08 August 2020: Articles 
Full Remission of Long-Term Premenstrual Dysphoric Disorder-Like Symptoms Following Resection of a Pituitary Adenoma: Case Report
Unusual clinical course, Unusual or unexpected effect of treatment
Guangrong Lu1ABCDEF*, Tiana M. Shiver2BDE, Spiros L. Blackburn1BDE, William C. Yao3BDE, Meenakshi B. Bhattacharjee4BDE, Jay-Jiguang Zhu1ABDEDOI: 10.12659/AJCR.922797
Am J Case Rep 2020; 21:e922797






Abstract
BACKGROUND: Few case reports exist in the literature of patients with pituitary adenoma presenting with premenstrual syndrome (PMS) or premenstrual dysphoric disorder (PMDD). Complete remission of persistent PMDD symptoms after surgical removal of a pituitary lesion has not been reported.
CASE REPORT: We report a case of a 44-year-old woman with childbearing potential who underwent transsphenoidal surgery (TSS) in December 2017 to remove a non-functioning pituitary adenoma. The surgery resulted in full remission of her PMDD symptoms. The patient’s hormone levels remained stable before and after the TSS procedure. During 28 months of follow-up, the woman has been asymptomatic for periods of 6 consecutive months or longer without taking antidepressants. Given the patient’s current condition, a durable remission from PMDD is anticipated.
CONCLUSIONS: We believe that refractory PMS/PMDD associated with pituitary lesions is under-diagnosed and under reported. As demonstrated in this case, surgical intervention for a sellar mass has the potential to be effective or even curative for patients with PMS/PMDD. We recommend that physicians consider magnetic resonance imaging of the brain in patients with PMS/PMDD.
Keywords: Magnetic Resonance Imaging, Neurosurgical Procedures, Pituitary Neoplasms, Premenstrual Syndrome, premenstrual dysphoric disorder
Background
Premenstrual dysphoric disorder (PMDD) is a severe and disabling form of premenstrual syndrome (PMS) affecting 1.2–8% (1.2–6.4% [1] and 3–8% [2]) of menstruating women. The disease appears to be ovarian hormone-related because physical and psychiatric symptoms only occur during the luteal phases in menstruating women. These symptoms do not occur in females prior to their menarche, during pregnancy, or after menopause. However, no ovarian hormone has been clinically validated as a biomarker for PMDD [3]. Based on the hypothesis that has been known since the 1980s that PMDD is associated with changing levels of gonadal steroids [1], ovariectomy or total hysterectomy with bilateral salpingo-oophorectomy has been offered to patients with refractory PMS/PMDD whose condition has failed to respond to all existing treatments [4]. However, observations of treatment efficacy from such surgical procedures were mainly empirical; their effectiveness and clinical benefits have never been validated with controlled clinical trials. Gibson et al. reported a 10-year follow-up study of patients who underwent surgical menopause including ovarian conservation (N=76) and bilateral oophorectomy (N=101) in whom depression and anxiety scores evaluated and were compared with patients experiencing natural menopause (N=1793). There was no significant clinical benefit from surgical intervention based on statistical analysis, regardless of ovarian retention [5]. Use of antidepressant medication and hormone therapy was also documented [5], indicating that symptom-free status was not commonly achieved with surgical procedures alone. A similar study has never been done among patients with PMS/PMDD who chose to have ovariectomy as intervention.
We report the case of a patient with chronic PMS/PMDD-like symptoms for more than 20 years, and who had a coexistent pituitary adenoma that was found in 2016 by brain magnetic resonance imaging (MRI). She underwent transsphenoidal surgery (TSS) in December 2017 when the tumor was found to be larger with follow-up MRIs, and had met criteria for surgical intervention (Figure 1). The goal of the surgery was to achieve accurate diagnosis and to prevent optic chiasm compression. Surprisingly, the patient experienced dramatic improvement in her PMDD-like symptoms after surgery. To our knowledge, this is the first case report of remission of PMS/PMDD-like symptoms after TSS.
Case Report
The patient, a 44-year-old woman, was first diagnosed with major depression in 1997 while she was still residing in China. Physical symptoms included delayed and irregular menstruation, bloating, and chest tightness in a cyclical pattern that had persisted for more than 20 years. She gave birth to three healthy children and did not experience such symptoms during her pregnancies, but the symptoms returned postpartum and were accompanied by severe weight loss after her third delivery (Figure 1A). These monthly recurring symptoms occurred about 5–10 days prior to the patient’s menses, and completely resolved with the onset of her period. After she was diagnosed with major depression by her psychiatrist in China, she was prescribed selective serotonin reuptake inhibitors (SSRI), but the patient did not benefit from these medications.
