhancement, and, in rare cases such as our patient, minute foci of intracranial air [9]. Magnetic resonance imaging (MRI) can offer further characterization, especially in the presence of subtle cortical or subdural abnormalities.
This report aims to contribute to the limited literature on atraumatic pneumocephalus and pneumococcal subdural empyema secondary to sinusitis in the elderly. Given the unusual presentation and successful outcome, this case has potential implications for improving the early recognition of intracranial complications in chronic sinusitis and for addressing altered mental status in the elderly population. It also underscores the importance of including rare infectious etiologies in differential diagnoses when atraumatic pneumocephalus is detected. Further studies are warranted to explore predictive imaging findings, optimize diagnostic algorithms, and evaluate the role of multidisciplinary management strategies in enhancing patient outcomes.
Case Report
A 76-year-old Black woman with a medical history significant for diabetes mellitus presented to the emergency department (ED) after being found unresponsive in her bed. According to her family, she had been in her usual state of health the day prior, performing all activities of daily living independently and exhibiting no symptoms. The next morning, she was discovered unresponsive but with an intact pulse and was protecting her airway. Emergency medical services (EMS) transported her promptly to the ED.
On arrival, she was hemodynamically stable, saturating well on room air, and continued to protect her airway. She was febrile to 40.3°C and unresponsive, prompting a Code Stroke activation. Initial non-contrast brain computed tomography (CT) (Figures 1, 2) demonstrated a thin isodense-to-hypodense subdural collection over the right cerebral convexity without mass effect or intraparenchymal hemorrhage. Notably, small specks of intracranial air were present over the same region, raising concern for possible infection versus venous air embolus (Figure 3).
Computed tomography angiography (CTA) of the head and neck showed no significant vascular stenosis. CT perfusion imaging revealed a Tmax delay of more than 4 s in the right temporal-parietal region, concerning for possible ischemia; an MRI of the brain was recommended for further evaluation. However, at the time of the MRI, the patient was unable to stay still and therefore could not complete the imaging.
Laboratory evaluation revealed leukocytosis (27.56 K/cmm), elevated lactic acid (3.7 mmol/L), low magnesium (1.4 mg/dL), elevated troponin (0.22 ng/mL), and mild brain natriuretic peptide (BNP) elevation (643 pg/mL). Thyroid-stimulating hormone (TSH) was within normal limits. Electrocardiography (EKG) (Figure 4) showed sinus tachycardia at 128 bpm without ischemic changes. Chest X-ray showed a left lower-lung base infiltrate, raised concern for pneumonia, and urinalysis suggested a possible urinary tract infection (minimal white blood cells [WBC], small leukocyte esterase, negative for nitrate, and moderate red blood cells [RBC]). Clinically, the patient appeared acutely ill, was nonverbal, fidgeting, and showed signs of photophobia and nuchal rigidity. Her pupils were equal and reactive to light, and there was no evidence of external trauma noted; the tympanic membrane could not be visualized due to cerumen; and the tongue appeared enlarged. Her lungs were clear to auscultation without accessory muscle use; the rest of the physical examination was unremarkable.
A full septic workup was initiated, including blood, urine, and sputum cultures. Broad-spectrum antibiotics (Vancomycin, Piperacillin/tazobactam, Metronidazole, Ampicillin, ceftriaxone, and acyclovir) were started empirically to cover suspected meningitis, community-acquired pneumonia, and urinary tract infection. Neurology was consulted, and a lumbar puncture (LP) was recommended. Urine antigen testing returned positive for
Later that evening, a lumbar puncture (LP) was performed and yielded xanthochromic fluid with the following results: CSF glucose 53 mg/dL, protein >400 mg/dL, RBC 5480/μL, WBC 56/μL. CSF culture later confirmed
Postoperative CT brain and maxillofacial imaging with and without contrast (Figure 5) revealed right maxillary sinusitis and bilateral ethmoidal air cell mastoiditis. Ear, Nose, and Throat (ENT) was consulted on the day of admission; however, due to the patient’s urgent and unstable condition, imaging was deferred until after the craniotomy. Once the patient was hemodynamically stable, the ENT specialist proceeded with a sinus endoscopy, which included a right maxillary antrostomy, a right total ethmoidectomy, and a right tympanostomy with pressure-equalizing (PE) tube placement. These procedures were performed 2 days after the initial surgery.
