29 April 2021: Articles 
Two Limitations of Subcutaneous Implantable Cardioverter Defibrillator in the Same Patient Warranting Its Explant
Unusual clinical course, Unusual or unexpected effect of treatment
Rahul Dhawan1ADEF, Mansoor Ahmad1DE, Aravdeep Jhand1DE, Sumera Kanwal1DE, Adeel Jamil2DE, Faris Khan1ADEF*DOI: 10.12659/AJCR.928983
Am J Case Rep 2021; 22:e928983






Abstract
BACKGROUND: A subcutaneous implantable cardioverter defibrillator (S-ICD) is preferred over a transvenous implantable cardioverter defibrillator (TV-ICD) in selected cases owing to a lower rate of lead-related complications such as infections and venous thrombosis. However, the S-ICD has its own limitations, including inappropriate shocks due to oversensed events, and the inability to treat ventricular tachycardia (VT) below a heart rate of 170 beats per minutes (bpm). We present a patient case which showed manifestations of both of these limitations, warranting explant of the device.
CASE REPORT: A 50-year-old man with a history of nonischemic cardiomyopathy and VT had a S-ICD placed at an outside facility. However, he continued to have VT despite on anti-arrhythmic drugs and required recurrent S-ICD shocks. Device interrogation showed that he was intermittently receiving appropriate shocks for slower VT (with a heart rate ranging from 150 bpm to 160 bpm) due to oversensing of T waves. However, treatment was delayed for other VT episodes owing to appropriate sensing and the patient’s heart rate being below the lowest detection zone for S-ICD. Due to slower VT cycle length and frequent oversensed events, the S-ICD was ultimately replaced by a TV-ICD system.
CONCLUSIONS: This case report emphasizes the importance of S-ICD pre-implant vector screening and the need for paying attention to VT cycle length to prevent inappropriate device shocks and/or delayed therapies.
Keywords: Cardiac Electrophysiology, Transvenous ICD, Subcutaneous ICD, Oversensing, ventricular tachycardia, Arrhythmias, Cardiac, Defibrillators, Implantable, Electric Countershock, Tachycardia, Ventricular
Background
The subcutaneous implantable cardioverter defibrillator (S-ICD) was approved by the FDA in 2012 [1]. It works in 3 phases: a detection phase, certification phase (to remove oversensed events), and therapy decision phase, during which shock is delivered [1]. Although the S-ICD has certain advantages over a transvenous implantable cardioverter defibrillator (TV-ICD), it has limitations, including the inability to treat ventricular tachycardia (VT) below a heart rate of 170 beats per minute (bpm), oversensing that can result in inappropriate shocks (especially if not screened properly), and a lack of pacing capability. A study by Noel et al estimated oversensed events in 16% of S-ICD recipients, and 5.6% of the patients underwent device extraction due to the oversensed events [2]. We present an interesting case [3] of intermittent T-wave oversensing that led to intermittent appropriate S-ICD therapy for VT below a heart rate of 170 bpm, which was untreated at other times because of appropriate sensing.
Case Report
A 50-year-old man with a history of nonischemic cardiomyopathy (left ventricular ejection fraction of 25%) and VT had an S-ICD placed in December 2018 at an outside hospital. His symptoms during VT were palpitations and lightheadedness. He started having multiple S-ICD shocks 6 months after the S-ICD implantation. He was administered amiodarone, which had to be discontinued due to pulmonary toxicity. Treatment with sotalol and mexiletine were initiated; however, the patient continued to have recurrent VT and S-ICD shocks. He was transferred to our hospital in July 2019 for further management. Device interrogation on admission showed one VT event, which was appropriately detected and treated. However, all other VT events were in the heart rate range of 150 bpm to 160 bpm. This was under the lowest detection zone of S-ICD therapy (which is 170 bpm), but VT was inappropriately detected due to the oversensing of T waves (despite having a SMART Pass filter on) leading to appropriate S-ICD shocks (Figure 1A). There were, however, additional events where the device did not treat slow VT (heart rate around 150-160 bpm) due to appropriate sensing, leading to the absence or delay of therapy.