The patient experienced persistent intermittent psychiatric symptoms including depressed mood, anxiety, anger, self-blame, and suicidal ideation with attempts. Initially, agoraphobia and social avoidance were noted, but these symptoms resolved 5 to 6 years later. Subsequently, she developed cyclic chest tightness that worsened over the years. With the onset of symptoms, she also exhibited self-destructive behaviors, such as head-banging against walls or hitting her head with her hands intermittently. These behaviors were unassociated with headache, nausea, or vomiting. The patient developed suicidal thoughts and attempted suicide a few times around the year 2010, but did not have suicidal ideation during the 5 years prior to TSS. She denied cold or heat intolerance, thirst, or hair loss. Physical and neurological exams were within normal limits except for a highly anxious state and severely reduced self-confidence and tendency to self-blame. Thyroid function evaluated multiple times showed results within normal limits. Repeated medical check-ups showed no evidence of hypertension, cardiac ischemia, electrocardiographic abnormalities, or tachycardia, that could have contributed to the complaints of chest tightness. The patient has never used tobacco, alcohol, or illegal drugs. Her family history is positive only for maternal hyperthyroidism.
The patient was initially seen in the neuro-oncology clinic in 2016 because of galactorrhea. Laboratory results showed a prolactin (PRL) level of 35.9 ng/mL (Table 1). Brain MRI with contrast revealed a solid pituitary lesion. She was prescribed bromocriptine (2.5 mg once daily). Her PRL level rose to 50.8 ng/mL once while on bromocriptine, and subsequently returned to within the normal range (Table 1). The patient’s galactorrhea responded quickly to bromocriptine, and her monthly symptoms were also significantly improved. Typical PMDD symptoms reappeared in October 2017. A diagnosis of PMDD was made based on recurrent monthly symptoms, including sudden feelings of sadness and crying, markedly depressed mood, and markedly increased interpersonal conflicts with family members (Figure 1A).
Repeat brain MRI showed a pituitary adenoma with increased size that met the criteria for surgical intervention (Figure 1B). Visual acuity in the patient’s right eye was worse than left eye, but that had been stable over the last 10 years without optic nerve compression or peripheral vision loss. She declined to have visual acuity or visual field testing by an ophthalmologist. The patient was sent to an emergency room two weeks prior to the scheduled surgery because of sudden onset of chest tightness, but no cause was found for the symptoms, or for evidence of myocardial ischemia. Elective TSS was performed on December 28, 2017 and the pathological diagnosis was a nonfunctioning pituitary adenoma (NFPA). She tolerated the TSS well without any complication, and a gross total resection of the pituitary adenoma was achieved.
The patient has been followed for 28 months at the time of writing of this report. Her menstrual cycles became normal and regular (Table 2) after TSS and she was completely symptom-free during months 1 to 3, 8, 10, 12 to 18, and 20 to 28 without taking medication. She had sporadic episodes of chest tightness and anxiety during postoperative months 4 to 7, 9, 11 and 19. These symptoms did not have the same temporal relationship with the patient’s menses, and the symptoms were mild and short-lived. She does not drink coffee regularly, but happened to drink it a couple of times at work after she recovered from the TSS. A few hours after drinking coffee she reported mild anxiety and chest tightness, which resolved completely in 3 to 5 days. She developed two more episodes of mild anxiety and chest tightness; one was after watching a scary movie trailer in month 9, and the other episode was after one red-eye flight in month 19 post-TSS (Table 2). The patient did take vortioxetine (5 mg) samples once a day for 2 weeks during the 7th month post-TSS, but she chose to discontinue the medication. She has returned to a normal life, and has been free of PMDD symptoms for a 9-month period without medications.
Discussion
We report a case of a menstruating patient with full remission of PMDD symptoms after resection of a NFPA. This patient was first diagnosed with major depression in 1997, prior to the formal adoption of PMDD in the Diagnostic and Statistical Manual of Mental Disorders (DSM-V 2013) [1]. Her medical/psychiatric symptoms and their duration met the diagnostic criteria for PMDD. We describe her symptoms as PMDD-“like” because the diagnosis was not made by a psychiatrist, and it was a retrospective diagnosis. Based on psychiatric studies of major depressive disorders, in which a “full remission” is defined as a return of and sustained normal functioning for 4 to 6 months [6], the patient’s recovery met this definition. Most recently, she has achieved a symptom-free status for 9 months consecutively, with regular menstrual cycles. Although she has experienced recurrent episodes of mild anxiety and chest tightness associated with coffee consumption, scary movies, and a late-night flight, she recovered from these symptoms within 3 to 5 days without further medical intervention.
