26 November 2020: Articles 
A Case Report of Malignant Eccrine Porocarcinoma Involving the Palm Requiring Surgical Excision and Free Flap Reconstruction
Challenging differential diagnosis, Unusual or unexpected effect of treatment, Rare coexistence of disease or pathology
Kevin L. Chow1ABCDEF, Xane Peters1CDEF, Hassan Mashbari2ABCDEF*, Mohammad Shokouh-Amiri1CDEF, Martin Benjamin1ABCDEF, Michael Warso1ACDEDOI: 10.12659/AJCR.925231
Am J Case Rep 2020; 21:e925231






Abstract
BACKGROUND: Eccrine porocarcinoma (EPC) was first described in 1963 as an epidermotropic eccrine carcinoma. Fifty years later, its etiology remains poorly understood. The infrequent nature of this disease merits further inquiry into its etiology, presentation, and standards of management. Furthermore, the propensity for metastasis, which may be as high as 31% on presentation, increases the importance of investigating this rare disease.
CASE REPORT: The patient was a 63-year-old mechanic who presented with the lesion as a chronic wound following a chemical exposure. The lesion involved the ulnar aspect of his right palm and had concern for extension to the underlying tendons. He underwent a wide excision extending from the wrist to the proximal interphalangeal joint, preserving the ulnar neurovascular bundle. The hand was reconstructed with an anterolateral thigh fascia perforator flap and a skin graft. He had an excellent functional and cosmetic recovery. Unfortunately, he developed metastases to the lymph nodes, necessitating an axillary lymphadenectomy followed by adjuvant chemoradiation using concurrent cisplatin and docetaxel with radiation for 6 weeks. Follow-up at 18 months found no recurrence.
CONCLUSIONS: Cases of EPC presenting in the fingers have been managed with amputation of the involved phalanges; however, in addition to obtaining complete excision with negative margins, surgeons who deal with tumors of the hand must also consider the goals of limb preservation, functional preservation, and functional reconstruction. Options for reconstruction following excision include primary closure, dermal regeneration templates, skin grafts, flaps, and free-tissue transfer, depending on what tissue types are needed.
Keywords: chemoradiotherapy, Eccrine Porocarcinoma, Free Tissue Flaps, Lymph Node Excision, Reconstructive Surgical Procedures, Sweat Gland Neoplasms
Background
Eccrine porocarcinoma (EPC) was first described in 1963 by Pinkus and Mehregan as an epidermotropic eccrine carcinoma [1]. Fifty years later, its etiology remains poorly understood. Possible predisposing factors include immunosuppression, exposure to pesticides or benzenes, and lifelong sunlight exposure without adequate protection. The infrequent nature of this disease merits further inquiry into its etiology, presentation, and standards of management. Furthermore, the propensity for metastasis, which may be as high as 31% on presentation, increases the importance of investigating this rare disease [2]. We present a case of EPC on the palmar aspect of the hand, treated with wide local excision (WLE) and reconstruction using an anterolateral thigh fascia perforator flap. Regrettably, the patient was later found to have metastases to the axilla treated with an axillary lymph node dissection and adjuvant chemoradiation. To the best of our knowledge, this is only the fourth reported case of eccrine porocarcinoma with the primary lesion on the palm [3,4].
Case Report
A 63-year-old male mechanic presented for surgical evaluation of a tumor growing from his right palm. He initially noticed the lesion, 1 year prior to our evaluation, after he sustained a puncture wound and was exposed to an unknown chemical. The lesion began as a chronic wound on his hand, which was biopsied at an outside hospital, demonstrating an eccrine tumor. This tumor progressively enlarged over the course of 1 year, becoming more painful and inhibiting the use of his hand, which then led to his referral. He had a previous history of diabetes, hypertension, and hyperlipidemia, without any previous surgeries. On examination, there was a 5×6 cm round lesion on the ulnar aspect of the right palm with a fungating center measuring 2.5×2.5 cm (Figure 1). The motor functions of the ulnar, anterior, and posterior interosseous nerve (AIN, PIN) were intact. Sensory functions of the median, ulnar, and radial nerves were intact. Flexion in all digits of the hand were present, although weak. There was also an intention tremor at baseline. An MRI of the hand demonstrated a soft-tissue tumor of the palm of the right hand on the ulnar side involving the skin and extending into the subcutaneous tissue, with stranding and abnormal areas of signal extending to the underlying tendons (Figure 2).
We planned for a combined operation with Surgical Oncology for a WLE with 1–2 cm margins and Plastic Surgery for wound closure. There was concern that he did not have a patent superficial palmar arch, precluding a distally-based forearm flap. Instead, he would need a free-tissue transfer using a vascularized fascial flap and skin graft such as an anterolateral thigh (ALT) fascia perforator flap. We discussed the possibility of lymph node evaluation; however, as it was unclear if sentinel lymph node biopsy or other interventions would affect outcomes, we decided to follow the nodes clinically after discussions with the patient.
