10 January 2021: Articles 
A Rare Case of Acute Pleuropericarditis as a Complication of Permanent Pacemaker Insertion
Unusual clinical course, Challenging differential diagnosis, Unusual or unexpected effect of treatment, Diagnostic / therapeutic accidents
Małgorzata Chlabicz12ABCDEFG*, Piotr Jakim1BCD, Małgorzata Zalewska-Adamiec1ACDEF, Magdalena Róg-Makal1ACDEF, Sławomir Dobrzycki1ABDEFDOI: 10.12659/AJCR.928188
Am J Case Rep 2021; 22:e928188






Abstract
BACKGROUND: Pleuropericarditis after pacemaker (IPG) implantation is a rare post-cardiac injury syndrome (PCIS) condition. Pericarditis is one of the complications following insertion of a IPG; it affects 2–5% of patients within 5–21 days after IPG implementation and is associated with screw-in (active fixation) atrial lead positioning. Usually, pericarditis following IPG implantation is benign and has a self-limiting course. The mechanism of this complication remains unclear. It could involve a direct irritation of pericardium by minimally protruding electrodes, low bleeding, and autoimmune and inflammatory responses. The frequency of pleuropericarditis is not well defined. The etiopathogenesis is presumed to be the same as for pericarditis, yet there are no standardized criteria for the diagnosis, and treatment is based on the empirical anti-inflammatory therapy used in pericarditis.
CASE REPORT: A 71-year-old woman was admitted due to syncope. Sinus arrests with escape atrioventricular rhythm were observed during hospitalization; therefore, a dual-chamber pacemaker (IPG) was implanted with 2 active fixation (screw-in) electrodes. On the first day after implantation, a slight pericardial hemorrhage occurred with resorption in the following days, and an inflammatory reaction with pericardial and left pleural effusion occurred later. The first-line treatment was ineffective. However, prednisolone with colchicines with longer use than suggested by pericarditis recommendations was effective.
CONCLUSIONS: Patients with even mild pericardial effusion after IPG insertion should be followed closely due to the risk of pleuropericarditis, with consideration of anti-inflammatory treatment for longer than in pericarditis.
Keywords: case reports, Pacemaker, Artificial, Pericardial Effusion, Pericarditis, Pericardium, Pleural Effusion
Background
The mechanism of post-cardiac injury syndrome (PCIS) was suggested to be an autoimmune-mediated condition involving the pleura and pericardium. PCIS may result in pericardial effusion or pleural effusion, and may even lead to cardiac tamponade. It is a common complication after cardiac surgery. Pleuropericarditis after pacemaker (IPG) implantation is a rare condition [1]. Pericarditis is one of the complications following insertion of the IPG; it affects 2–5% of patients within 5–21 days after IPG implantation and is associated with screw-in (active fixation) atrial lead positioning [2–5]. Typically, pericarditis following the IPG implantation is benign and has a self-limiting course [3,4]. The mechanism of this complication remains unclear. It could involve a direct irritation of the pericardium by minimally protruding electrodes, low bleeding, or autoimmune and inflammatory responses [2,3,6]. Several authors reported that PCIS could occur after percutaneous coronary angioplasty, radiofrequency ablation, and IPG implantation. The frequency of pleuropericarditis is still not well defined, and the etiopathogenesis is presumed to be the same as in pericarditis. There are no standardized criteria for the diagnosis, and treatment is based on the empirical anti-inflammatory therapy used in pericarditis [1,7].
