24 February 2021: Articles 
Complicated Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome History in a 14-Year-Old
Unknown etiology, Challenging differential diagnosis, Diagnostic / therapeutic accidents, Unexpected drug reaction
Michael Tomani1ADEF*, Cristina Caridi1ABEF, Oksana Tatarina-Nulman1ABEF, Cascya Charlot1ADEF, Pramod Narula1ADEFDOI: 10.12659/AJCR.927951
Am J Case Rep 2021; 22:e927951






Abstract
BACKGROUND: Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome is a drug-induced hypersensitivity reaction that can result in a severe cutaneous adverse drug reaction (SCAR). It is a rare and potentially life-threatening condition that occurs after exposure to sulfonamides, antibiotics, or antiepileptics. Its incidence in children is not established; however, the mortality rate is documented at approximately 10%. DRESS syndrome is believed to result from an interaction between multiple factors, including genetics, abnormalities of metabolism, and reactivation of certain herpes family viruses including EBV and HHV-6. The classic presentation includes fever, rash, and lymphadenopathy. Symptoms begin approximately 3 to 8 weeks after exposure to the offending agent.
CASE REPORT: We present a unique case of DRESS syndrome in a 14-year-old girl occurring after the ingestion of minocycline and amoxicillin-clavulanic acid (amoxicillin). Identification of the offending agent was complicated by the patient having been on multiple antibiotics within a short timeframe of the initial presentation of symptoms. In addition to swelling and pruritus, the patient experienced vision problems due to papilledema with bilateral hemorrhage. The treatment course was further complicated by a decrease in kidney function, requiring the patient’s medication regimen to be adjusted accordingly.
CONCLUSIONS: This is a unique case of DRESS syndrome demonstrating the potential influence of certain viruses on the severity of its presentation. This case also highlights the need to adjust the steroid regimen to reduce the potentially harmful effects on various organ systems.
Keywords: Drug Hypersensitivity, Drug Hypersensitivity Syndrome, Eosinophilia, Adolescent, Anti-Bacterial Agents, Anticonvulsants, Child, Exanthema
Background
Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome is classified as a drug-induced hypersensitivity reaction, as well as a severe cutaneous adverse drug reaction (SCAR). It is a rare and potentially life-threatening condition that occurs primarily after exposure to antibiotics, particularly sulfonamides, or antiepileptics [1,2]. Its incidence in children is not established; however, its mortality rate is documented at approximately 10% [3]. DRESS syndrome is believed to result from an interaction between multiple factors, including genetics, abnormalities of metabolism, and reactivation of certain herpes family viruses, including human herpes virus (HHV)-6, HHV-7, cytomegalovirus (CMV), and Epstein-Barr virus (EBV) [4].
The classic presentation of DRESS syndrome includes fever, rash, and lymphadenopathy. Symptoms begin approximately 3 to 8 weeks after exposure to the offending agent. Facial edema, which is considered as the hallmark feature of the disease, is present in approximately 76% of cases [5]. Typically, the liver and kidney are affected, but other organs potentially involved are the pancreas, thyroid, heart, brain, muscle, peripheral nerves, and eye [6].
In this case report, we present a unique case of DRESS syndrome occurring after the ingestion of amoxicillin and minocycline. This report highlights the need for proper detail-oriented history taking, necessity of close follow-up, with special attention to the monitoring of renal function, and adaptations in the scheduling of steroid tapering.