Due to recurrent slow VT, intermittent oversensing of T waves, and the limitation of the S-ICD detection zone to appropriately treat all VT episodes, we decided to explant the S-ICD. The patient underwent a single chamber TV-ICD implant in July 2019, and the S-ICD was turned off. Because recurrent symptomatic slow VT was appropriately detected and successfully treated with anti-tachycardia pacing by the TV-ICD system (Figure 1C), the patient underwent VT ablation in October 2019 (3 months after the TV-ICD implant and 1 month before the S-ICD explant). Substrate modification and local abnormal ventricular activity ablation was successfully performed in the basal to mid anterolateral wall of the left ventricle (Figure 1D). Treatment with mexiletine was discontinued after the ablation procedure, and sotalol was continued. The staged removal of the S-ICD was done in November 2019 (Figure 1B). Unfortunately, the S-ICD extraction was complicated by delayed pocket site infection requiring incision and drainage (I&D) and a short course of antibiotics 2 months after the S-ICD explantation.
The patient had routine follow-up visits in arrhythmia clinic, with the last visit occurring 15 months after his ablation procedure. During this visit, no additional delayed or inappropriate TV-ICD therapy was found. The patient’s treatment time-line is shown in Table 1.
Discussion
There has been an increase in the use of the S-ICD to minimize complications associated with the presence of a TV-ICD system, such as systemic infections, venous obstruction, and thrombosis [4]. A meta-analysis comparing TV-ICD and S-ICD systems showed fewer lead-related complications in the S-ICD group; however, it reported a similar infection rate in both groups. The incidence of inappropriate shocks was similar in both groups, but the TV-ICD group had inappropriate shocks primarily due to treatment of supraventricular tachycardia, whereas oversensing of T waves or noise resulted in inappropriate shocks in the S-ICD group [5]. However, none of the studies included in the meta-analysis were randomized. Only 1 randomized study compared the S-ICD and TV-ICD. That trial showed a higher trend of inappropriate shocks in the S-ICD group, which were mostly related to the oversensing of T and P waves or extracardiac stimuli, such as myopotentials and noise. However, the trial did not have sufficient power for this outcome [6]. Importantly, inappropriate therapies of TVICD are usually due to supraventricular tachycardia, which can be managed easily by reprogramming the device. However, in the S-ICD, there are limited options for managing inappropriate shocks due to oversensing [6]. There is a definite need for further studies to delineate the difference in inappropriate shocks between the 2 devices. Young patient age, small amplitude of QRS complexes, atrial fibrillation, and hypertrophic cardiomyopathy have been associated with T-wave oversensing [7,8]. Manual and automated screening tools lack specificity to select eligible patients [9,10]. The SMART Pass filter has helped reduce oversensing events [11]; however, it does not eliminate the risk of inappropriate shocks. In addition, a sensing vector may be appropriate at the time of device implantation, but it is dynamic and can result in a poor quality vector over time [2]. A rate-dependent bundle branch block can also lead to inappropriate sensing due to double counting of the notched R wave [2]. The evaluation of factors impacting clinical outcome and cost effectiveness of the S-ICD (EFFORTLESS S-ICD) registry showed that the 1-year complication rate of the S-ICD was 2%, with an inappropriate shock incidence of 1.5% [12]. Because of the potential issues of over-sensing, vigilant pre-implant screening is needed. The S-ICD is also not ideal for slow ventricular arrhythmias owing to its limitations of arrhythmia detection zone and treatment [2].
Our case describes a scenario in which appropriate screening and selection of the suitable defibrillator type to treat slower VT could have potentially avoided 3 procedures (S-ICD implantation, followed by its extraction, and then its pocket site I&D). It would have reduced the healthcare costs and improved the patient outcomes.
Conclusions
Both the S-ICD and TV-ICD have limitations. This case highlights 2 limitations of the S-ICD that hindered appropriate management of this patient’s VT, resulting in his S-ICD being replaced with a TV-ICD for appropriate management. Available options for managing the oversensing problems of the S-ICD are limited; therefore, extra diligence is needed during pre-implant vector screening. The dynamic nature of this vector should also be considered prior to device implantation. Due to SICD’s limitation to treat slower VT (tachycardia cycle length less than 170 bpm); close attention should be paid to the clinical VT cycle length prior to S-ICD implantation to avoid absence or delay of appropriate device therapies.