Case Report
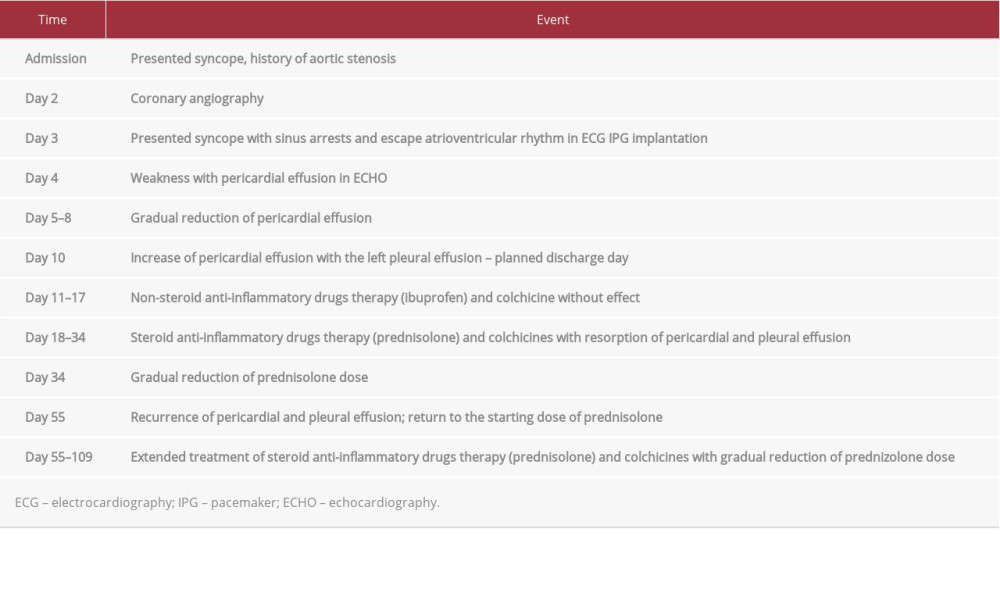
A 71-year-old woman with a medical history of aortic stenosis was admitted to the Invasive Cardiology Department due to syncope. The timeline illustrating subsequent events is shown in Table 1. The patient had no history of smoking or alcohol or drug abuse. Echocardiography (ECHO) revealed right atrial dilatation, left ventricular wall hypertrophy, severe aortic stenosis (aortic valve area 0.7 cm2), moderate mitral and tricuspid regurgitation, left ventricular ejection fraction of 70%, and no pericardial fluid. The levels of highly sensitive C-reactive protein (hs-CRP) (9.0 mg/L) and fibrinogen (351 mg/dL) were in the normal ranges (hs-CRP 0–10.0 mg/L; fibrinogen 200–400 mg/dL). The patient was qualified for transcatheter aortic valve implantation (TAVI); therefore, a coronary angiography was performed, which showed no atherosclerotic changes in the coronary arteries. During hospitalization, symptomatic sinus arrests with escape atrioventricular rhythm were observed; hence the first dual-chamber pacemaker (IPG) was implanted with 2 active-fixation (screw-in) electrodes. One day after implantation, the patient reported weakness. The electrocardiography (ECG) presented diffused PQ segment depression and ST segment elevation (Figure 1). The chest X-ray showed correct electrode placement and no lung changes. The ECHO examination revealed pericardial effusion (1 cm) and normal cardiac function. The IPG follow-up revealed correct leads parameters. The patient was stable; therefore, no action was taken. In the following days, no complaints were reported and the amount of fluid in the pericardial sac decreased, but 5 days later (planned discharge day), the fluid increased up to 11 mm behind the posterior wall of the left ventricle with effusion in the left pleura up to 48 mm (Figure 2A, Video 1). In ECHO, atrial and ventricular electrodes were correctly located (Figure 2B). The IPG follow-up reveled correct and stable leads parameters. The computed tomography (CT) scan of the chest did not show any signs of perforation of electrodes, but there was 23 mm of fluid (the addition of blood could not have been excluded, and 30 Hounsfield units [HU] suggested exudate) behind the posterior wall of the left ventricle and up to 60 mm of effusion in the left pleural cavity (Figure 2C, Video 2). There was a small amount of fluid in front of the right ventricle; hence, pericardiocentesis was not performed (Video 3). Nevertheless, the left pleural cavity was punctured, and 300 ml of dark yellow fluid was obtained. The analysis demonstrated serosanguineous exudate (pleural fluid/serum protein ratio 0.68; pleural fluid/serum lactate dehydrogenase [LDH] ratio 1.2, and pleural fluid LDH >2/3 upper limit of normal plasma levels) and negative bacterial culture. The patient had not had a fever since the admission. The laboratory tests revealed normal white blood cell count (4.96×103/ul) and procalcitonin (PCT) level (0.1 ng/ ml), yet high level of highly sensitive C-reactive protein (hs-CRP) (168.3 mg/L) and fibrinogen (711 mg/dL). Based on the aforementioned factors, we diagnosed pleuropericarditis following the IPG insertion. Initially, colchicine (0.5 mg per 24h) and ibuprofen (1.2 g per 24 h) [1, 5] were administered, without any effect (the increase of pericardial effusion to 25 mm and pleural effusion to 62 mm) (Figure 2D). Then, predniso-lone (0.5 mg/kg per 24 h) with colchicine (0.5 mg per 24 h) [1] were introduced, which resulted in a gradual reduction of pericardial fluid and decrease of hs-CRP value. The patient