In this patient, a pituitary mass was identified during evaluation for galactorrhea. Her PRL level was slightly elevated (Table 1), but it did not meet the current diagnostic criteria for prolactinoma (PRL ≥250 µg/L). A stalk effect [7] rather than a true prolactin-secreting adenoma is quite possible, and pathological findings confirmed the pituitary lesion to be a NFPA. A literature search revealed similar cases. For example, one 32-year-old patient with PMS/PMDD with an initial PRL level of 48.1 µg/L was found to have a co-existing “micro-prolactinoma” (8×4 mm), which was stable in size during a 17-month follow-up [8]. Although the elevated PRL was successfully suppressed with cabergoline, the patient continued having cyclical mood fluctuations described as “2 weeks of normal mood followed by a week of depressed mood with hypersomnia, anorexia, and fatigue, and then a week of hypomanic symptoms” [8]. This is a typical description of PMS/PMDD.
Elevated intrasellar pressure (ISP) is known to occur in patients who have pituitary lesions, and it has been suggested as a cause for the clinical symptoms as the symptoms resolve after surgical reduction of ISP [9,10]. Elevated pressure on the pituitary gland, either indirectly from increased intracranial pressure, or directly from cerebrospinal fluid leaking into the pituitary fossa, is a known cause for the empty sella syndrome (ESS). Contrary to the common belief that ESS is usually asymptomatic, two early studies of 43 [11] and 71 [12] cases reported a high frequency of psychological disorders [11] and 80.2% [12] of mental disorders, respectively. A literature search exploring the occurrence of psychiatric symptoms that may predate the objective pituitary findings, depression was reported in 71% of relevant papers [13]. On average, it took 11 years from initially documented clinical depression to an objective pituitary abnormality among 51% of cases with pituitary findings [13].
Encouragingly, studies of psychiatric symptoms associated with NFPA are now getting some needed attention [14]. For example, one study demonstrated that patients with NFPA (N=58) have increased anxiety-related personality traits compared to 140 age- and gender-matched, mentally healthy population controls [15]. A NFPA has been noted in a PMDD patient [8], and in a woman with major depression [16]. Complete remission of major depression was also reported after surgical removal of the lesion [16].
Stalk effect from pituitary gland may be a dynamic phenomenon. It is not necessarily absent in patients with normoprolactinemia [7]. Based on such observations, surgery may be a better treatment option than pharmaceutical agents because surgical removal of a lesion will eliminate the stalk effect [8] and/or elevated ISP [9,10]. Surgical removal of NFPA and drainage of cysts have been demonstrated to provide durable normalization of serum PRL levels and to achieve significant symptom reduction or resolution [7,14]. Unfortunately, no study has ever been conducted regarding the long-term effects of pituitary gland surgery on psychiatric/psychological outcomes.
The exact pathophysiology of and factors contributory to PMS/PMDD remain elusive. For example, studies on an association between coffee consumption and PMS are inconclusive [17,18]. Interestingly, the patient in this case had two episodes of anxiety and/or chest tightness soon after coffee consumption, and similar episodes after a red-eye domestic flight. Because she suffered PMDD for more than 20 years, her reaction threshold to such stimuli may be lower than normal. It is also possible that chemicals such as caffeine, or a change in fear-related internal neurotransmitter(s) trigger a neural cascade, which leads to different psychiatric symptoms.
