05 August 2020: Articles 
Diagnostic Delays in Metastatic Amelanotic Melanoma Presenting as Breast Pain
Challenging differential diagnosis, Rare disease
Tiffanie Do1EF, Raisa Epistola1EF, Duong T. Hua1EF*, Maria M. Taylor2BC, Rose Venegas2BCDOI: 10.12659/AJCR.921360
Am J Case Rep 2020; 21:e921360






Abstract
BACKGROUND: Breast metastases from melanoma are rare. Amelanotic melanoma is difficult to diagnose, as primary lesions not only lack the pigment typical of melanoma, but also lack other features associated with these tumors, including asymmetry, irregular borders, and color variegation.
CASE REPORT: A 58-year-old woman presented with an enlarging mass on her left breast, a finding confirmed by physical examination. Mammography showed a 10-cm breast mass of category 4 according to the Breast Imaging Reporting and Data System (BI-RADS). Staging computed tomography (CT) showed widely scattered metastatic sites in the brain, lungs, mediastinum, and adrenal glands. A biopsy of the mass in her left breast was non-diagnostic due to extensive necrosis. Because of severe pain, simple left breast mastectomy was performed. Tissue from the mastectomy revealed a diagnosis of amelanotic malignant melanoma.
CONCLUSIONS: Diagnosing amelanotic melanoma is difficult without tissue biopsy as these tumors lack the typical features of melanoma and can mimic other dermatologic diseases. This frequently results in a significant delay in diagnosing amelanotic melanoma, with patients often presenting with advanced stage disease having poor prognosis.
Keywords: Breast Neoplasms, Melanoma, Melanoma, Amelanotic, delayed diagnosis, Mastectomy, Mastodynia, Skin Neoplasms
Background
Metastases to the breast of extra-mammary tumors are rare, with an incidence of 1–2% [1,2]. Tumors that more frequently spread to the breast include malignant melanomas, pulmonary carcinomas, and lymphomas [3]. Malignant melanoma is one of the most prevalent and most aggressive forms of skin cancer worldwide [4]. These tumors most frequently metastasize to the liver, lungs, and brain, although they can metastasize to any organ including the breast, which is an uncommon site [5]. It may be difficult to distinguish metastases from primary breast tumors, especially when tumors present as an isolated masses with no evidence of systemic disease. Furthermore, meta-static amelanotic melanoma (AM) from an unknown primary is rare, with an incidence of 2.2% [6,7]. The poor prognosis of patients with AM is due in part to difficulties encountered in making an early accurate diagnosis. This report describes the challenges encountered in diagnosing metastatic AM in a woman who presented with an enlarging mass on her left breast and the associated poor prognosis of this patient.
Case Report
A 58 year-old post-menopausal Hispanic woman with no significant past medical history presented to the emergency room with an enlarged left breast of 6 months’ duration, along with pain for the previous 1 month. Physical examination showed that her left breast was double the size of her right breast, along with erythema and warmth encompassing the lateral aspect. A firm, palpable, and tender 7-cm mass was observed on her left breast, accompanied by nipple retraction and dimpling, but no discharge. Ultrasound revealed a large oval mass with microlobulated margins and necrotic center occupying almost the entire left breast, with diffusely increased vascularity in the surrounding tissue. Mammography showed a 10 cm by 10 cm mass in her left breast classified as category 4 according to the Breast Imaging Reporting and Data System (BI-RADS) (Figure 1). An ultrasound-guided biopsy of the mass yielded a specimen unsatisfactory for diagnostic evaluation due to extensive necrosis. The sample was negative for all specific breast markers. Differential diagnoses included meta-static breast carcinoma, stromal component of malignant phyllodes tumor, and sarcoma not otherwise specified. Computed tomography (CT) scans of her head, chest, abdomen and pelvis revealed multiple enhancing lesions in the brain, mediastinal lymphadenopathy, pulmonary nodules with invasion into the pericardium, axillary nodules, and bilateral adrenal masses suggesting metastases (Figure 2). Although it was unclear whether this mass was a primary or secondary tumor site, its large size and associated pain prompted urgent palliative simple mastectomy of her left breast. Because the CT scans showed widespread disease, sentinel lymph node biopsy was not performed. Immunohistochemistry showed that the mass was positive for vimentin, S-100, and MiTF-1 and negative for MART, HMB-45, epithelial breast markers, and BRAF mutation, suggesting a malignant AM (Figures 3, 4). Although treatment with nivolumab and ipilumumab was planned, the patient’s functional status deteriorated. She was enrolled in a hospice and died shortly thereafter.