did not receive any antibiotics. On the 23rd day of hospitalization, the patient was discharged (12 mm of pericardial effusion, 53 mm of pleural effusion, CRP 20.3 mg/L, PCT <0.02 ng/ml, fibrinogen 367 mg/dL). On the 33rd day, during an outpatient visit, after normalization of hs-CRP (2.1 mg/L) and complete resolution of pericardial and pleural fluid, the dose of prednisone was gradually reduced (to 5 mg per week), which resulted in the recurrence of pericardial (10 mm) and pleural effusion (26 mm) with a significant increase of hs-CRP value (169.7 mg/L) observed during the next outpatient visit (on the 54th day). The initial dose of prednisone was administered again and maintained for another month with a gradual tapering. A follow-up examination 3 months later showed no recurrence of pericardial and pleural effusion. Six months after the IPG implantation, TAVI was performed without any complications.
Discussion
PCIS includes a group of conditions such as postpericardiotomy syndrome, postmyocardial infarction syndrome and post-traumatic pericarditis. Post-IPG implantation pleuropericarditis with initial cardiac injury involving the pericardium/ myocardium and pleura is a feature of PCIS [1]. The clinical manifestation of PCIS is nonspecific, with pleuritic chest pain (90%), dyspnea (57%), fever (66%), and pericardial friction rub (63%), with leukocytosis (49%) and elevated erythrocyte sedimentation rate (96%) in laboratory tests being the most common symptoms [8]. The symptoms can occur on day 1 or even up to 4 months after cardiac injury [8]. The frequency of pleuropericarditis after permanent pacemaker implantation is unknown. There are no standardized criteria for the diagnosis of PCIS, and the treatment is based on empirical anti-inflammatory therapy, which is used in pericarditis.
Levy et al. [3] retrospectively reviewed 395 consecutive patients after IPG implantation; 8 cases (2%) of pericarditis were detected, 2 of them accompanied pleural effusion (0.5% of analyzed population). All affected patients had undergone active fixation lead implantation in the atrial position. Pericarditis occurred 5–21 days after the IPG; 4 patients were treated with non-steroidal anti-inflammatory drugs (NSAID) and 3 with steroids. Two patients who received NSAID developed relapse and required steroid therapy. Wei-Che Tsai et al. [9] presented PCIS after dual-chamber (active fixation electrodes) IPG implantation; on the 5th day, the patient developed shortness of breath and a fever, a pericardial friction rub, leukocytosis, and elevated level of CRP. The CT scan chest showed a moderate amount of pericardial and bilateral pleural effusion. After nonsteroidal anti-inflammatory drugs (NSAIDs) therapy (naproxen and colchicine), the patient was discharged, and at follow-up 1 month later there was no sign of recurrent pericardial effusion. Additionally, Kumar et al. [10] described pleuropericarditis after IPG implantation. Firstly, pericarditis was diagnosed 2 weeks after the IPG insertion, and ibuprofen was used. Secondly, after a month, pleuritis was found with a large right-sided pleural effusion. Furthermore, Sedaghat-Hamedani et al. [8] reported a case of PCIS after cardiac resynchronization therapy (CRT-D) with increased CRP level without leukocytosis and increasing of PCT level. Initially, antibiotic therapy was used, but in the next 3 months the patient complained about shortness of breath; ECHO revealed a pericardial effusion. Then, ibuprofen was given, without any improvement. A CT chest scan reveaed a pericardial effusion with a density lower than 20 HU.
