17 February 2021: Articles 
An Unusual Maxillary Sinus Foreign Body: A Case Report
Unusual clinical course, Diagnostic / therapeutic accidents, Management of emergency care, Educational Purpose (only if useful for a systematic review or synthesis)
Maeidah A. Alrasheed1ABCD, Mohammed S. Alhaddad2ABCDEF*, Nora A. Almuhainy3ADEF, Abrar A. Almohammedali3ADEFDOI: 10.12659/AJCR.928534
Am J Case Rep 2021; 22:e928534






Abstract
BACKGROUND: Paranasal sinus foreign bodies are rarely encountered in otolaryngology practice.
CASE REPORT: We present the case of a 32-year-old man who presented to our Emergency Department with his left eye bleeding after a nail gun injury. The initial physical examination revealed the presence of a left eye ruptured globe, which led to left eye blindness. An urgent plain X-ray scan was done, in which the presence of a metallic object impacted in the left maxillary sinus was demonstrated. The patient was managed surgically by an external approach using the Caldwell-Luc procedure, with no intra- or postoperative complications.
CONCLUSIONS: Paranasal sinus foreign bodies, if improperly treated, can cause serious morbidity. Surgical removal, either endoscopically or through an external approach, is required.
Keywords: Foreign Bodies, Maxillary Sinus, Paranasal Sinuses, Paranasal Sinus Diseases, Postoperative Complications, Radiography
Background
Foreign bodies are frequently encountered in ENT practice, and are commonly found in the nasal cavities, ears, and pharynx [1]. However, a foreign body in the paranasal sinuses is rare, about 80% of which occur in the maxillary sinus [1,2].
There are 2 main causes of paranasal sinus foreign bodies. The most common is iatrogenic, which is a consequence of dental, ophthalmic, and otorhinolaryngological procedures, and makes up 60% of cases [1,2]. The other cause is traumatic incidents, which account for 25% of cases [2]. Traumatic foreign bodies can be a result of direct external trauma to the sinus, or indirectly through orbital or palate injuries [3]. Foreign bodies may consist of various substances such as dental implants, tooth roots, wooden sticks, toothpicks, needles, plastic, glass, metal, and bullets [1–3]. These are usually detected when a patient has unexplained rhinosinusitis, or as an accidental finding during radiological examination [2]. If the foreign body was not removed from the sinus, it can lead to serious complications such as sinusitis, inflammatory reactions, and fungal infections [1,4].
There are different methods used to extract foreign bodies from the sinus. The type of management is determined by the size, shape, and location of the foreign body [2,3]. The Caldwell-Luc procedure, the lateral window approach, and endoscopic sinus surgery are common procedures used for the removal of foreign bodies [4,5].
This report presents a case of a foreign body identified in the maxillary sinus caused by penetration of the orbital cavity, which was removed by Caldwell-Luc procedure.
Case Report
A 32-year-old man, working as a laborer and not known to have any medical illness, presented to the ER with bleeding in the left eye after trauma 1 hour earlier.
The patient sustained the injury while he was using a nail gun to fix a nail in a roof. The nail reflected from the roof to his left eye, and he presented to the ER 1 hour after the time of injury, with bleeding and severe pain in the left eye.
It was associated with loss of vision from the left eye and paresthesia and numbness in the left side of the face.
On examination the patient was conscious and was alert and oriented to time and place on arrival to the ER. He was in severe pain, with active bleeding in the left eye. His vital signs were stable.
The patient presented with a severe rupture globe injury with no light-perception vision. The rupture globe injury led to uveal prolapse, hemorrhagic choroidal detachment, and retinal detachment in all 4 quadrants. The case was managed by the Ophthalmology Department, with poor outcomes. The final result was complete loss of vision in the left eye.
The patient was sent to the Radiology Department for a plain head X-ray (anterior-posterior [AP] and lateral). The X-ray showed an abnormal curved radio-opaque shadow (metallic object) projected over the left maxillary antra with a pointed end extending to the left alveolar margin (Figure 1).
Then, the patient was prepared and shifted to the operating room (OR) immediately as an emergency case in order to save the left eye. In the OR, the ruptured globe was assessed and evaluated as a full-thickness scleral wound extending from the limbus all the way posteriorly, involving damage to the rectus muscle and loss of nonviable uveal tissue. The wound was sutured with a Vicryl 8.0 suture, and the full-thickness wound in the upper lid involving the lid margin was sutured with 6.0 Vicryl.
A CT scan with 3D reconstruction for sinus and paranasal sinus without contrast was done after the stabilization of the patient by the ophthalmology team in the OR. The CT scan showed a ruptured left globe with fracture of the left inferior orbital wall, which was identified as the region of the nail entry, fat herniation from the same opening, and a retained large dense foreign body in the left maxillary sinus (Figure 2).