Discussion
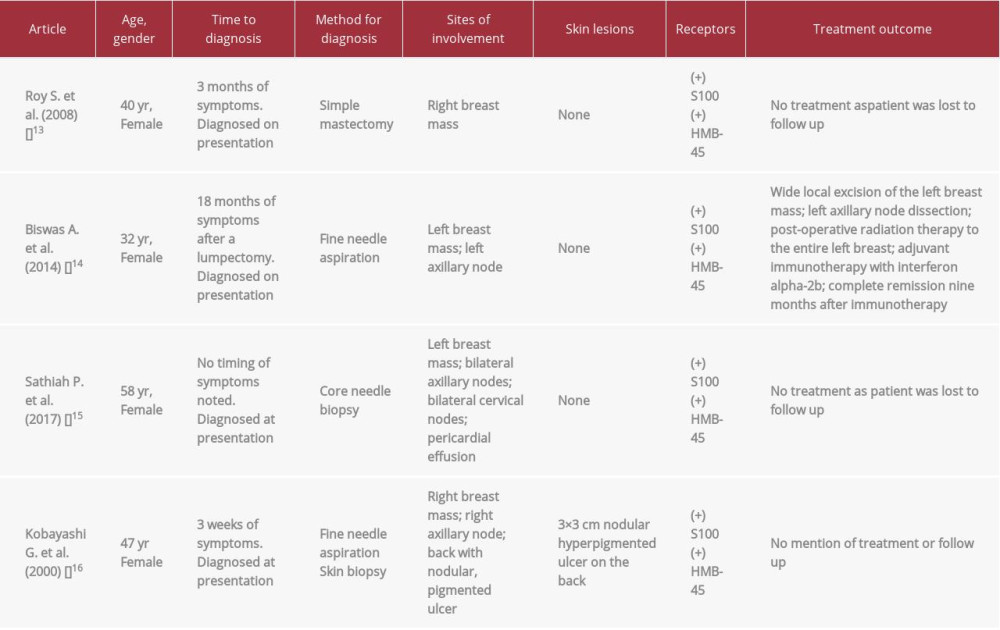
AM is an uncommon subtype of melanoma, being present in 2–8% of patients with malignant melanoma [8,9]. Diagnosing AM is challenging because the primary lesion lacks the typical pigment usually found in melanoma. Lesions may be amelanotic or hypomelanotic, which appear similar on clinical examination. These lesions can be distinguished by dermatoscopy, as discernible pigmentation is present only on hypomelanotic lesions [9]. Adding to the diagnostic challenge, AM rarely exhibits the classic features of melanomas, such as asymmetry, irregular borders, and color variegation [10]. AM lesions can have various shapes, borders, and colors, with these characteristics mimicking several other dermatologic diseases. For example, AM lesions can appear nodular or flat; have well- or poorly-defined borders; be pink-erythematous or light brown color; and have scaling or disruption of skin markings [9]. The atypical appearance of AM often results in a significant delay in diagnosis, with most patients presenting with advanced stage disease. The five year survival rates are 85% for patients with localized AM and 96% for patients with melanotic melanoma [11], compared with 26% in patients with metastatic AM [11]. It is difficult to identify a primary skin lesion in patients with metastatic AM. For example, a primary skin lesion was detected in only one of four patients with AM of the breast, (Table 1).
Because of the atypical clinical presentation of these lesions, immunohistochemistry is required to confirm diagnosis, as in our patient, and to differentiate between benign and malignant melanocytotic tumors. All four additional patients with amelanotic melanoma of the breast identified in the literature, were positive for S-100 and HMB-45 (Table 1). Although our patient was also positive for S-100, she was negative for HMB-45. Many immunohistochemical markers, including S-100, HMB-45, MART-1/Melan-A, tyrosinase, and MITF, are highly specific for melanoma, with S-100 being the most sensitive. Because the histological features of melanoma vary considerably, no single histologic marker is diagnostic [10].