The excision was approximately 9×17 cm extending from the wrist to the PIP joint of the hand and was carried down through the superficial and subcutaneous tissues of the hand. The tumor was seen to be extending deep into the tissues of the hand; therefore, the palmar fascia and the intrinsic structures of the hand were dissected free. The ulnar neurovascular bundle was dissected out, preserving both the vessels and nerves as the specimen was removed off the underlying lumbrical muscles and tendons, leaving them intact (Figure 3). An ALT fascia perforator flap was harvested from the right thigh with inflow from a large perforator from the transverse branch of the lateral circumflex artery (Figure 4). A microsurgical anastomosis was performed from the lateral circumflex system to the radial artery, and the venous anastomosis was performed with a 2.0-mm coupler. A fenestrated split-thickness skin graft was also harvested from the patient’s right thigh and applied to the palmar defect.
Microscopically, the lesion had an epidermal component consisting of nests and islands of small basaloid cells, sharply demarcated from the adjacent keratinocytes. The tumor cells proliferated with irregular broad anastomosing cords into the dermis. Cytologic and nuclear atypia, mitosis, and necrosis were also present (Figure 5A–5D). Final pathology was a poorly differentiated porocarcinoma with intraepithelial involvement, including eccrine duct involvement, invasion of the subcutaneous tissue, perineural invasion, and extension to the inked deep margin. Immunohistochemical staining was also performed and is summarized in Table 1, comparing it to typical melanomas, basal cell carcinomas, and squamous cell carcinomas.
Postoperatively, the patient had an excellent functional recovery with full use of his hand and was cosmetically acceptable, although he did have some paresthesia of his 3rd and 4th digit. Unfortunately, 5 months after his initial resection, he developed right axillary lymphadenopathy that was hypermetabolic on positron emission tomography (PET), necessitating an axillary lymphadenectomy with 10/15 nodes positive for malignancy. Based on a case report by Mandaliya et al., adjuvant chemoradiation was pursued with concurrent cisplatin, docetaxel, and radiation therapy (50 Gy/25 fractions) for 6 weeks [5]. He has had no recurrence during the follow-up period of 18 months.
Discussion
Eccrine porocarcinoma is a rare malignant cutaneous neoplasm that presents as an ambiguous and difficult-to-diagnose entity. There is no consensus regarding optimal work-up and management due to the scarcity of data, which are limited to case reports and case series. EPC often presents as a plaque, a slow-growing painless nodule, a cyst, or as a chronic ulcer. They are commonly misidentified as squamous cell carcinoma (SCC), SCC
High-risk histologic features, including increased tumor depth (>7 mm), lymphovascular invasion, higher number of mitoses (>14 mitoses per 10 high-power fields), and poorly differentiated tumors, suggest the need for further diagnostic imaging to evaluate for metastasis [6]. Metastatic disease to the regional lymph node basins on presentation is common and has been reported in 22% to 31% of cases [2,4]. As such, ultra-sound, PET/CT, or MRI of regional lymph node basins should be considered for all EPC tumors found on the trunk, extremities, and genitalia, and can assist with surgical planning [4]. When palpable lymphadenopathy is present or when there are suspicious imaging findings, fine-needle aspiration (FNA) can be performed to confirm lymph node involvement.
The mainstay of treatment is surgical excision of the primary tumor and involved lymph nodes. The most common treatment for the primary EPC without metastasis is WLE with 3-mm margins; however, there is a trend towards utilizing Mohs micrographic surgery (MMS) [4,6]. In one of the largest case series, by Tolkachjov et al., MMS was utilized in 9 cases of EPC without lymph node involvement and had no recurrence or metastatic disease during their follow-up period [6]. Although no large-scale studies have been performed to compare WLE to MMS, they are comparable in the literature and, when local expertise is available, MMS can be beneficial in cosmetically challenging areas [6]. A sentinel lymph node biopsy (SLNB) can also be performed in tumors with high-risk features, and lymph node dissections can be performed for involved basins; however, disease-free or survival benefits have not been demonstrated [4]. In cases where a SLNB was performed, 81.3% were reported positive for metastasis [4]. For those with nodal involvement, the use of chemotherapy or radiotherapy is more varied and is controversial, while those with distant metastatic disease were predominantly treated with chemotherapy. The most frequently reported chemotherapy regimens are 5-fluorouracil, cisplatin, doxorubicin, vincristine, and mitomycin [5].