An endoscopic examination was done, in which nasal cavity and nasal mucosa were found to be normal, without any obvious injury. The patient was prepared for surgery the next day to remove the nail from the maxillary sinus using Caldwell-Luc procedure.
After opening the maxillary antrum in the OR, a nail was found impacted in the inferior maxillary wall in the second premolar region (Figure 3). Premolar teeth were stable, with no perfo-ration in the hard palate.
The foreign body (the nail) was identified and removed (it was about 4 cm in length) (Figure 4).
Irrigation of the maxillary sinus with diluted betadine was performed. The sublabial incision was closed with catgut suture 2.0.
A plain X-ray was repeated after surgery, showing mild bilateral opacification of the maxillary antra.
Finally, follow up with the patient was conducted 1 week after the operation, in an out-patient clinic. There was complete loss of vision in the left eye. The original wound and the wound resulting from the Caldwell-Luc operation were within normal parameters of healing, without any infection or signs of inflammation.
Discussion
Foreign bodies (FB) can be presented in the maxillary sinus by traumatic or non-traumatic causes.
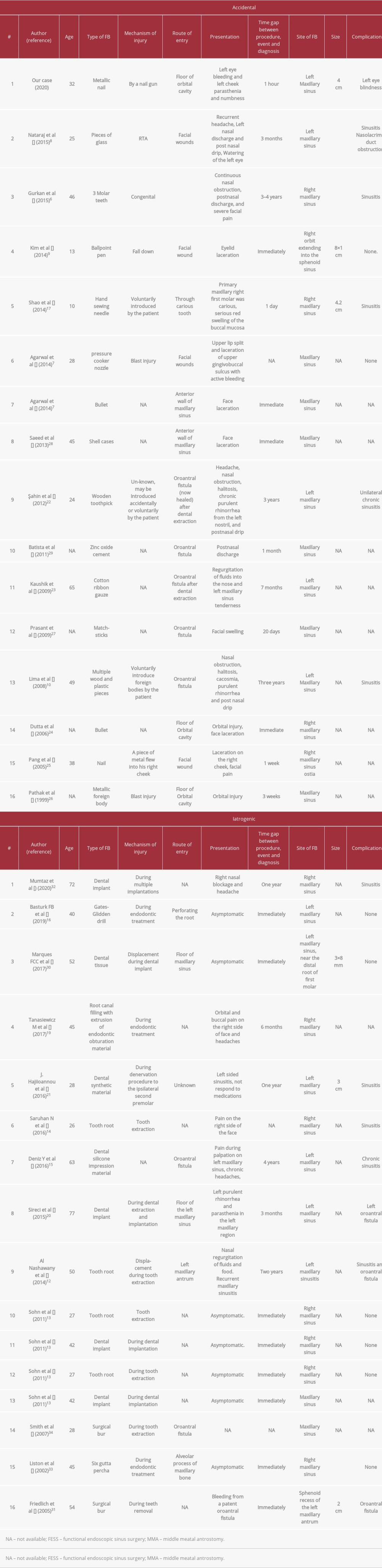
Gurkan et al (2014) found ectopic 3rd molar teeth in the right maxillary sinus as a non-traumatic cause [6]. The traumatic causes can be classified as accidental or iatrogenic [7]. The presence of pieces of glass [8], a ballpoint pen [9], and multiple wood and plastic pieces [10] are considered accidental causes.
On review of literature, the majority of iatrogenic cases are caused by the presence of tooth implants (54%) [11], tooth root [12–14], and surgical bur [15] (Table 1).
There are some similar cases in which a metallic foreign body presented in the maxillary sinus [16,17].
Patients with FB in the sinuses can present with mild fever, facial pain, headache, nasal obstruction, and chronic nasal discharge [18]. Some patients have been found to have a FB in the sinuses without any symptoms. However, the FB should be removed to avoid tissue reactions and prevent sinusitis [19].
The mechanism of sinusitis caused by FBs is unknown. It has been suggested that FBs can lead to ciliary insufficiency by causing tissue reaction and producing chronic irritation of the mucosa [19].
In the current case, the patient presented with paresthesia and numbness in the left side of the face. These symptoms could be explained by an injury to the infraorbital nerve through the opening of the infraorbital bone by the FB. Similar studies showed the same presentation in patients with infraorbital nerve injury [20].
In cases of foreign bodies in paranasal sinuses, the definite diagnosis is reached by radiological investigations [20]. Routine radiographs in at least 2 projections, or Waters’ radiograph, can usually determine the location and content of radiopacity [21]. The panoramic view is also effective in detecting foreign bodies in maxillary sinus [21]. However, a computed tomography (CT) scan is more accurate than a plain radiograph. CT can assess the shape, size, and exact location of a foreign body as well as capture thin cross-sections and multiple views [20,21]. CT is considered the most beneficial imaging study because of its ability to visualize both bone and soft tissue [21]. CT scanning is essential in planning the surgical approach [20].