Throughout her hospitalization, the patient showed significant clinical improvement. Repeat CT brain 7 days after the intervention (Figure 6) showed significant resolution of the previously observed pneumocephalus and a small hypoattenuating fluid collection beneath the right frontal craniotomy, consistent with post-surgical changes. She was successfully extubated and transitioned from the ICU to a medical ward, with progressive neurologic recovery. She became fully responsive, able to follow commands, engage in physical therapy, and tolerate oral intake. She was ultimately transferred to an inpatient rehabilitation facility in stable condition and with no residual neurological deficits.
Discussion
RARITY AND CLINICAL SIGNIFICANCE:
SDE is a rare yet potentially life-threatening intracranial infection, accounting for approximately 10–20% of all intracranial infections [4]. It is classically associated with contiguous infections, such as sinusitis, otitis media, or mastoiditis, and is more common in younger males [3,4]. In elderly patients, especially females, such presentations are exceptionally uncommon. Even more rare is the occurrence of atraumatic pneumocephalus, particularly in the absence of trauma or recent surgical procedures. Reports indicate that intracranial air is seen in only 7% of SDE cases, underscoring the diagnostic challenge [5,15].
The presence of pneumocephalus in our elderly female patient, without preceding trauma or surgery, highlighted an unusual and underrecognized pattern of presentation. While frontal and ethmoidal sinus infections are commonly implicated in SDE, the chronic polypoid form of sinusitis is especially insidious and often overlooked until neurological complications arise [13]. This case aligns with prior reports, such as that by Eça et al, which described subdural empyema and pneumocephalus following sinusitis, although their patient was younger and male, demonstrating how our case expands the demographic and clinical spectrum of such presentations [7]. Only a handful of such cases have been reported in the literature globally, particularly involving Streptococcus pneumoniae as the causative agent of both SDE and meningitis in elderly adults [10,11,13,15]. A 2019 case series by Saleem et al also noted the rarity of pneumocephalus as a presenting sign in non-traumatic subdural empyema, yet none of their cases involved elderly women with polypoid sinusitis, as presented here [15].
DIAGNOSTIC EVALUATION AND IMAGING FINDINGS:
Our patient presented with fever, altered mental status, and nuchal rigidity, classic signs suggestive of central nervous system infection. Initial non-contrast CT imaging revealed crescentic subdural collections and small intracranial air pockets over the right cerebral convexity. These radiologic findings are hallmark features of SDE, especially when accompanied by meningeal enhancement and sinus disease [17,18].
The detection of discrete intracranial air foci, as seen in this case, may signal infection with gas-producing organisms or air tracking from infected sinuses or mastoid air cells [19,20]. In the absence of trauma, this finding should prompt urgent investigation for infectious causes. Lumbar puncture confirmed Streptococcus pneumoniae meningitis, corroborated by urine antigen testing and CSF culture, further supporting the diagnosis of infectious subdural empyema [10,12].
CT imaging is crucial for early recognition and surgical planning. Studies have shown that minute intracranial gas specks, although rare, are key diagnostic clues that can help differentiate infectious causes from trauma or postoperative pneumocephalus [5,15,21]. This emphasizes the importance of detailed radiologic evaluation, particularly in patients with sinus pathology and altered mental status.
TREATMENT RATIONALE AND OUTCOME:
Immediate broad-spectrum antimicrobial therapy was initiated to address suspected meningoencephalitis and sepsis. Given the radiologic concern for empyema, Neurosurgery was promptly consulted, and the patient underwent emergency craniotomy with evacuation of 75 cc of purulent material. The subsequent ENT intervention, including maxillary antrostomy, ethmoidectomy, and tympanostomy, targeted the likely source of infection and helped prevent recurrence [16,13].
The patient had rapid neurological recovery, with complete resolution of pneumocephalus on follow-up imaging. This favorable outcome highlights the crucial role of early multidisciplinary intervention, including Neurosurgery, Infectious Disease, ENT, and Critical Care teams, in managing complex intracranial infections [14]. Clinicians encountering similar cases should maintain a high index of suspicion for intracranial infection in elderly patients presenting with sinus disease and altered mental status, particularly when pneumocephalus is identified in the absence of trauma. Prompt neuroimaging with CT should be followed by lumbar puncture when deemed safe, and early consultation with Neurosurgery and ENT is essential for timely intervention. Empiric antibiotic regimens should provide broad-spectrum coverage, including anaerobes, with subsequent de-escalation based on culture results. Repeat imaging plays a critical role in monitoring treatment response and confirming the resolution of intracranial gas.