Case Report
The patient is a 14-year-old Black girl in generally good health, who presented with a sore throat and a diffuse pruritic rash over her entire body, which started 6 days prior to presentation. The history that was gathered from the Emergency Department (ED) visit was complex and required extensive questioning to understand the sequence of events that may have led to her symptoms. The patient presented to our ED with rash and swelling of the face and arms (Figure 1). Prior to presentation to our ED, the patient had sought care at multiple urgent care clinics and EDs. Approximately 14 to 30 days prior to arrival, the patient was prescribed minocycline by a dermatologist. The exact date the medication was started is unknown and was unable to be confirmed. Approximately 2 weeks later, the patient went to a water park, after which she experienced symptoms of suspected ear infection. The patient self-medicated with an old bottle of amoxicillin for about 1 week, with inconsistent frequency. Nonetheless, the symptoms persisted. She visited an urgent care clinic and was prescribed amoxicillin for a suspected sinus infection. A rash occurred after the first prescribed dose of amoxicillin. Due to the nonspecific reported timeline of the patient’s initial incomplete course of amoxicillin, the patient’s timeline (Day 1) begins at presentation, the day she took her first dose of prescribed amoxicillin and the rash initially developed. The patient went on to complete 3 total doses of amoxicillin at this time (Table 1).
The rash was described as erythematous, with fine papules all over her body. The face and arms were more affected than the rest of the body. The rash was reported to have developed cranio-caudally. The patient’s eyelids then became swollen bilaterally, with generalized face swelling. The patient stopped taking amoxicillin after the third dose, but the rash progressed, and significant itching developed.
Six days later (Day 7), the patient sought care at an ED because of persistent itching. She was discharged home with diphenhydramine. The pruritic rash persisted, and throat swelling developed. Since her symptoms did not improve, the patient returned to the ED the next day (Day 8). She noted an increase in a diffuse erythematous papular rash all over her body. Furthermore, the patient reported minor visual changes, which she described as blurry vision and some dizziness.
At this time the patient was given steroids (Decadron, PO, reported as standard dosing) and epinephrine IM, and was admitted for overnight observation. Her laboratory test results showed alanine aminotransferase (ALT) of 70 units/L and aspartate aminotransferase (AST) of 62 units/L (upper limit normal, 55 and 40 units/L, respectively). She was discharged the next day (Day 9) with diphenhydramine and prednisone 20 mg PO to take twice per day (bid). The patient followed this regimen for 3 days without an improvement in the swelling, rash, and itchiness.
At this time (Day 12), the patient presented to our institution’s ED with a pruritic, erythematous rash, and was noted to have periorbital edema. On physical examination, all body systems were otherwise normal. Initial laboratory results were significant for the complete blood count showing leukocytosis (an elevated white blood cell [WBC] count) of 38.5 k/μl, and a manual differential with an eosinophil count of 18%. The patient received IV fluids, diphenhydramine, and methylprednisolone 40 mg IV every 12 h. She was admitted for further monitoring.
Treatment with hydroxyzine was started on Day 13. This regimen of medications continued for 3 days, and the patient was discharged home on Day 16. During the hospitalization, repeat testing of eosinophils on a manual differential were noted to be 15%. The patient was provided instructions to taper the dose of steroids at home. The day following discharge (Day 17), the patient reported a fever of 39.1°C and an episode of non-bloody, non-bilious vomiting. She went to her primary doctor the next day (Day 18) complaining of a sore throat, fever, cough, and blurry vision. Although her visual symptoms had improved initially, the patient experienced a worsening in visual acuity and mild associated dizziness. She was prescribed azithromycin and albuterol. Laboratory results were significant for an elevated WBC of 35 k/μL.
Two days after seeing her primary doctor (Day 20, 4 days after discharge from our hospital) the patient returned to our ED with a fever of 38.7°C, dizziness, submental and submandibular lymphadenopathy, and generalized maculopapular rash of the arms, legs, torso, and back. She received a stress dose of 1 g of methylprednisolone and was admitted to the hospital.