Based on what we observed in this case, we propose a model in which pituitary hormone secretion is not thought to be the key factor causing PMS/PMDD symptoms (Figure 2). Rather, we speculate that some neurotransmitters indirectly affected by either the stalk effect or elevated ISP may have causative roles. This patient’s symptoms can still be triggered by coffee and other stimuli (scary movies) after months free of symptoms, which indicates that an etiopathogenetic neurotransmitter cascade still gets activated when the inciting stimulus presents. The pituitary gland receives neurotransmitters from the hypothalamus, and in young women, its size changes during each menstrual cycle [19,20]. If there is a space-occupying pituitary adenoma within the sella turcica, physiological change in size or length of a normal pituitary gland during each menstrual cycle will be restricted. Given the impact of a space-occupying lesion, a distorted hypophyseal gland body or stalk reduces or blocks transmission of neurotransmitter(s) coming down from the hypothalamus or other anatomic connections. Imbalanced neurotransmitter(s) subsequently result in PMS/PMDD symptoms. When the pituitary gland’s size returns to its baseline during the follicular phase, a patient’s PMS/PMDD symptoms are reduced or resolved as long as the sella can still hold both pituitary gland and a small space-occupying mass. With this model, clinical benefits might reasonably be expected after surgical removal of mass lesion. However, the model would not explain the absence of PMS/PMDD during pregnancy despite the fact that the pituitary gland enlarges throughout pregnancy as a physiological process [21,22].
Evidence is lacking at this time on the benefits of surgical treatment of NFPA in patients with psychiatric disorders. As a result, we cannot draw any firm conclusions; however, this case report along with prior evidence of psychiatric disease in patients with NFPA supports a possible link. Therefore, we recommend that physicians use brain MRI to assess for possible pituitary lesions in patients with refractory PMS/PMDD. For patients with PMS/PMDD who have a comorbid pituitary lesion, surgery should be considered, with postoperative monitoring and evaluation of PMS/PMDD symptoms. Identification of additional cases like the one presented here may facilitate classification of PMS/PMDD with comorbid pituitary lesion as a subtype of PMS/PMDD.
Conclusions