Additionally, subdural empyema can be complicated by septic cerebral venous sinus thrombosis (CVST), a condition that increases the risk of infarction and hemorrhage. While not observed in this patient, the literature supports the use of anticoagulation in such scenarios, provided infection control is achieved [22].
Conclusions
This case illustrated an exceptionally rare presentation of subdural empyema with atraumatic pneumocephalus in an elderly woman with chronic polypoid sinusitis. The identification of minute intracranial air foci over the right cerebral convexity, in the absence of trauma or prior neurosurgical intervention, is exceedingly uncommon and raises early concern for infectious intracranial extension. Further imaging and CSF studies confirmed the diagnosis of pneumococcal meningitis complicated by subdural empyema. A multidisciplinary approach, combined with emergent neurosurgical evacuation and ENT-directed sinus surgery, led to a full neurological recovery. This case emphasizes the critical role of early imaging and a multidisciplinary approach in managing rare intracranial complications of chronic sinusitis, particularly in atypical patient populations. The findings contribute to the limited body of literature documenting atraumatic pneumocephalus as an initial radiologic clue to severe intracranial infection.
Figures
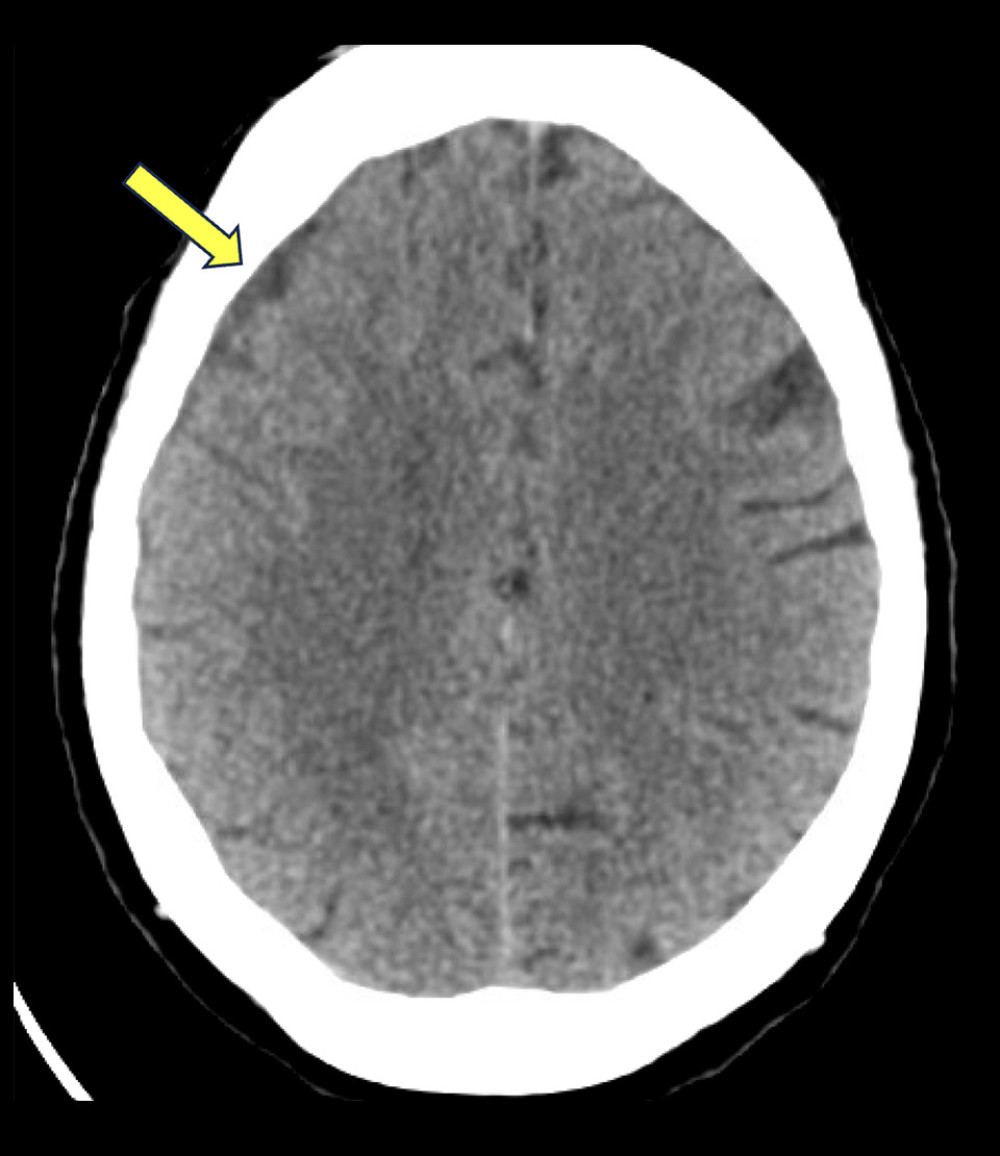 Figure 1. Increased density in the extra-axial space is seen on initial CT brain without contrast, most commonly seen in subdural hematoma.