Another choice in evaluation of the paranasal sinuses is cone beam computed tomography (CBCT). It has advantages over the other imaging modalities in that there is low radiation exposure while still giving good imaging quality and resolution [22]. However, this imaging modality is not available in our hospital.
In the reported case above, radiological investigations were done after the eye operation, given that the patient had active severe bleeding and required stabilization. First, we requested plain radiographs. Since they were insufficient, we performed a CT scan to identify the exact location and position of the foreign body, and to better visualize the sinus walls.
Middle meatal antrostomy (MMA) could be considered as one of the choices of FB removal from the maxillary sinus, but it is not the best due to a high failure rate without guarantee of better surgical outcomes [23].
The Caldwell-Luc approach has been used for more than 100 years [12] and is still the mainstay of surgical treatment of maxillary sinus disease after the failure of middle meatal antrostomy [11].
Despite the advanced endoscopic techniques, the Caldwell-Luc procedure remains important for its easier and safer access to the anterior wall and floor of the maxillary sinus compared to the endoscopic procedure and its indications. These indications include the removal of foreign bodies that are impacted in regions not visible or accessible with endoscopic instruments, excision of benign tumors involving the antrum, visualization of orbital floor during orbital floor decompression for Graves ophthalmopathy, access to the pterygomaxillary space, and endoscopic surgical failures [24].
In our case, we decided to perform the Caldwell-Luc procedure because the FB was large in size, impacted in the second pre-molar region, and the lateral nasal wall was clear without any signs of injury or opening.
Conclusions
In paranasal sinuses, foreign bodies are rarely encountered. The choice of the surgical approach depends on the location and the size of the foreign body. In this case, the endoscopic approach was not feasible, and the Caldwell-Luc procedure yielded excellent outcomes. The aim of presenting such cases is to give an overview of how to approach a case with an impacted metallic nail in the maxillary sinus, and choose the best way to remove it.
Figures
References:
1.. Lima M, Moreira C, da Silva V, de Freitas M, 34 Self-inflicted foreign bodies in the maxillary sinus: Braz J Otorhinolaryngol, 2008; 74(6); 948
2.. Agarwal S, Kumar S, Foreign bodies in maxillary sinus: Causes and management: Astrocyte, 2014; 1(2); 89-92
3.. Kim S, Cho K, A case of a tubular foreign body in the paranasal sinus after penetrating orbital injury: J Med Cases Jan, 2014; 5(1); 45-48
4.. Sohn D, Jung H, Kim K, Removal of displaced foreign body from the maxillary sinus using replaceable bony windows and saline irrigation, followed by suctioning of the foreign body: Implant Dent, 2011; 20(2); 112-17
5.. Agbara R, Fomete B, Omeje K, Onyebuchi P, Is the Caldwell-Luc operation and its modifications still useful in the era of endoscopic sinus surgery? Findings from a resource-limited setting: J Stoma, 2019; 72(2); 63-69
6.. Kayabasoglu G, Karaman M, Kaymaz R, Nacar A, A rare entity causing chronic sinusitis: Ectopic tooth in maxillary sinus: European Journal of General Medicine, 2015; 12(1); 86-89
7.. Agarwal S, Kumar S, Foreign bodies in maxillary sinus: Causes and management: Astrocyte, 2014; 1(2); 89
8.. Nataraj RV, Jagade M, Chavan R, An unusual maxillary sinus foreign body and its endoscopic assisted removal: International Journal of Otolaryngology and Head & Neck Surgery, 2014; 4(1); 38
9.. Kim SW, Cho KR, A case of a tubular foreign body in the paranasal sinus after penetrating orbital injury: Journal of Medical Cases, 2014; 5(1); 45-48
10.. Lima MM, Moreira CA, Silva VC, Freitas MR, 34 Self-inflicted foreign bodies in the maxillary sinus: Braz J Otorhinolaryngol, 2008; 74(6); 948
11.. Hara Y, Shiratsuchi H, Tamagawa T, A large-scale study of treatment methods for foreign bodies in the maxillary sinus: J Oral Sci, 2018; 60(3); 321-28
12.. Al Nashawany M, Olakunle HO, Kumar R, Endoscopic sinus surgery for the removal of foreign body (root) from the maxillary antrum: Our experience: Case Rep Int, 2014; 1(3); 1-5
13.. Sohn DS, Jung HS, Kim KH, Removal of displaced foreign body from the maxillary sinus using replaceable bony windows and saline irrigation, followed by suctioning of the foreign body: Implant Dent, 2011; 20(2); 112-17