Surgical resection of NFPA resulted in immediate relief and durable remission of PMDD symptoms as demonstrated in this case. This observation suggests that a NFPA or another space-occupying lesion in the sella, either due to stalk effect or elevated ISP, may play a contributory role in PMDD. A brain MRI scan with and without contrast should be considered in screening patients with refractory PMS/PMDD. Prospective studies should investigate whether a pituitary lesion may cause or indirectly contribute to PMS/PMDD and surgical intervention might be of benefit in these patients.
Figures
References:
1.. Yonkers KA, Simoni MK, Premenstrual disorders: Am J Obstet Gynecol, 2018; 218(1); 68-74
2.. Rapkin AJ, Lewis EI, Treatment of premenstrual dysphoric disorder: Womens Health (Lond), 2013; 9(6); 537-56
3.. Rubinow DR, Hoban MC, Grover GN, Changes in plasma hormones across the menstrual cycle in patients with menstrually related mood disorder and in control subjects: Am J Obstet Gynecol, 1988; 158(1); 5-11
4.. Casson P, Hahn PM, Van Vugt DA, Reid RL, Lasting response to ovariectomy in severe intractable premenstrual syndrome: Am J Obstet Gynecol, 1990; 162(1); 99-105
5.. Gibson CJ, Joffe H, Bromberger JT, Mood symptoms after natural meno-pause and hysterectomy with and without bilateral oophorectomy among women in midlife: Obstet Gynecol, 2012; 119(5); 935-41
6.. Kennedy S, Full remission: A return to normal functioning: J Psychiatry Neurosci, 2002; 27(4); 233-34
7.. Bergsneider M, Mirsadraei L, Yong WH, The pituitary stalk effect: Is it a passing phenomenon?: J Neurooncol, 2014; 117(3); 477-84
8.. Burback L, Management of a microprolactinoma with aripiprazole in a woman with cabergoline-induced mania: Endocrinol Diabetes Metab Case Rep, 2015; 2015; 150100
9.. Arafah BM, Prunty D, Ybarra J, The dominant role of increased intrasellar pressure in the pathogenesis of hypopituitarism, hyperprolactinemia, and headaches in patients with pituitary adenomas: J Clin Endocrinol Metab, 2000; 85(5); 1789-93
10.. Hayashi Y, Sasagawa Y, Oishi M, Contribution of intrasellar pressure elevation to headache manifestation in pituitary adenoma evaluated with intraoperative pressure measurement: Neurosurgery, 2019; 84(3); 599-606
11.. Bragagni G, Bianconcini G, Mazzali F, 43 cases of primary empty sella syndrome: A case series: Ann Ital Med Int, 1995; 10(2); 138-42
12.. Bianconcini G, Bragagni G, Bianconcini M, Primary empty sella syndrome. observations on 71 cases: Recenti Prog Med, 1999; 90(2); 73-80
13.. Cardoso F, Azizi H, Kilpatrick A, Chronic atypical depression as an early feature of pituitary adenoma: A case report and literature review: Case Rep Psychiatry, 2019; 2019; 4892183