Figure 1. Increased density in the extra-axial space is seen on initial CT brain without contrast, most commonly seen in subdural hematoma. 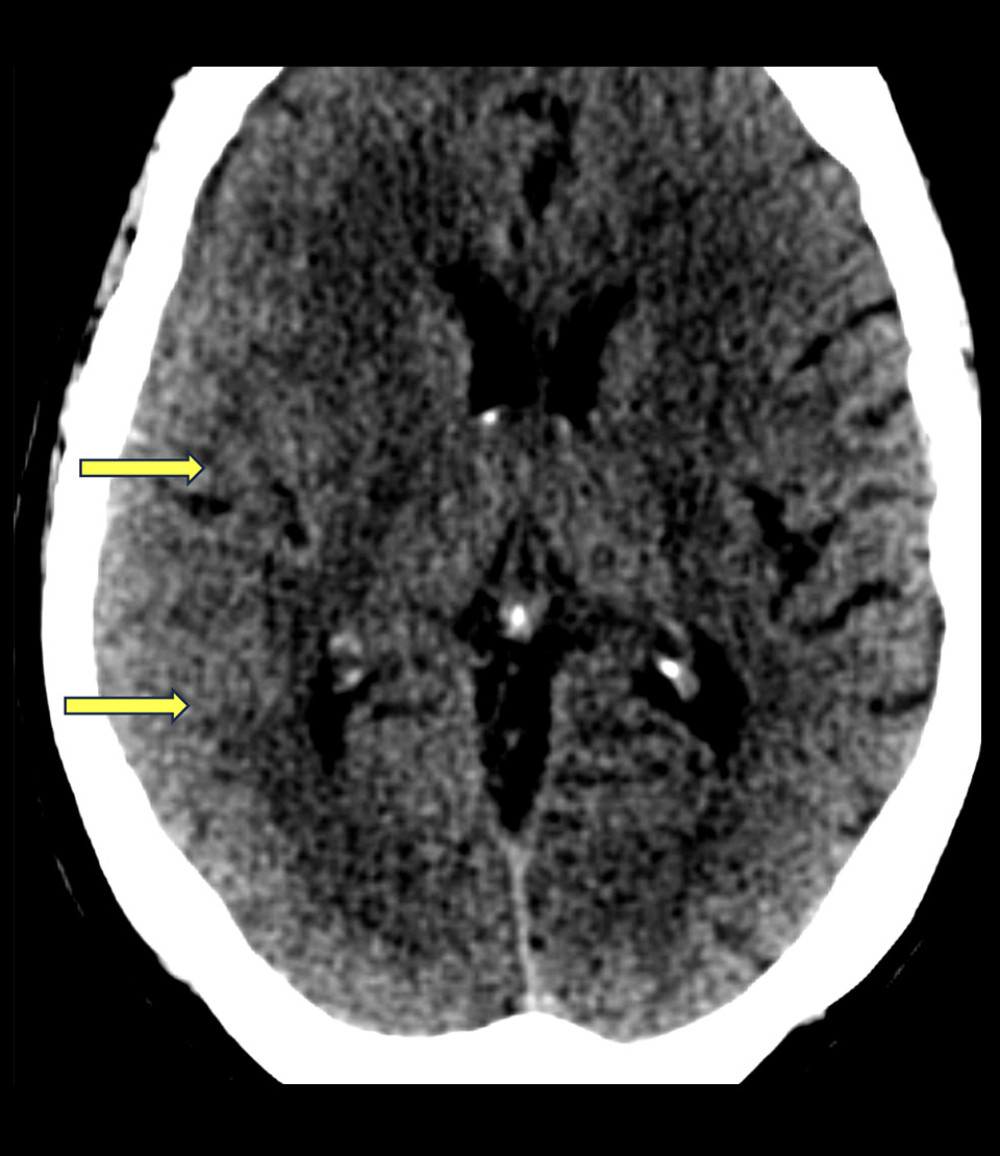 Figure 2. Abnormal soft tissue is observed in the brain on the initial CT scan of the brain without contrast. Sulcal effacement is seen in the right posterior temporal and occipital regions.