Magnetic resonance imaging (MRI) of the brain and electrocardiogram results were unremarkable. Ultrasound imaging showed hepatomegaly. The patient’s liver function test (LFT) results were significantly elevated, with ALT 1080 units/L and AST 1836 units/L. The renal function test results showed a BUN level of 15 mg/dL and a creatinine level of 2.22 mg/dL. Thus, the patient was admitted to the Pediatric Intensive Care Unit. Upon admission, the patient’s laboratory test results were significant for leukocytosis (WBC 32.1 K/uL) and prominent eosinophilia (eosinophils 18%) on the manual differential, which was consistent with DRESS syndrome. The EBV titers were measured at IgM <36 U/mL and IgG 526 U/100 mL; the IgM titer was within normal limits at this time. The patient received IV methylprednisolone 1 g every 24 h for 3 days (finishing on Day 23). During this time, the patient’s LFTs and creatinine levels were noted to be significantly elevated, but they later normalized after the 3 days of IV steroid administration (Table 1).
The patient clinically improved, and was discharged from the hospital (Day 24) with oral prednisone 25 mg bid after a 4-day admission. The patient’s prednisone dosage was increased to 30 mg bid the next day (Day 25) because of ongoing symptoms. Throughout the following week, her laboratory values were monitored closely on an outpatient basis, with specific attention paid to her renal function. The patient’s creatinine level was noted to increase from 1.28 mg/dL to 1.61 mg/dL (Table 1), which prompted a multiple-day course of outpatient IV steroid infusion treatment. The patient received a daily dose of IV solumedrol for 4 days (Day 33 to Day 36). Similar to the results from her previous IV steroid treatment, there was dramatic improvement in her creatinine, with levels that decreased from 1.61 mg/dL to 1.33 mg/dL, and then to 0.86 mg/dL, with restarting of oral prednisone treatment of 30 mg bid (Table 1).
One week later (Day 43), the patient returned with complaints of significant blurry vision. At an outpatient ophthalmology clinic, she was found to have papilledema with bilateral hemorrhage. The patient went to the ED and was readmitted to the hospital, approximately 1 month after her initial admission.
The 2 competing diagnoses at this time were pseudotumor cerebri, secondary to high-dose steroids, and ongoing DRESS syndrome. The patient’s MRI scan was unremarkable. The EBV titers were repeated and showed IgM >100 mg/dL, which was significant and added to the complicated nature of this case, as it indicates a possible reactivation of EBV, as compared with the previous levels of IgM of 36 U/mL. The patient underwent a lumbar puncture with an increased opening pressure of 40 cm H20. The results from all other studies were unremarkable. The patient was treated with acetazolamide, which led to an improvement of symptoms, and the patient was discharged after 4 days.
The patient’s dosage of oral prednisone was decreased to 20 mg bid, and while her creatinine had a brief increase to 1.19 mg/dL, it consistently decreased afterward (Figures 2–4). The ongoing concern of autoimmunity was continually followed up and only nonspecific antinuclear antibodies (ANA) were found to be elevated, with a 1: 1086 titer. All other titers and values were noted to be negative, indicating no significant concern of an additional developing autoimmunity.
The patient was transferred to the affiliated academic medical center. Consultations with the Departments of Neurology, Ophthalmology, Nephrology, Rheumatology, and Dermatology confirmed the DRESS diagnosis. The rheumatology specialist repeated all titers, including histone AB, and only ANA was elevated, once again. The patient continued on prednisone 20 mg bid for fluctuating renal function indicators. On a repeat ophthalmology examination, papilledema was still present but was noted to have continually improved after the patient began treatment with acetazolamide. No other visual field deficits were noted at the time. The patient’s renal function continued to steadily improve. Finally, the patient was discharged after a 10-day admission at the affiliated academic medical center (Day 54). The ophthalmologist agreed that the patient should continue taking prednisone, with slow tapering.
Although the protocol [7] recommended decreasing the prednisone dosage by 5 mg per week and checking weekly laboratory examination results, it was decided to maintain a total daily dosage of 40 mg, owing to the repeat elevation in the patient’s creatinine values. Two days after discharge (Day 56) the patient’s creatinine level was 0.98 mg/dL, indicating a significant improvement in her renal function. The patient was administered mycophenolic acid for 3 days (completed on Day 59). The administration of cyclosporine and cyclophosphamide was considered, but was refused by the patient due to concerns of the effects on her kidneys and fertility. The patient’s rash significantly improved after 2 months of treatment. The patient is still being followed by various specialists including, but not limited to, rheumatologists, neurologists, and nephrologists, and she continues to show clinical improvement.
