24 March 2021: Articles 
“Double Trouble”: Severe Meningoencephalitis Due to and Powassan Virus Co-Infection Successfully Treated with Intravenous Immunoglobulin
Unusual or unexpected effect of treatment, Rare coexistence of disease or pathology
Igor Dumic12ABCDEFG*, Bridget Glomski3ABCDEFG, Janki Patel4CD, Terri Nordin23E, Charles W. Nordstrom12EG, Lawrence J. Sprecher12EG, Eric Niendorf5BE, Amteshwar Singh6DEF, Kosana Simeunovic7AF, Anand Subramanian12CD, Oladapo Igandan12EG, Danilo Vitorovic8ACDEFDOI: 10.12659/AJCR.929952
Am J Case Rep 2021; 22:e929952






Abstract
BACKGROUND: Powassan virus (POWV) is an emerging tick-borne flavivirus transmitted to humans by ticks. While infection is asymptomatic in some people, others develop life-threatening encephalitis with high mortality rates. Co-infection between POWV and Borrelia burgdorferi is rare despite the fact that both pathogens can be transmitted through the same tick vector, Ixodes scapularis. It is unclear if co-infection leads to more severe clinical presentation and worse outcome.
CASE REPORT: A 76-year-old Wisconsin man was admitted for meningoencephalitis complicated by hypoxemic and hypercapnic respiratory failure requiring endotracheal intubation. The patient had no known tick bites but lived in a heavily wooded area. Extensive work-up for infectious, autoimmune, and paraneoplastic causes was positive for Borrelia burgdorferi and Powassan virus infection (POWV). Following treatment with ceftriaxone for neuroborreliosis and supportive care for POWV infection, the patient failed to improve. Intravenous immunoglobulins (IVIG) were started empirically, and the patient attained gradual neurological improvement and was successfully extubated.
CONCLUSIONS: Treatment for POWV infection is supportive, and at this time there are no approved targeted antivirals for this disease. At this time, it remains unclear if co-infection with 2 pathogens leads to a more severe clinical presentation and higher mortality. In the absence of contraindications, IVIG might be beneficial to patients with POWV infection who are not improving with supportive care.
Keywords: Encephalitis, Tick-Borne, Immunoglobulins, Intravenous, Lyme Disease, Powassan virus, co-infection, Borrelia burgdorferi, coinfection, Encephalitis Viruses, Tick-Borne, Meningoencephalitis
Background
Powassan virus (POWV) is an emerging tick-borne flavivirus named after the city of Powassan in the Canadian province of Ontario where it was first described in a 5-year-old boy who tragically died from severe encephalitis [1]. Unlike other flavi-viruses, which are transmitted to humans by mosquitos, the vectors for POWV and the eastern hemisphere’s tick-borne encephalitis (TBE) virus are ticks. Since its discovery, 2 sero-logically indistinguishable yet distinct genotypes have been described: POWV lineage I (prototype POWV) transmitted by
In the United States the disease is most prevalent in the Northeast and the upper Midwest, and this geographical distribution mirrors those of
Neurologic manifestations of Lyme disease (LD) and POWV infection are protean. Encephalitis is a common presentation of POWV infection, while aseptic meningitis is the most common clinical manifestation of Lyme neuroborreliosis (LNB) [7,8]. While there is a well-established treatment protocol for LNB, the care of patients with POWV infection is primarily supportive. Some case reports have described successful outcomes with immunosuppressive therapy in patients with severe POWV encephalitis, yet no rigorous study has been performed due to the rarity of the disease.
Here, we report a patient who developed severe meningoencephalitis due to LD and POWV co-infection. Treatment for LD with intravenous ceftriaxone failed to yield neurologic improvement. He was subsequently given intravenous immunoglobulins (IVIG) for POWV encephalitis, which did result in gradual neurologic recovery.
Case Report
A 76-year-old Wisconsin man was brought in by his daughter for abrupt onset of fever and confusion with onset 1 day prior. The patient had been born and raised in Wisconsin and lived in a heavily wooded area. He had no domestic or international travel within the last year. He was a nonsmoker, drank socially, denied illicit drug use, and had no pets. He had reported no known tick bites. His medical history was significant for well-controlled hypertension, hyperlipidemia, depression, type II non-insulin-dependent diabetes mellitus, and remote history of prostate cancer. His home medication regimen included Atorvastatin, Lisinopril/Hydrochlorothiazide, Clonidine, Sertraline, and Terazosin. The surgical history was relevant for prostatectomy approximately 10 years prior.