Figure 2. Abnormal soft tissue is observed in the brain on the initial CT scan of the brain without contrast. Sulcal effacement is seen in the right posterior temporal and occipital regions. 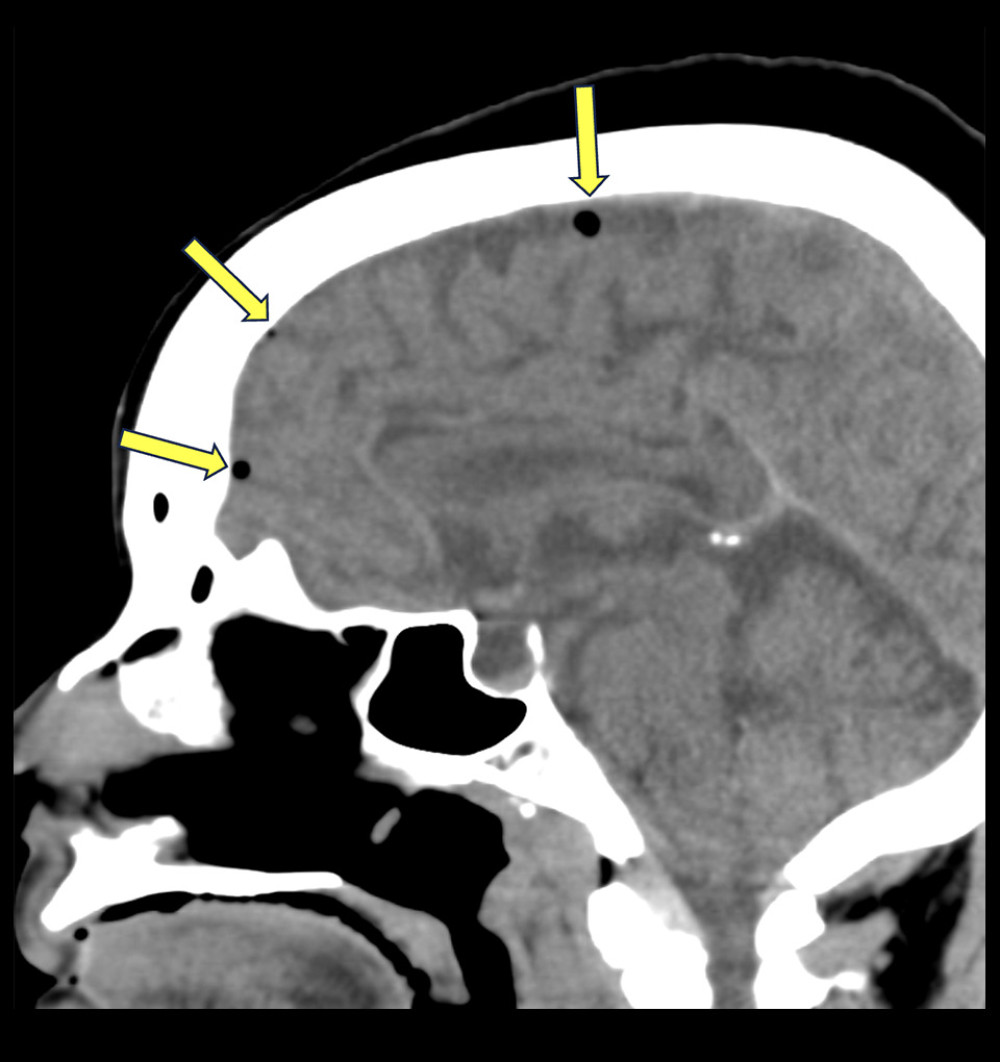 Figure 3. Pneumocephalus is visible in the extra-axial space on the initial CT scan of the brain without contrast, most often due to venous air embolus.