The diagnosis of DRESS syndrome was considered early in the patient’s initial hospital course; however, due to an inaccurate reported history regarding the supposed timing of antibiotic consumption, it was not considered to be the main differential diagnosis. Upon further questioning during the worsening of symptoms, the patient remembered consuming medication 21 days prior to her initial presentation for a suspected ear infection. It was discovered that the medication was amoxicillin. To complicate matters further, the patient’s mother recalled that she was also prescribed minocycline by a dermatologist weeks before the initial symptoms began. This information greatly helped our team formulate a more effective treatment plan. A visual representation of the entire timeline is shown in Table 1.
Discussion
We present a unique case of DRESS syndrome for which we propose further emphasis on the monitoring of renal function throughout the course of the patient’s illness. For the most part, DRESS syndrome has been studied in the acute phase, with particular attention paid to the monitoring of LFTs [8].
It is uncertain which drug caused the drug reaction and DRESS syndrome in this particular case. The unknown timing and duration of the minocycline prevents us from ruling out that this is the culprit drug responsible for our patient’s symptoms, as hepatotoxicity, nephrotoxicity, eosinophilia, and DRESS have all been reported as adverse effects of minocycline [9]. It is also possible that amoxicillin led to the DRESS syndrome, perhaps in part due to the short timeframe of repeated doses [10]. We emphasize the necessity for proper history taking and discussion to show that the proper diagnosis may not have been achieved were it not for the realization of the potential reaction-causing drugs.
The current literature consistently states that DRESS syndrome is typically caused by antiepileptic medications [11], but practitioners should be aware of a severe reaction after the administration of antibiotics. This case emphasizes that causative agents of DRESS syndrome can also be antibiotic therapy, and not necessarily long-term antibiotic therapy. It was confirmed by our team of specialists that the patient in this case met all the necessary criteria to confirm the diagnosis of DRESS syndrome, as she met both DRESS/DIHS30 and DRESS RegiSCAR criteria for diagnosis [12] (Tables 2, 3).
An additional point of interest in our case is the patient’s age and demographic. Although the patient was of age to be prescribed minocycline, this was her first exposure to this medication. Mori et al showed that Blacks are most likely to develop DRESS syndrome after the initiation of aromatic anticonvulsants drugs, whereas Han Chinese are most likely to develop DRESS after allopurinol intake [3]. Our patient was an adolescent Black female who developed DRESS syndrome after antibiotic therapy, illustrating that further study is necessary to show the possible genetic predisposition to specific adverse drug effects.
A few viruses have been shown to be involved in drug hyper-sensitivity reactions and DRESS syndrome. The typical viruses include EBV and HHV6 [13]. In our patient’s case, HHV6 testing was unable to be conducted due to multiple samples of an insufficient quantity, but she was shown to have high EBV titers on multiple occasions. Remarkably, the patient had a reactivation of EBV; the patient’s EBV titer from her initial admission showed IgM 36 U/mL and IgG 496 U/mL, with a subsequent increase and a positive EBV IgM 50.8 U/mL and IgG 750.00 U/ mL 1 month later. These results are unusual because both EBV IgM and IgG levels were low initially and later increased; however, this has been shown in previous literature [4] and displays the importance of testing EBV (and HHV-6) titers on patients with suspected or confirmed DRESS syndrome.