Conclusions
Amongst EPC, primary tumors of the hand are especially rare, representing as little as 3% of all EPC cases reported in the literature and can differ based on the region of the hand involved [7]. Cases of EPC presenting in the fingers have been managed with amputation of the involved phalanges; however, Wong et al. demonstrated success in more conservative excisions, with no recurrence or signs of metastasis [8]. Only 1 other case of EPC on the palm has been reported in the literature [3,4]. In addition to obtaining complete excision with negative margins, surgeons who deal with tumors of the hand must also consider the goals of limb preservation, functional preservation, and functional reconstruction. Options for reconstruction following excision include primary closure, dermal regeneration templates, skin grafts, flaps, and free-tissue transfer, depending on what tissue types are needed [9].
To the best of our knowledge, this is the only reported case of EPC on the palmar aspect of the hand treated with simultaneous wide local excision, preserving the underlying tendons to maintain functionality, and to utilize a free-tissue transfer reconstruction with an ALT fascia perforator flap, achieving an acceptable cosmetic and functional outcome. The patient subsequently developed lymph node metastases and underwent a lymph node dissection with adjuvant chemoradiation using concurrent cisplatin, docetaxel, and radiation therapy (50 Gy/25 fractions) for 6 weeks, with no recurrence during the follow-up period of 18 months.
Figures
Tables
Table 1.. Tumor markers.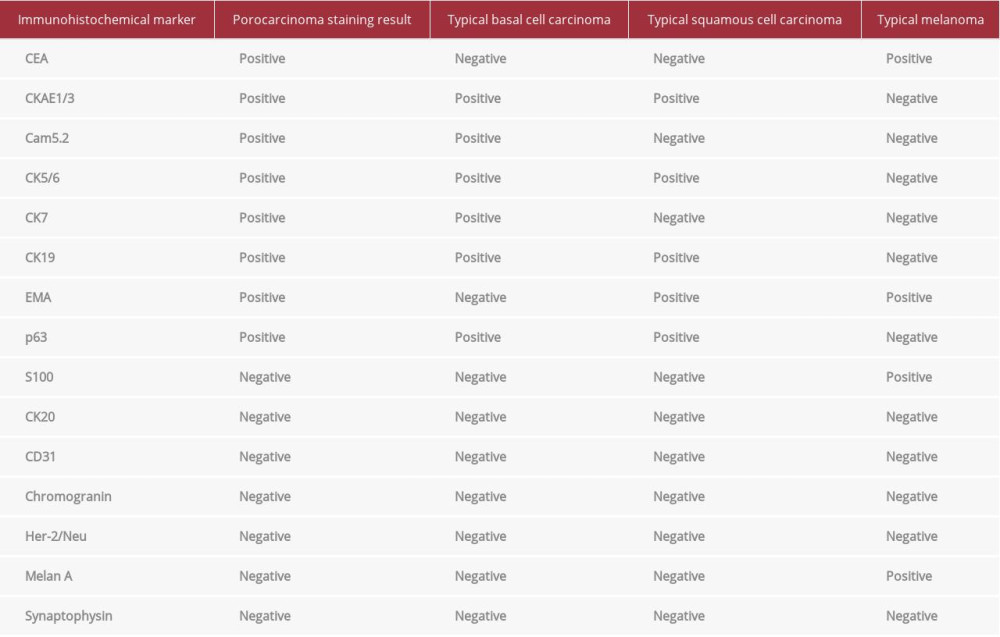
References:
1.. Pinkus H, Mehragan AH, Epidermotropic eccrine carcinoma: A case combining features of eccrine poroma and paget’s dermatosis: Arch Dermatol, 1963; 88(5); 597-606
2.. Salih AM, Kakamad FH, Baba HO, Porocarcinoma; Presentation and management, a meta-analysis of 453 cases: Ann Med Surg, 2017; 20; 74-79
3.. Shaw M, Mckee PH, Lowe D, Black MM, Malignant eccrine poroma: A study of twenty-seven cases: Br J Dermatol, 1982; 107(6); 675-80
4.. Nazemi A, Higgins S, Swift R, Eccrine porocarcinoma new insights and a systematic review of the literature: Dermatol Surg, 2018; 44(10); 1247-61
5.. Mandaliya H, Nordman I, Metastatic eccrine porocarcinoma: A rare case of successful treatment: Case Rep Oncol, 2016; 9(2); 454-56
6.. Tolkachjov SN, Hocker TL, Camilleri MJ, Baum CL, Treatment of porocarcinoma with mohs micrographic surgery: Dermatologic Surg, 2016; 42(6); 745-50
7.. Robson A, Path MRC, Greene J, Eccrine porocarcinoma (malignant eccrine poroma): A clinicopathologic study of 69 cases: Am J Surg Pathol, 2001; 25(6); 710-20
8.. Wong A, Hughes C, Luu X, Subungal malignant eccrine porocarcinoma: An unusual presentation: Eur J Plast Surg, 2013; 36(2); 131-33
9.. Yegiyants SS, Avashia YJ, Panthaki ZJ, Reconstruction of the hand: Dermatologic surgery: Step by step, 2013; 177-82, Blackwell
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133