Figure 3. Pneumocephalus is visible in the extra-axial space on the initial CT scan of the brain without contrast, most often due to venous air embolus. 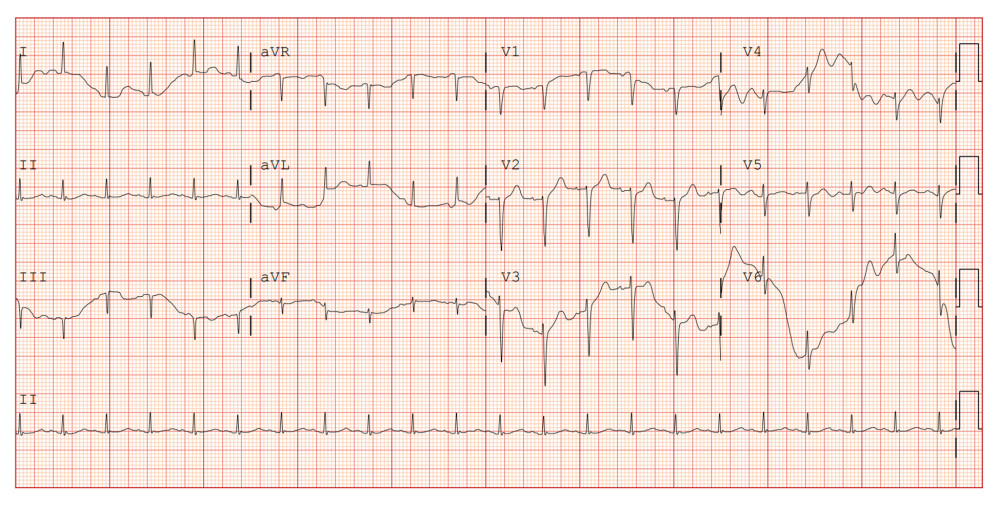 Figure 4. EKG showed sinus tachycardia at 128 beats per minute (bpm) without ischemic changes.
Figure 4. EKG showed sinus tachycardia at 128 beats per minute (bpm) without ischemic changes. 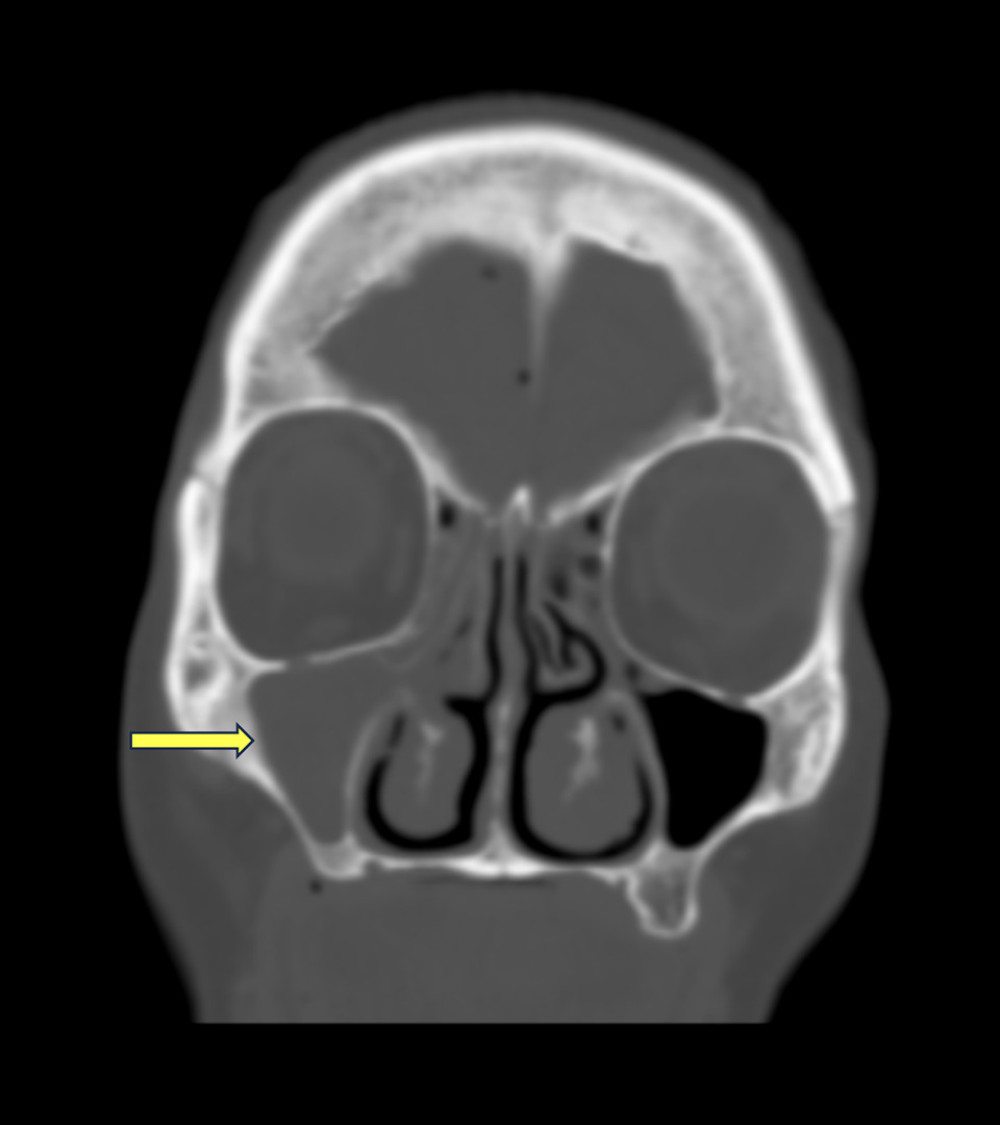 Figure 5. Complete opacification of the right maxillary sinus is seen on initial CT of the brain without contrast. Mucosal thickening and right sinus hypoplasia are also seen.