Multiple case reports and medical journals state that the long-term prognosis and risk of mortality is mostly associated with LFTs [8]. The peculiar aspect of this case is that her clinical symptoms consistently coincided with her renal function. As her creatinine levels decreased and renal function improved after various steroid treatments, her clinical symptoms concurrently improved. This could indicate that renal function, specifically creatinine levels, could serve as a marker for severity of illness in DRESS syndrome. The administration of IV steroids had the most pronounced effect, resulting in the significant improvement of our patient’s LFTs, renal function, and clinical manifestations. The use of steroids as a treatment for DRESS syndrome needs to be specifically investigated to help establish a proper protocol. Using creatinine as a marker for ongoing steroid therapy is introduced as a novel concept in this case study. This can also potentially help to direct the dose adjustments and timing of the steroid taper. Of note, no further immunomodulatory therapy was used, as the patient’s symptoms continued to improve. Intravenous immunoglobulin (IVIG) was considered early on but was not given because the patient showed a response to steroids. The use of IVIG is considered anecdotal in nature, and a few studies show that not only is not very beneficial, but that it may in fact be associated with severe adverse effects [14].
Conclusions
There are numerous causes of DRESS syndrome, such as the reaction to specific medication, viral interference, and genetic predisposition. These range from a sole reaction to a particular medication to reaction to a combination of medications and the reactivation of certain viruses [5,13]. There is evidence of genetic predisposition and lack of metabolizing enzymes for these drugs, which cannot be ruled out in the present case [5]. DRESS diagnosis is further complicated because its symptoms overlap with many autoimmune diseases [15,16]. This specific case was complicated by the patient possibly having a reaction to either minocycline or amoxicillin [9,10]. The reaction could have also been due to repeat/prolonged exposure to amoxicillin [9]. Given the patient’s ethnicity, it is possible the reaction was caused by minocycline, which is common in those of Caribbean descent [9,17]. The present case is unique, as this is a rare presentation in a patient of this age and race/ethnicity [18]. The young age of the patient also lends an opportunity to potentially add to the knowledge of long-term effects of DRESS syndrome [3]. Due to the complexity of DRESS syndrome’s etiology and diagnosis, the utmost caution is needed with short-term and long-term management and the monitoring of a patient’s care. Outlining the most effective immediate treatment must include monitoring of both the liver and kidney functions to reduce potential adverse effects on the renal and hepatic systems. Long-term follow-up is needed to monitor for early development of any potentially related comorbidities, such as autoimmune disease.
Additional therapies, such as IVIG, require further research to better understand their utility in the treatment of DRESS syndrome.
Figures
Tables
Table 1.. Patient timeline.The timeline displays the patient’s course starting from initial ingestion of the potential DRESS syndrome-inducing medications and subsequent reactions leading to the patient’s symptoms, laboratory values, and steroid treatment regimen are documented to show the patient’s course of illness and dosing of medications with subsequent steroid tapering. Table 2.. Registry of Severe Cutaneous Adverse Reaction (RegiSCAR) criteria.
Table 2.. Registry of Severe Cutaneous Adverse Reaction (RegiSCAR) criteria.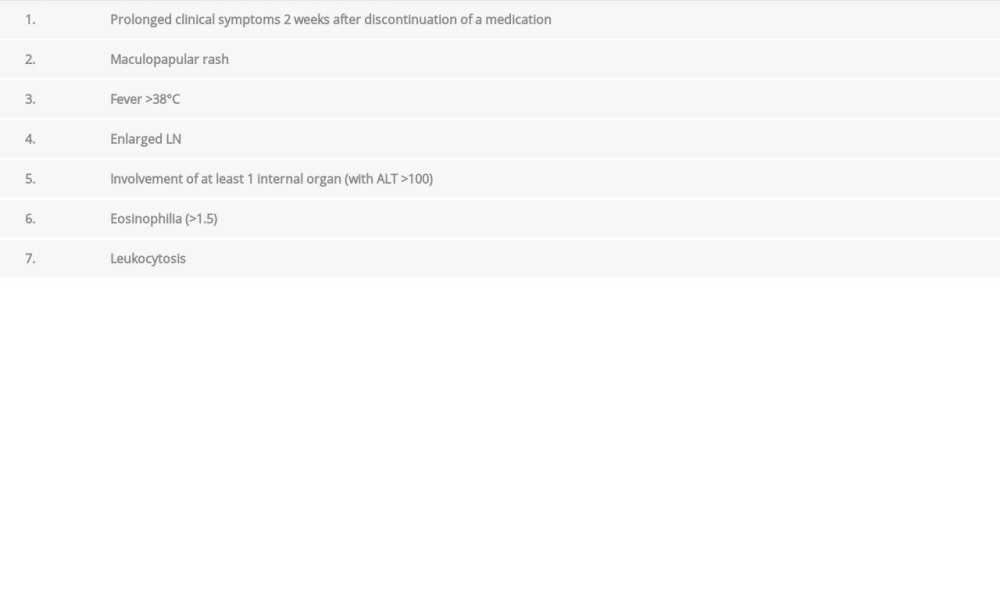 Table 3.. Drug-induced hypersensitivity syndrome (DIHS)30 criteria.