14.. Zaidi HA, Cote DJ, Castlen JP, Time course of resolution of hyperprolactinemia after transsphenoidal surgery among patients presenting with pituitary stalk compression: World Neurosurg, 2017; 97; 2-7
15.. Sievers C, Ising M, Pfister H, Personality in patients with pituitary adenomas is characterized by increased anxiety-related traits: Comparison of 70 acromegalic patients with patients with non-functioning pituitary adenomas and age- and gender-matched controls: Eur J Endocrinol, 2009; 160(3); 367-73
16.. Chang H-A, Chang C-C, Chen C-L, Ma H-I, Mood disorder due to nonfunctioning pituitary adenoma with a major depressive-like episode in a post-menopausal woman: Journal of Medical Sciences, 2007; 27(1); 41-46
17.. İşik H, Ergöl Ş, Aynioğlu Ö, Premenstrual syndrome and life quality in Turkish health science students: Turk J Med Sci, 2016; 46(3); 695-701
18.. Purdue-Smithe AC, Manson JE, Hankinson SE, A prospective study of caffeine and coffee intake and premenstrual syndrome: Am J Clin Nutr, 2016; 104(2); 499-507
19.. Tsunoda A, Okuda O, Sato K, MR height of the pituitary gland as a function of age and sex: Especially physiological hypertrophy in adolescence and in climacterium: Am J Neuroradiol, 1997; 18(3); 551-54
20.. Grams AE, Gempt J, Stahl A, Förschler A, Female pituitary size in relation to age and hormonal factors: Neuroendocrinology, 2010; 92(2); 128-32
21.. Dinç H, Esen F, Demirci A, Pituitary dimensions and volume measurements in pregnancy and post partum. MR assessment: Acta Radiol, 1998; 39(1); 64-69
22.. Elster AD, Sanders TG, Vines FS, Chen MY, Size and shape of the pituitary gland during pregnancy and post partum: Measurement with MR imaging: Radiology, 1991; 181(2); 531-35
Figures
Tables
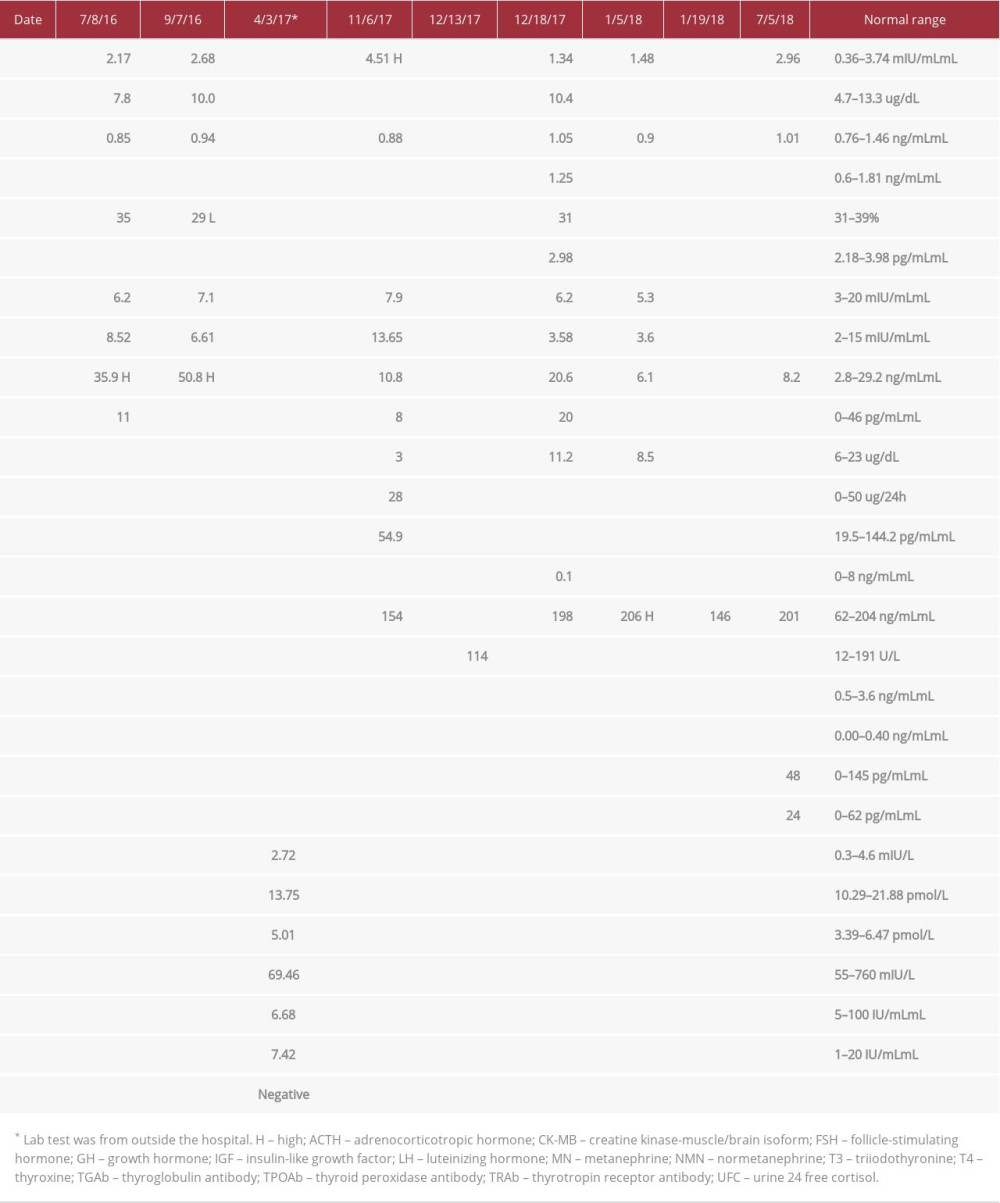 Table 1.. Relevant lab results prior to and post-pituitary adenoma diagnosis and TSS.
Table 1.. Relevant lab results prior to and post-pituitary adenoma diagnosis and TSS.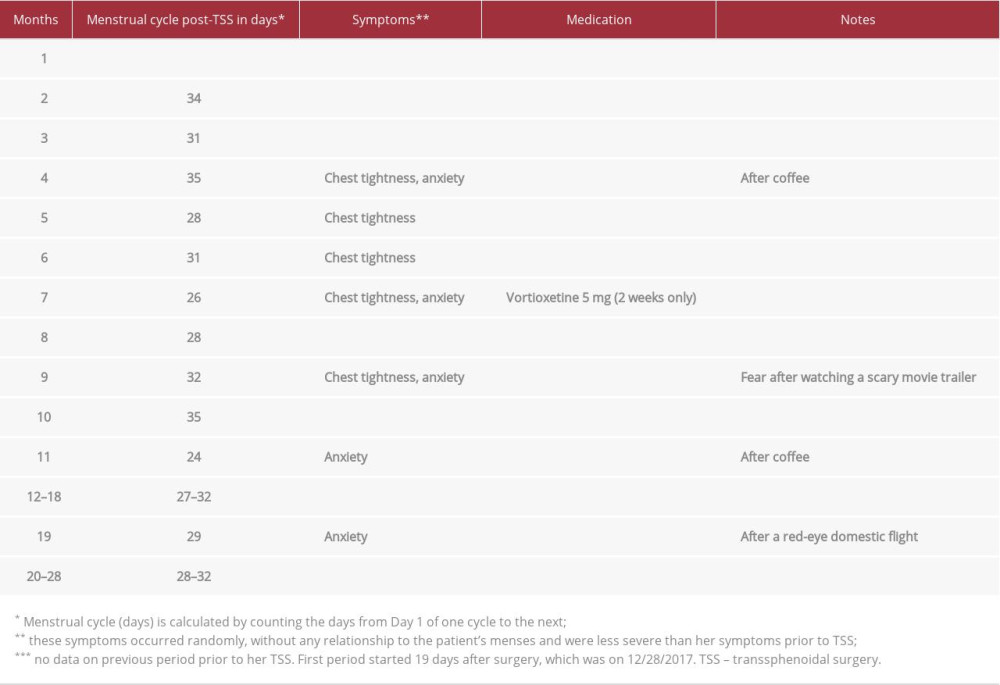 Table 2.. Summary of symptoms during the 28 months follow up post-TSS.Table 1.. Relevant lab results prior to and post-pituitary adenoma diagnosis and TSS.Table 2.. Summary of symptoms during the 28 months follow up post-TSS.
Table 2.. Summary of symptoms during the 28 months follow up post-TSS.Table 1.. Relevant lab results prior to and post-pituitary adenoma diagnosis and TSS.Table 2.. Summary of symptoms during the 28 months follow up post-TSS. In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133