Figure 5. Complete opacification of the right maxillary sinus is seen on initial CT of the brain without contrast. Mucosal thickening and right sinus hypoplasia are also seen. 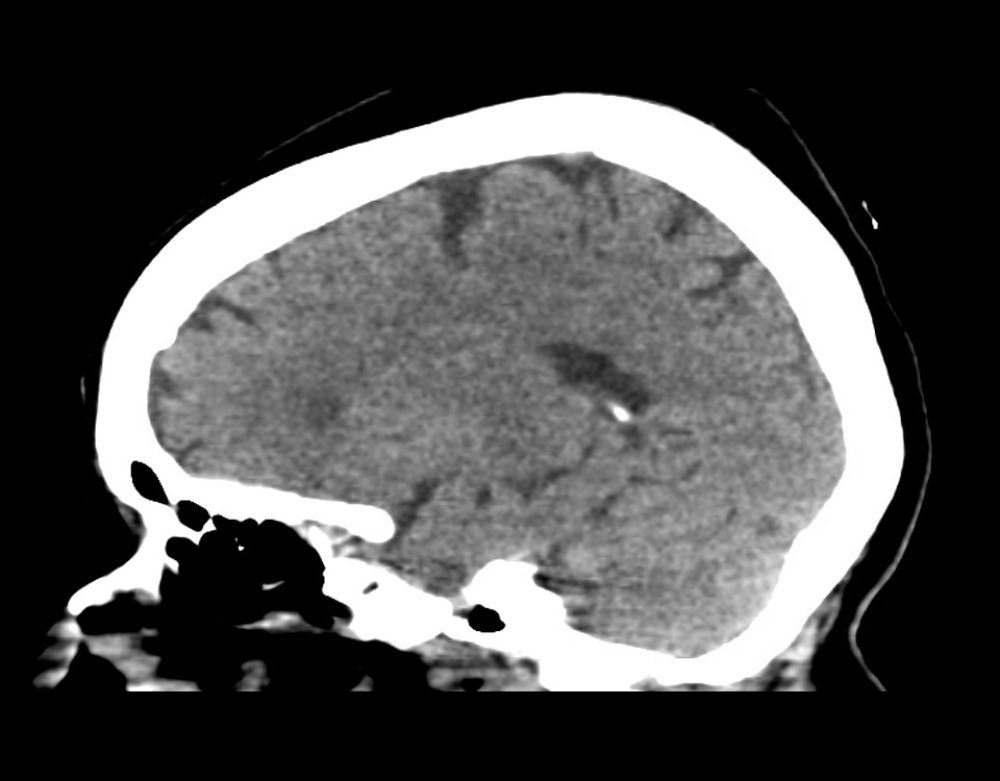 Figure 6. CT brain after right frontal craniotomy without contrast. Interval resolution of previously present small-volume right frontal pneumocephalus.