This case highlights the difficulties diagnosing metastatic AM of unknown primary origin. AM in this patient was finally diagnosed by IHC staining after mastectomy rather than by staining of an ultrasound guided biopsy sample, as the latter sample was unsatisfactory. Diagnostic delay may have been reduced by obtaining a core needle biopsy sample, which is more sensitive than fine needle aspiration cytology in diagnosing primary breast cancers, although these two diagnostic methods have not been compared for melanomas of the breast [12]. Two of the four patients with metastatic AM were diagnosed by fine needle aspiration. Diagnostic inaccuracy in our patient not only delayed her diagnosis, but resulted in an unnecessary and invasive simple mastectomy in a patient with extensive metastatic disease. The findings in our patient also emphasize the importance of identifying a primary malignancy site before treatment, as management depends on the origin of the primary tumor. This patient died 56 days after her initial presentation. Of the four patients reviewed, only one received treatment, which included wide local excision, node dissection, whole breast irradiation, and adjuvant inter-feron alpha-2b, and resulted in complete remission (Table 1). Breast metastases from melanoma may indicate wide meta-static spread and poor patient prognosis, suggesting that aggressive surgical procedures may be ineffective.
Conclusions
This report describes a patient who initially presented with metastases of AM to the breast and illustrates the poor prognosis of patients with this condition. Because of difficulties diagnosing metastatic AM, a multidisciplinary team is essential for further management, which may be palliative due to the advanced stage of the tumor and poor patient prognosis at presentation.
Figures
References:
1.. Georgiannos SN, Chin J, Goode AW, Sheaff M, Secondary neoplasm of the breast: A survey of the 20th century: Cancer, 2001; 92; 2259-66
2.. Toombs BD, Kalisher L, Metastatic disease to the breast: Clinical, pathologic and radiographic features: Am J Roentgenol, 1977; 129; 673-76
3.. Williams SA, Ehlers RA, Hunt KK, Metastases to breast from non-breast solid neoplasms: Presentation and determinants of survival: Cancer, 2007; 110; 731-37
4.. McIntosh IH, Hooper AA, Millis RR, Greening WP, Metastatic carcinoma within the breast: Clin Oncol, 1976; 2; 393-401
5.. Vergier B, Trojani M, de Mascarel I, Metastases to the breast: Differential diagnosis from primary breast carcinoma: J Surg Oncol, 1991; 48; 112-16
6.. Buzaid AC, Agarwala SS, Hauschild A, Atkins M, Algorithm for the management of metastatic cutaneous melanoma: Chin Clin Oncol, 2014; 3; 32
7.. Slingluff CL, Flaherty K, Rosenberg SA, Read PW, Cutaneous melanoma: DeVita, Hellman, and Rosenberg’s cancer: Principles and practice of oncology, 2011; 1643-91, Philadelphia, PA, Lippincott Williams and Wilkens
8.. Kurul S, Taş F, Büyükbabani N, Different manifestations of malignant melanoma in the breast: A report of 12 cases and a review of the literature: Jpn J Clin Oncol, 2005; 35; 202-6
9.. Jaimes N, Braun RP, Thomas L, Marghoob AA, Clinical and dermoscopic characteristics of amelanotic melanomas that are not of the nodular sub-type: J Eur Acad Dermatol Venereol, 2012; 26; 591-96
10.. Ohsie SJ, Sarantopoulos GP, Cochran AJ, Binder SW, Immunohistochemical characteristics of melanoma: J Cutan Pathol, 2008; 35; 433-44
11.. Moreau JF, Weissfeld JL, Ferris LK, Characteristics and survival of patients with invasive amelanotic melanoma in the USA: Melanoma Res, 2013; 23; 408-13
12.. Wang M, He X, Chang Y, A sensitivity and specificity comparison of fine needle aspiration cytology and core needle biopsy in evaluation of suspicious breast lesions: A systematic review and meta-analysis: Breast, 2017; 31; 157-66
13.. Roy S, Dhingra K, Mandal S, Khurana N, Unusual presentation of metastatic amelanotic melanoma of unknown primary origin as a solitary breast lump: Melanoma Res, 2008; 18; 447-50
14.. Biswas A, Goyal S, Jain A, Primary amelanotic melanoma of the breast: Combating a rare cancer: Breast Cancer, 2014; 21; 236-40
15.. Sathiah P, Gochhait D, Adithan S, Amelanotic signet ring cell melanoma presenting as a breast lump – a diagnostic conundrum: J Clin Diagn Res, 2017; 11; ED8-10
16.. Kobayashi G, Cobb C, A case of amelanotic spine-cell melanoma presenting as metastases to breast and axillary lymph node: diagnosis by FNA cytology: Diag Cytopath, 2000; 22; 246-49
Figures
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133