The patient presented to the emergency department with normal vital signs aside from a fever of 38.8°C. A physical exam revealed a well-developed man in no distress, who was somnolent but arousable, and able to protect his airway. He had positive meningeal signs and notable asterixis. Results of a limited neurological exam were consistent with encephalopathy with inattention, absence of spontaneous speech, and inability to follow commands. He moved all 4 extremities spontaneously, his muscle stretch reflexes were normal and symmetric, and both Babinski and Hoffman signs were absent bilaterally. His sensory and cranial nerve exams were unremarkable as assessed within the limitations of his encephalopathy. Results of heart, lung, and abdominal exams were normal. A skin exam revealed no rash.
Complete blood cell count was significant for mild thrombocytopenia of 134×109/L. Liver and renal function were normal, and electrolytes were significant for hypokalemia of 3 mmol/L. EKG demonstrated normal sinus rhythm. Computed tomography of the head was negative for intracranial hemorrhage, acute ischemic infarct, encephalomalacia, or any mass lesion. Cerebrospinal fluid (CSF) was clear and contained 68 total nucleated cells with 55% lymphocytes. CSF protein level was elevated at 81 mg/dl (normal level 15-45 md/dl), and CSF glucose was normal. Gram stain was negative for bacteria, and CSF cultures remained without growth. Since the patient presented in the summer and lived in an LD-endemic area, he was started empirically on ceftriaxone. Acyclovir was also started empirically for herpes simplex virus (HSV) coverage.
The following day the patient’s condition further deteriorated. His fever recurred with worsening encephalopathy, obtundation, and myoclonus. He developed hypoxemic and hyper-capnic respiratory failure requiring intubation and mechanical ventilation. A repeat lung exam remained normal, and a chest X-ray was negative for pulmonary infiltrates, pleural effusion, or pulmonary vascular congestion. A comprehensive work-up for infectious, autoimmune, and paraneoplastic causes of encephalopathy was performed (Table 1). Electroencephalography (EEG) demonstrated diffuse slowing of background, but neither epileptiform discharges nor electrographic seizures were captured. Magnetic resonance imaging (MRI) of the brain with and without contrast was interpreted as normal (Figures 1, 2). Cyproheptadine was empirically given due to suspicion for serotonin syndrome, but this failed to improve his neurological status. The patient was continued on supportive care, and intravenous ceftriaxone was continued following initial CSF lab tests returning positive for both POWV and LD. He was maintained on Ceftriaxone IV for another week, yet remained obtunded and failed multiple attempts at weaning from mechanical ventilation. Intravenous immunoglobulin (IVIG) was started on day 8 of his hospitalization at a dose of 1g daily for 5 days. Following the third dose of IVIG, the patient’s mental status gradually started to improve. He was more awake, cooperative, and intermittently following commands. After completion of the IVIG course, the patient further improved, and was subsequently extubated. He remained in the hospital for total of 36 days, and was discharged to a skilled nursing facility to continue physical rehabilitation. Two months following his critical illness, the patient continued to depend on a walker, and continued to exhibit intermittent memory impairment.
Discussion
Encephalitis is a neurological emergency defined as inflammation of the brain parenchyma, and manifested by personality changes or altered mental status in combination with 2 or more of the following: fever, focal neurological deficit, seizures, CSF pleocytosis, EEG abnormalities, or imaging suggestive of encephalitis [10]. If the meninges are affected by a pathological process, then a patient will experience the classic hallmarks of meningitis, including fever, headache, and nuchal rigidity. Due to the close proximity of brain parenchyma to the subarachnoid space and CSF, both processes can occur concurrently, presenting as meningoencephalitis [10,11].
In an immunocompetent host, such as our patient, encephalitis is most commonly caused by neurotropic viruses. Inflammatory/ autoimmune diseases and paraneoplastic phenomena are other causes of encephalitis [10–12]. Community-acquired meningitis, on the other hand, is most commonly due to encapsulated bacterial pathogens such as
While some neurotropic viruses cause disease predominantly in children (eg, La Crosse virus), others more commonly cause severe encephalitis in the elderly (eg, West Nile virus) [12].
