30 January 2021: Articles 
Closure of a Prosthetic Mitral Valve Paravalvular Leak Using a Ventricular Septal Defect (VSD) Amplatzer Occluder Device
Unusual clinical course, Diagnostic / therapeutic accidents, Unusual setting of medical care
Oreoluwa Oladiran1ABCDEF*, Gabriel Areoye2ACDEF, Adeolu O. Oladunjoye3ACDEF, Olubunmi O. Oladunjoye2ACDEF, Eric Elgin1ABCDE, Anthony Licata1ABCDEFDOI: 10.12659/AJCR.928003
Am J Case Rep 2021; 22:e928003






Abstract
BACKGROUND: Paravalvular leaks (PVL) are becoming more commonly experienced in clinical practice due to the increasing number of mitral valve replacements performed. There are about 182 000 valve replacements performed annually, with a 5–15% prevalence rate of paravalvular leaks. Due to increased mortality associated with surgical repair, percutaneous transcatheter closure procedures are increasingly being performed as an alternative to repeat surgery.
CASE REPORT: We present the case of a 52-year-old woman with past medical history of mitral valve endocarditis who developed worsening acute heart failure 1 month after surgical bioprosthetic mitral valve replacement. Transesophageal echocardiography at the time revealed dehiscence of the bioprosthetic mitral valve and severe mitral regurgitation. She subsequently had emergent surgical bioprosthetic mitral valve replacement and annular reconstruction. The post-operative course was complicated by increasing dyspnea and lower-extremity edema, with recurrent pericardial tamponade requiring placement of a pericardial window. Based on her multiple comorbidities, most notably the concomitant right ventricular failure with severe pulmonary hypertension and prior pericardial patch repair with compromise of her mitral valve annulus, she was deemed inoperable for re-do surgery and eventually underwent a successful percutaneous closure of the mitral paravalvular leak with a ventricular septal defect (VSD) Amplatzer occluder device. The patient made good recovery and was discharged home a few days after the procedure.
CONCLUSIONS: Although use of the Amplatzer VSD occluder device for this indication currently remains off-label, our report supports the use of the VSD occluder device in this subset of patients considering the high mortality rates associated with repeat surgical procedure.
Keywords: cardiac catheterization, Heart Valve Diseases, Mitral Valve, Septal Occluder Device, Echocardiography, Transesophageal, Heart Septal Defects, Ventricular, Heart Valve Prosthesis, Heart Valve Prosthesis Implantation
Background
Paravalvular leaks (PVL) are becoming more commonly experienced in clinical practice due to the increasing number of mitral valve replacements performed. There are about 182 000 valve replacements performed annually, with a 5–15% prevalence rate of paravalvular leaks [1]. About 1–5% of paravalvular leaks result in serious clinical consequences ranging from hemolytic anemia to congestive heart failure [2]. Due to increased mortality associated with surgical repair, percutaneous transcatheter closure procedures are increasingly being performed as an alternative to repeat surgery. We present the case of a 52-year-old woman who had a prosthetic mitral valve PVL successfully closed with a Ventricular septal defect (VSD) Amplatzer occluder device via an antegrade transseptal approach.
Case Report
PERCUTANEOUS TECHNIQUE:
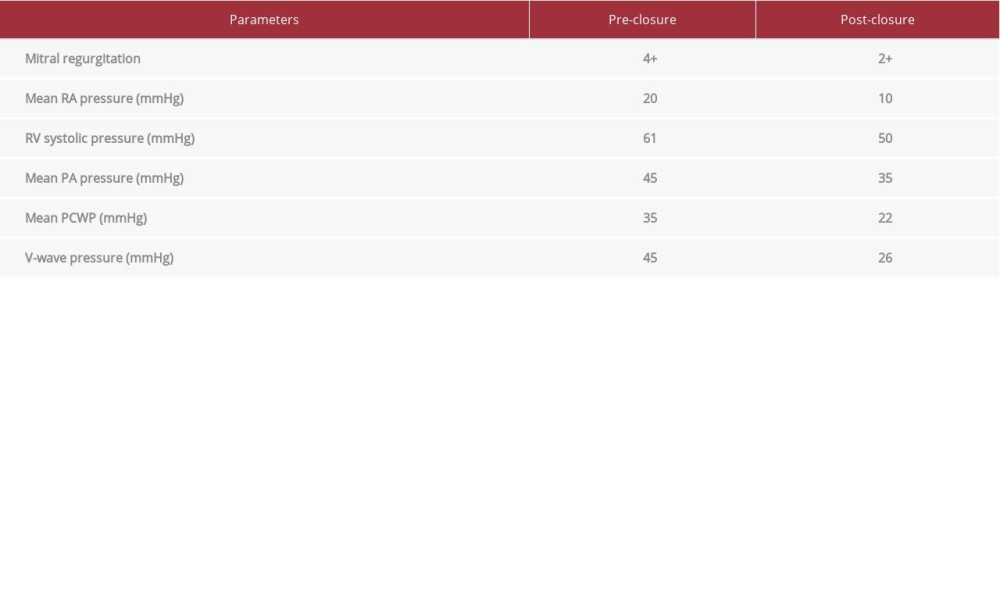
The patient was placed under general anesthesia and surgical right internal jugular line for monitoring and medication administration. The TEE probe was inserted, and initial images were obtained. Right heart catheterization was then completed in the standard fashion. A transseptal puncture was also performed and a Baylis wire was inserted into the left atrium. After confirmation of left atrial pressure and waveform, the Baylis sheath was removed and an Agilis sheath was advanced into the left atrium. The dilator was removed, a multipurpose guiding catheter was then advanced through the Agilis and with TEE guidance, and a Glidewire was directed through the defect in the left ventricle. The guidewire was removed and an Amplatz extra-stiff wire was inserted. The guide was then removed and a 14-mm VSD occluder was advanced. The ventricular disc was deployed and withdrawn to sit within the perivalvular space (Figure 3). This demonstrated immediate reduction of 4+ mitral regurgitation to 2+ mitral regurgitation with significant improvement in hemodynamics (Table 1). TEE evaluation demonstrated that tissue capture around all rims was present and the device was subsequently released. The patient made good recovery and was discharged home a few days after the procedure. At follow-up, she reported no relapse of drug abuse.