Figure 6. CT brain after right frontal craniotomy without contrast. Interval resolution of previously present small-volume right frontal pneumocephalus. References
1. Nathoo N, Nadvi SS, Narotam PK, van Dellen JR, Brain abscess: Management and outcome analysis of a computed tomography era experience with 973 patients: World Neurosurg, 2011; 75(5–6); 716-26
2. Muzumdar D, Jhawar S, Goel A, Brain abscess: An overview: Int J Surg, 2011; 9(2); 136-44
3. Hall WA, Subdural empyema: StatPearls [Internet], 2024, National Library of Medicine https://www.ncbi.nlm.nih.gov/books/NBK557829/
4. Agrawal A, Timothy J, Pandit L, Shetty L, A review of subdural empyema and its management: Infect Dis Clin Pract, 2007; 15(3); 149-53
5. Gelabert-Gonzalez M, Spontaneous pneumocephalus: Neurocirugía, 2005; 16(2); 152-56
6. Yilmazlar S, Arslan E, Kocaeli H, Cerebral subdural empyema: Analysis of 45 cases: Br J Neurosurg, 2006; 20(5); 346-56
7. Eça K, Guimarães J, Vaz R, Subdural empyema with pneumocephalus following sinusitis: A case report and review of literature: Acta Med Port, 2024; 37(1); 63-66
8. Zimmerman RA, Bilaniuk LT, Dolinskas C, Computed tomography of pneumocephalus: Am J Roentgenol, 1982; 138(1); 31-37
9. Nguyen HS, Doan N, Gelsomino M, Shabani S: Cureus, 2019; 11(3); e4260
10. Grigoriadis E, Gold WL: Clin Infect Dis, 1997; 25(5); 1108-12
11. Jim KK, Brouwer MC, van der Ende A, van de Beek D, Subdural empyema in bacterial meningitis: Neurology, 2012; 79(21); 2133-39
12. Agrawal A, Timothy J, Pandit L, Shetty L, Atraumatic intracranial pneumocephalus and pneumococcal meningitis: Neurol India, 2008; 56(3); 328-29
13. Akhaddar A, Subdural empyema: Diagnosis and management: Infections in Neurosurgery and Spinal Surgery Springer, 2017
14. Nguyen I, Urbanczyk K, Mtui E, Li S, Intracranial CNS infections: A literature review and radiology case studies: Semin Ultrasound CT MR, 2020; 41(1); 106-20
15. Saleem S, Anwar A, Aslam H, Non-traumatic pneumocephalus and sub-dural empyema as a complication of chronic sinusitis: Cureus, 2019; 11(7); e5202
16. Eça R, Graça A, Francisco R, Pamplona J, Subdural empyema as a complication of sinusitis: A diagnosis to keep in mind: Cureus, 2024; 16(1); e53249
17. Moseley IF, Kendall BE, Radiology of intracranial empyemas, with special reference to computed tomography: Neuroradiology, 1984; 26; 369-78
18. Martin A, Winn A, Sanchez A, Castellon I, MRI of emergent intracranial infections and their complications: Top Magn Reson Imaging, 2020; 29(4); 125-34
19. Aghadoost H, Salehabadi G, Fakharian E, Subdural empyema in patient with SARS-CoV-2 positivity: A rare case report of 3 patients: Radiol Case Rep, 2024; 20(3); 1552-58
20. Zimmerman RD, Leeds NE, Danziger A, Subdural empyema: CT findings: Radiology, 1984; 150(2); 447-52
21. Das JM, Munakomi S, Bajaj J, Pneumocephalus: StatPearls [Internet], 2024, National Library of Medicine https://www.ncbi.nlm.nih.gov/books/NBK441937/
22. Saposnik G, Barinagarrementeria F, Brown RDAmerican Heart Association Stroke Council and the Council on Epidemiology and Prevention, Diagnosis and management of cerebral venous thrombosis: A statement for healthcare professionals from the American Heart Association/American Stroke Association: Stroke, 2011; 42(4); 1158-92
Figures
Figure 1. Increased density in the extra-axial space is seen on initial CT brain without contrast, most commonly seen in subdural hematoma.Figure 2. Abnormal soft tissue is observed in the brain on the initial CT scan of the brain without contrast. Sulcal effacement is seen in the right posterior temporal and occipital regions.Figure 3. Pneumocephalus is visible in the extra-axial space on the initial CT scan of the brain without contrast, most often due to venous air embolus.Figure 4. EKG showed sinus tachycardia at 128 beats per minute (bpm) without ischemic changes.Figure 5. Complete opacification of the right maxillary sinus is seen on initial CT of the brain without contrast. Mucosal thickening and right sinus hypoplasia are also seen.Figure 6. CT brain after right frontal craniotomy without contrast. Interval resolution of previously present small-volume right frontal pneumocephalus. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133