Consequently, there was an improvement after ibuprofen and prednisolone therapy was applied.
PCIS is an inflammatory process involving the pericardium and pleura in response to cardiac injury. The mechanism of IPG-induced PCIS is still unclear but may involve localized micro-trauma at the site of IPG lead insertion [10]. The increased incidence of PCIS with atrial leads is likely related to the thin atrial wall. Lead perforation can cause a change in sensing and pacing parameters. It is important to differentiate PCIS from lead perforation to prevent unnecessary therapeutic interventions. A CT scan of the chest can detect pleuropericardial involvement and can help rule out cardiac perforation. Pleuropericarditis has rarely been reported with IPG insertion. Moreover, pleural fluid analysis shows exudative effusion in the majority of cases [11]. Thus, pleural fluid analysis can provide valuable diagnostic information.
In the present case, a slight pericardial hemorrhage could have occurred on the first day after implantation, with resorption in the following days, and inflammatory reaction with pericardial and left pleural effusion afterwards, without any complaints from the patient. This was confirmed by the laboratory examination of pleural fluid, suggesting fluid density in the pericardial sac in CT and an increase in hs-CRP value with normal PCT level, resulting in the recurrence of pericardial fluid with re-increase in hs-CRP value after decreasing the prednisolone dose. If these values had not been thoroughly examined on the day of planned discharge, the pleuritis with large effusion would have been overlooked.
Conclusions
Patients with even mild pericardial effusion after IPG insertion should be followed closely due to the risk of pleuropericarditis, with consideration of anti-inflammatory treatment longer than in pericarditis.
Figures
References:
1.. Imazio M, Hoit BD, Post-cardiac injury syndromes. An emerging cause of pericardial diseases: Int J Cardiol, 2013; 168(2); 648-52
2.. Trigano AJ, Taramasco V, Paganelli F, Incidence of perforation and other mechanical complications during dual active fixation: Pacing Clin Electrophysiol, 1996; 19(11 Pt 2); 1828-31
3.. Levy Y, Shovman O, Granit C, Pericarditis following permanent pacemaker insertion: Isr Med Assoc J, 2004; 6(10); 599-602
4.. Sivakumaran S, Irwin ME, Gulamhusein SS, Senaratne MP, Postpacemaker implant pericarditis: Incidence and outcomes with active-fixation leads: Pacing Clin Electrophysiol, 2002; 25(5); 833-37
5.. Ohlow MA, Lauer B, Brunelli M, Geller JC, Incidence and predictors of pericardial effusion after permanent heart rhythm device implantation: Prospective evaluation of 968 consecutive patients: Circ J, 2013; 77(4); 975-81
6.. Aizawa K, Kaneko Y, Yamagishi T, Oozing from the pericardium as an etiology of cardiac tamponade associated with screw-in atrial leads: Pacing Clin Electrophysiol, 2001; 24(3); 381-83
7.. Adler Y, Charron P, Imazio M, 2015 ESC guidelines for the diagnosis and management of pericardial diseases: Rev Esp Cardiol (Engl Ed), 2015; 68(12); 1126
8.. Sedaghat-Hamedani F, Zitron E, Kayvanpour E, Post cardiac injury syndrome after initially uncomplicated CRT-D implantation: A case report and a systematic review: Clin Res Cardiol, 2014; 103(10); 781-89
9.. Tsai WC, Liou CT, Cheng CC, Post-cardiac injury syndrome after permanent pacemaker implantation: Acta Cardiol Sin, 2012; 28; 53-55
10.. Kumar S, Madanieh A, Patel H, Large unilateral pleural effusion with pacemaker-associated post-cardiac injury syndrome: Cureus, 2018; 10(7); e2946
11.. Bielsa S, Corral E, Bagüeeste P, Porcel JM, Characteristics of pleural effusion in acute idiopathic pericarditis and post-cardiac injury syndrome: Ann Am Thorac Soc, 2016; 13; 298-300
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133