Tables
Table 1.. Timeline.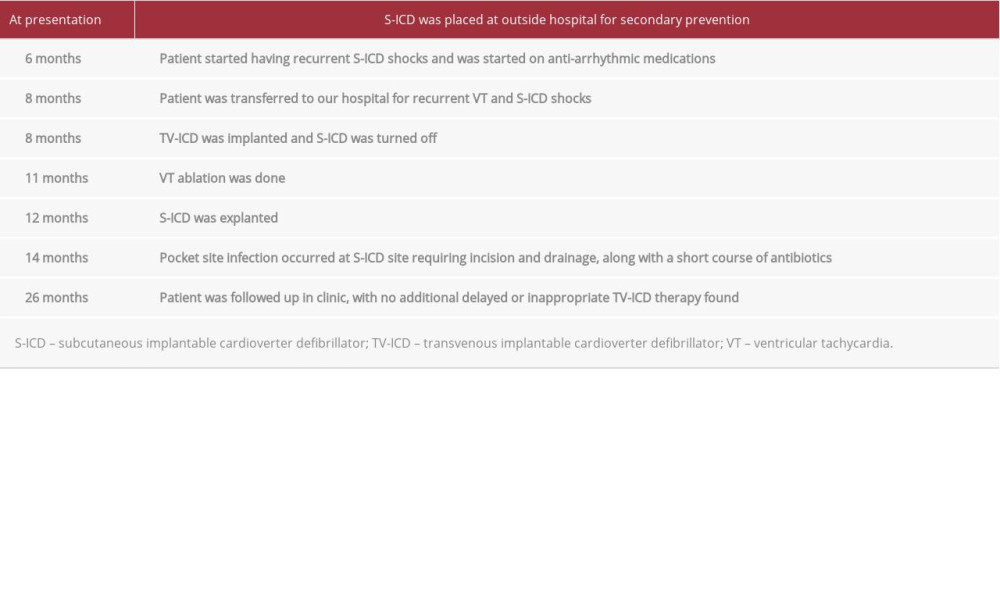
References:
1.. Brisben A, How the S-ICD (subcutaneous implantable cardiac defibrillator) senses cardiac signals to minimize cardiac over-sensing and maximize rhythm discrimination: J Electrocardiol, 2018; 51(6s); S38-43
2.. Noel A, Ploux S, Bulliard S, Oversensing issues leading to device extraction: When subcutaneous implantable cardioverter-defibrillator reached a dead-end: Heart Rhythm, 2020; 17(1); 66-74
3.. Dhawan R, Jhand A, Jamil A, Wrong decision making can rarely lead to correct management – A misbehaving tale of subcutaneous ICD: J Am Coll Cardiol, 2020; 75(11 Suppl. 1); 2635-35
4.. Viani S, Migliore F, Tola G, Use and outcomes of subcutaneous implantable cardioverter-defibrillator (ICD) after transvenous ICD extraction: An analysis of current clinical practice and a comparison with transvenous ICD reimplantation: Heart Rhythm, 2019; 16(4); 564-71
5.. Basu-Ray I, Liu J, Jia X, Subcutaneous versus transvenous implantable defibrillator therapy: A meta-analysis of case-control studies: JACC Clin Electrophysiol, 2017; 3(13); 1475-83
6.. Knops RE, Olde Nordkamp LRA, Delnoy PHM, Subcutaneous or transvenous defibrillator therapy: N Engl J Med, 2020; 383(6); 526-36
7.. El-Chami MF, Harbieh B, Levy M, Clinical and electrocardiographic predictors of T wave oversensing in patients with subcutaneous ICD: J Arrhythm, 2016; 32(3); 181-85
8.. Olde Nordkamp LR, Brouwer TF, Barr C, Inappropriate shocks in the subcutaneous ICD: Incidence, predictors and management: Int J Cardiol, 2015; 195; 126-33
9.. Bögeholz N, Pauls P, Güner F, Direct comparison of the novel automated screening tool (AST) versus the manual screening tool (MST) in patients with already implanted subcutaneous ICD: Int J Cardiol, 2018; 265; 90-96
10.. Groh CA, Sharma S, Pelchovitz DJ, Use of an electrocardiographic screening tool to determine candidacy for a subcutaneous implantable cardioverter-defibrillator: Heart Rhythm, 2014; 11(8); 1361-66
11.. Theuns D, Brouwer TF, Jones PW, Prospective blinded evaluation of a novel sensing methodology designed to reduce inappropriate shocks by the subcutaneous implantable cardioverter-defibrillator: Heart Rhythm, 2018; 15(10); 1515-22
12.. Boersma L, Barr C, Knops R, Implant and midterm outcomes of the sub-cutaneous implantable cardioverter-defibrillator registry: The EFFORTLESS study: J Am Coll Cardiol, 2017; 70(7); 830-41
In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133