14.. Saruhan N, Kılınç A, Tepecik T, Ertaş Ü, Foreign material in a maxillary sinus as a complication of root canal treatment: A case report: Turkish Endod J, 2016; 1(2); 96-98
15.. Deniz Y, Zengin AZ, Karli R, An unusual foreign body in the maxillary sinus: Dental impression material: Niger J Clin Pract, 2016; 19(2); 298-300
16.. Selvi F, Enöz M, Yazgin I, Do asymptomatic foreign bodies in the maxillary sinus always need to be removed?: B-ENT, 2008; 4(4); 243-47
17.. Enöz M, Selvi F, İnançlı HM, Incidentally detected asymptomatic metal foreign bodies (two nails) in shoemaker’s maxillary sinus: Kulak Burun Bogaz Ihtis Derg, 2012; 22(5); 301-4
18.. Basturk FB, Turkaydin D, Aktop S, Ovecoglu HS, An iatrogenic foreign body in the maxillary sinus: Report of an unusual case: J Otolaryngol Rhinol, 2019; 5; 54
19.. Shao L, Qin X, Ma Y, Removal of maxillary sinus metallic foreign body like a hand sewing needle by magnetic iron: Int J Clin Pediatr Dent, 2014; 7(1); 61-64
20.. Lone PA, Singh RK, Pal US, Treatment of traumatic infra orbital nerve paresthesia: Natl J Maxillofac Surg, 2012; 3(2); 218-19
21.. Tanasiewicz M, Bubilek-Bogacz A, Twardawa H, Foreign body of endodontic origin in the maxillary sinus: J Dent Sci, 2017; 12(3); 296-300
22.. Neimane L, Zamure L, Klimecs V, Cone beam computed tomography evaluation of maxillary sinus before and after sinus floor elevation. In Proceedings of the Latvian Academy of Sciences. Section B: Natural, Exact, and Applied Sciences, 2019; 73(4); 387-92
23.. Sireci F, Nicolotti M, Battaglia P, Canine fossa puncture in endoscopic sinus surgery: Report of two cases: Braz J Otorhinolaryngol, 2017; 83(5); 594-99
24.. Hajiioannou J, Exarchos S, Lachanas V, Bizakis J, In the era of endoscopic sinus surgery, is there still a place for the Caldwell-Luc procedure?: B-ENT, 2016; 12(2); 99-102
25.. Şahin YF, Muderris T, Bercin S, Chronic maxillary sinusitis associated with an unusual foreign body: A case report: Case Rep Otolaryngol, 2012; 2012; 903714
26.. Kaushik S, Singh A, Karthikeyan A, Unusual foreign body in the maxillary antrum: A case report: The Internet J Otorhinolaryngol, 2009; 12(2); 1-3
27.. Dutta A, Awasthi SK, Kaul A, A bullet in the maxillary sinus: Indian J Otolaryngol Head Neck Surg, 2006; 58(3); 307-9
28.. Pang KP, Siow JK, Tan HM, Migration of a foreign body in the maxillary sinus illustrating natural mucociliary action: Med J Malaysia, 2005; 60(3); 383-85
29.. Phatak S, A rare foreign body in the maxillary antrum: Indian J Otolaryngol Head Neck Surg, 1999; 52(1); 95-57
30.. Prasant MC, Bande CR, Two atypical case reports of foreign bodies in the maxillary sinus and nasal septum: J Maxillofac Oral Surg, 2009; 8(1); 88-90
31.. Saeed B, Traumatic foreign bodies in the paranasal sinuses: Jordan Medical Journal, 2013; 171(788); 1-8
32.. Batista SH, Soares ES, Costa FW, Foreign body in the maxillary sinus. Considerations on maxillary sinus approaches wound closure: Rev Stomatol Chir Maxillofac, 2011; 112(5); 316-18
33.. Marques FC, Sufredini I, Georgevich Neto R, Foreign body displacement for the maxillary sinus and surgical removal by the caldwell-luc technique: Clinical case: International Journal of Case Studies in Clinical Research, 2017; 1(4); 96-100
34.. Friedlich J, Rittenberg BN, Endoscopically assisted Caldwell-Luc procedure for removal of a foreign body from the maxillary sinus: J Can Dent Assoc, 2005; 71(3); 200-1
35.. Mumtaz M, Alotaibi NM, Alfawaz NF, Alhajri AN, Retrieval of two displaced dental implants from the maxillary sinus through Caldwell-Luc approach:A case report: International Journal of Medical and Dental Case Reports, 2020; 2020; INS161200420
36.. Liston PN, Walters RF, Foreign bodies in the maxillary antrum: A case report: Austr Dent J, 2002; 47(4); 344-46
37.. Smith JL, Emko P, Management of a maxillary sinus foreign body (dental bur): Ear Nose Throat J, 2007; 86(11); 677-78
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952909
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.950868
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952931
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.952577
Most Viewed Current Articles
07 Dec 2021 : Case report  22,759,844
22,759,844
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  176,022
176,022
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
120,540
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
65,552
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133