Table 3.. Drug-induced hypersensitivity syndrome (DIHS)30 criteria.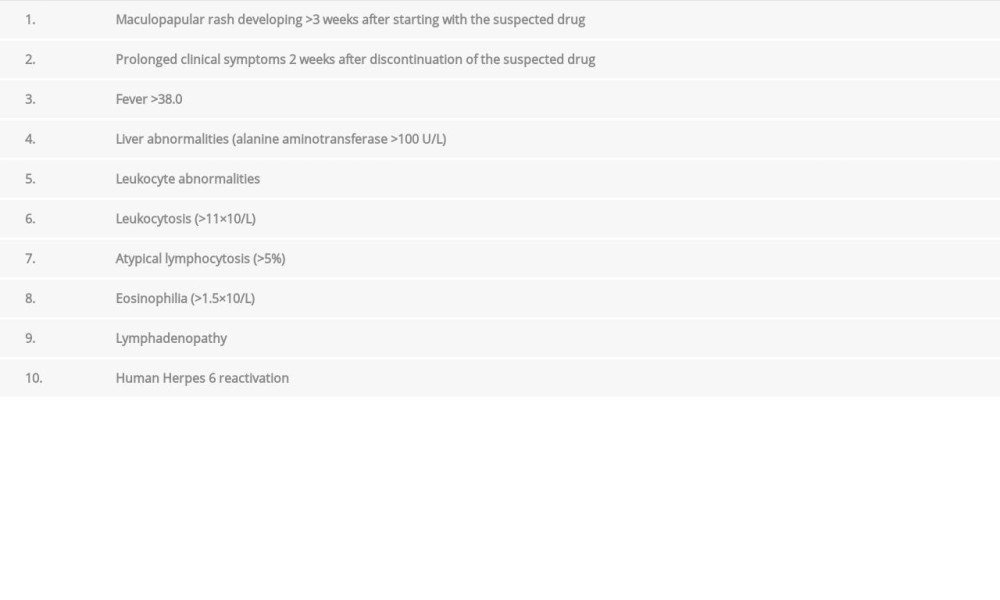
References:
1.. James J, Sammour YM, Virata AR, Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome secondary to furosemide: Case report and review of literature: Am J Case Rep, 2018; 19; 163-70
2.. Bocquet H, Bagot M, Roujeau JC, Drug-induced pseudolymphoma and drug hypersensitivity syndrome (Drug Rash with Eosinophilia and Systemic Symptoms: DRESS): Semin Cutan Med Surg, 1996; 15(4); 250-57
3.. Mori F, Caffarelli C, Caimmi S, Drug reaction with eosinophilia and systemic symptoms (DRESS) in children: Acta Biomed, 2019; 90(3-S); 66-79
4.. Lee JY, Lee SY, Hahm JE, Clinical features of drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: A study of 25 patients in Korea: Int J Dermatol, 2017; 56(9); 944-51
5.. Cho YT, Yang CW, Chu CY, Drug reaction with eosinophilia and systemic symptoms (DRESS):An interplay among drugs, viruses, and immune system: Int J Mol Sci, 2017; 18(6); 1243
6.. Kardaun SH, Sekula P, Valeyrie-Allanore L, Drug reaction with eosinophilia and systemic symptoms (DRESS):An original multisystem adverse drug reaction. Results from the prospective RegiSCAR study: Br J Dermatol, 2013; 169; 1071-80
7.. Liu D, Ahmet A, Ward L, A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy: Allergy Asthma Clin Immunol, 2013; 9(1); 30
8.. Husain Z, Reddy BY, Schwartz RA, DRESS syndrome: Part I. Clinical perspectives: J Am Acad Dermatol, 2013; 68(5); 693.e1-e14
9.. Brown RJ, Rother KI, Artman H, Minocycline-induced drug hypersensitivity syndrome followed by multiple autoimmune sequelae: Arch Dermatol, 2009; 145(1); 63-66
10.. Abdin AY, Auker-Howlett D, Landes J, Reviewing the mechanistic evidence assessors e-synthesis and EBM: A case study of amoxicillin and drug reaction with eosinophilia and systemic symptoms (DRESS): Curr Pharm Des, 2019; 25(16); 1866-80
11.. Besli GE, Yildirim S, Yilmaz K, Yuksel E, DRESS syndrome or hematologic malignancy?: Pediatr Emerg Care, 2017; 33(7); 494-96
12.. Choudhary S, McLeod M, Torchia D, Romanelli P, Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: J Clin Aesthet Dermatol, 2013; 6(6); 31-37