Discussion
PVL results from inappropriate sealing between the structure of the implanted valve and the surrounding cardiac tissue, resulting in blood flow via the channel [3]. It occurs in about 5–15% of patients following prosthetic mitral valve replacement, with higher incidence following surgically implanted valves compared to percutaneously implanted ones, with the majority being crescent, oval, or round mitral PVLs [3]. Although rare, about 3% of these patients progress to heart failure, hemolytic anemia, or both, requiring prompt intervention [4]. As in our case, most patients present with signs of acute mitral regurgitation and heart failure. Our patient presented with acute mitral regurgitation resulting in congestive heart failure. The criterion standard for diagnosis is echocardiography, preferably transesophageal. Transthoracic echocardiography is not as sensitive and can underestimate the severity of the regurgitation due to the eccentricity of the mitral regurgitation jet, artifacts from the bioprosthesis, and technically challenging imaging. TEE also has more utility with increasing use of real-time 3D echocardiography to evaluate the bioprosthetic valve dysfunction and help guide the repair. Surgery has long been the criterion standard intervention strategy for repair of PVL, especially for patients with infectious endocarditis, concurrent need for bypass, or an unstable prosthesis [5,6]. However, percutaneous PVL repair has been gradually becoming more commonly used over the past decade, with large-volume centers creating tailored multidisciplinary teams and employing uniform approaches, significantly improving patient selection and timing to achieve optimal results [4]. A case series by Hernandez-Enriquez et al. suggests that even though there are similar results between percutaneous and surgical PVL closure in some series, PVL is a valid alternative to surgical correction because it is well tolerated [7]. Percutaneous valve closure is less invasive, permits multiple attempts, and is an option in patients who are at high risk for open heart surgery [8,9]. Another similar case report, by Abueletta et al., advocates that percutaneous PVL closure with VSD can be done at least 3 months after the prior surgery [10]. However, we believe it is best not to wait that long after surgery, and suggest prompt intervention because of worse clinical outcomes. Our patient’s case was reviewed by the heart valve team and, due to the worsening clinical condition, a decision was made to pursue percutaneous closure using the VSD occluder. Results for percutaneous PVL closure have been promising, with low complication rates, depending on the expertise of the interventionalist. As with any other type of surgical procedure, there is still an increased risk of endocarditis, even after the procedure, especially in patients with a history of drug abuse, like this patient. Percutaneous paravalvular leak repair has been shown to improve heart failure symptoms and to decrease hospitalizations and procedure-related adverse events [11,12]. More importantly, an advantage over surgery is the improved short and midterm survival rates in patients with no PVL to mild residual leak after the procedure [4].
Conclusions
Although the use of the Amplatzer VSD occluder device for this indication currently remains off-label, this article is in support of percutaneous closure devices in mitral PVL, even as the trend toward percutaneous cardiac interventions continues to increase.
Figures
References:
1.. Sorajja P, Mitral paravalvular leak closure: Interv Cardiol Clin, 2015; 5(1); 45-54
2.. Cruz-Gonzalez I, Rama-Merchan JC, Rodríguez-Collado J, Transcatheter closure of paravalvular leaks: State of the art: Neth Heart J, 2017; 25(2); 116-24
3.. Smolka G, Wojakowski W, Paravalvular leak-important complication after implantation of prosthetic valve: E-journal of Cardiology Practice, 2010; 9(8)
4.. Alkhouli M, Zack CJ, Sarraf M, Successful percutaneous mitral paravalvular leak closure is associated with improved midterm survival: Circ Cardiovasc Interv, 2017; 10(12); e005730
5.. Trehan V, Subhendu M, Chaturvedi V, Paravalvular leak closure with two large size devices: Indian Heart J, 2014; 66(1); 91-94
6.. Spargias K, Tzifa A, Chrissoheris M, Transapical closure of mitral prosthetic paravalvular leak: Hellenic J Cardiol, 2013; 54; 397-400
7.. Hernández-Enríquez M, Freixa X, Quintana E, Paravalvular leak correction: Searching for a balance between surgical and percutaneous techniques: Rev Esp Cardiol (Eng Ed), 2018; 71(8); 679-81
8.. Asami M, Pilgrim T, Windecker S, Praz F, Case report of simultaneous trans-catheter mitral valve-in-valve implantation and percutaneous closure of two paravalvular leaks: Eur Heart J Case Rep, 2019; 3(3); ytz123
9.. Thourani VH, Smith CM, Guyton RA, Repair of prosthetic mitral valve paravalvular leak using an off-pump transapical approach: Ann Thorac Surg, 2012; 94(1); 275-78
10.. Abuelatta R, Naeim HA, Percutaneous paravalvular leak closure early post-MV replacement with retrieval of embolized muscular VSD device: JACC: Case Reports, 2019; 1(4); 471-76
11.. Ruiz CE, Jelnin V, Kronzon I, Clinical outcomes in patients undergoing percutaneous closure of periprosthetic paravalvular leaks: J Am Coll Cardiol, 2011; 58(21); 2210-17
12.. Calvert PA, Northridge DB, Malik IS, Percutaneous device closure of paravalvular leak: Combined experience from the United Kingdom and Ireland: Circulation, 2016; 134(13); 934-44
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133