13.. Descamps V, Human herpesvirus 6 involvement in paediatric drug hyper-sensitivity syndrome: Br J Dermatol, 2015; 172; 858-59
14.. Joly P, Janela B, Tetart F, Poor benefit/risk balance of intravenous immunoglobulins in DRESS: Arch Dermatol, 2012; 148(4); 543-44
15.. Gowani F, Gehrs B, Scordino T, Drug-induced hypersensitivity syndrome: A clinical, radiologic, and histologic mimic of lymphoma: Case Rep Hematol, 2018; 2018; 7037352
16.. Misirlioglu ED, Guvenir H, Bahceci S, Severe cutaneous adverse drug reactions in pediatric patients: A multicenter study: J Allergy Clin Immunol Pract, 2017; 5(3); 757-63
17.. Wu PA, Anadkat MJ, Fever, eosinophilia, and death: A case of minocycline hypersensitivity: Cutis, 2014; 93(2); 107-10
18.. Hübner ST, Bertoli R, Rätz Bravo AE, C-reactive protein and procalcitonin in case reports of drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: Int Arch Allergy Immunol, 2018; 176; 44-54
Figures
Tables
Table 1.. Patient timeline.The timeline displays the patient’s course starting from initial ingestion of the potential DRESS syndrome-inducing medications and subsequent reactions leading to the patient’s symptoms, laboratory values, and steroid treatment regimen are documented to show the patient’s course of illness and dosing of medications with subsequent steroid tapering.Table 2.. Registry of Severe Cutaneous Adverse Reaction (RegiSCAR) criteria.Table 3.. Drug-induced hypersensitivity syndrome (DIHS)30 criteria.Table 1.. Patient timeline.The timeline displays the patient’s course starting from initial ingestion of the potential DRESS syndrome-inducing medications and subsequent reactions leading to the patient’s symptoms, laboratory values, and steroid treatment regimen are documented to show the patient’s course of illness and dosing of medications with subsequent steroid tapering.Table 2.. Registry of Severe Cutaneous Adverse Reaction (RegiSCAR) criteria.Table 3.. Drug-induced hypersensitivity syndrome (DIHS)30 criteria. In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133