Similar to HSV type I (the most common cause of viral encephalitis across all age groups), POWV and LD also have no age predilection [11,12].
As with any neuro-infection, the diagnosis of POWV and LNB rests on appropriate epidemiological data, clinical manifestations, and the detection of a pathogen or specific antibodies in blood and/or CSF Our patients extensive work up returned positive only for
Lymphocytic pleocytosis is the most common CSF finding in patients with meningitis due to LNB and POWV encephalitis. CSF protein level may be slightly elevated, while CSF glucose levels are expected to be normal. CSF Gram stain and cultures are negative, which, when taken together with other findings, help exclude bacterial meningitis. Imaging and EEG findings in POWV are nonspecific. EEG shows diffuse and severe slowing in up to 80% of patients, while around one-third of patients have epileptiform waveforms [9]. MRI imaging findings in POWV encephalitis are either nonspecific or normal, as was documented in our patient.
MRI is the best imaging modality to detect brain changes in encephalitis [10]. MRI is abnormal in more than 90% of patients with HSV encephalitis, while in cases of autoimmune or paraneoplastic encephalitis, it may be normal or with very subtle changes [10,11]. Due to the small number of cases, our understanding of specific MRI changes in cases of POWV encephalitis is limited. In addition, most cases have nonspecific findings which cannot be used to differentiate POWV encephalitis from other etiologies. In one review, only 12 of 102 patients with TBE had MRI abnormalities, and the thalami were most commonly affected in this group of patients [7,14]. Hemorrhagic involvement of bilateral thalami has been described as well [15]. One retrospective case series suggested that patients with POWV encephalitis with brainstem involvement on MRI have a worse prognosis [9]. In cases with POWV rhombencephalitis, the MRI might be normal and the absence of MRI changes might suggest a favorable prognosis [16].
While
LNB should be treated with 4 weeks of ceftriaxone [19]. In some cases of LNB, steroids have been used successfully, although there is a lack of consensus about their efficacy [20]. Conversely, there is no proven effective therapy for POWV encephalitis, and the care is supportive [21]. The fact that in some cases patients favorably responded to immunosuppressive therapy [6,7,9,16] poses an intriguing question about whether, in addition to direct viral pathological effects, the patient’s immune system might play a significant role in the pathogenesis of POWV infection [16]. Hence, use of immunosuppressive therapy in the form of steroids or IVIG has been attempted in some cases of POWV encephalitis. In a retrospective study, none of the patients treated with IV steroids died [9]. In the only case reported to date (excluding ours), the use of IVIG for POWV encephalitis resulted in an excellent outcome [7]. Our patient is only the second reported case of POWV encephalitis that had improvement with IVIG despite having the severe form of the disease.
There has been no trial testing either steroids or IVIG for the treatment of patients with POWV encephalitis. One double-blind, placebo-controlled trial of patients with Japanese encephalitis did not show a clear benefit of IVIG; however, it was not powered for a clinical end-point [22]. Another trial that tested safety and tolerability of IVIG in patients with West Nile encephalitis also failed to demonstrate any statistically significant benefit [23]. Consequently, the use of immunosuppressive therapy remains experimental until more rigorous studies are conducted. In cases of severe POWV encephalitis, and in the absence of contraindications, we recommend the use of either steroids or IVIG.
Patients with POWV encephalitis have a protracted hospital course, and the majority of patients need prolonged physical rehabilitation following the acute illness. As many as 50% of POWV encephalitis survivors remain with some form of neuropsychological impairment, and the prevalence of behavioral, emotional, and cognitive deficits remains high up to 3 years following onset of the illness [10,24].
Conclusions
We describe a patient who developed severe meningoencephalitis secondary to co-infection with
Figures
References:
1.. McLean DM, Donohue WL, Powassan virus: Isolation of virus from a fatal case of encephalitis: Can Med Assoc J, 1959; 80(9); 708-11
2.. Dupuis AP, Peters RJ, Prusinski MA, Isolation of deer tick virus (Powassan virus, lineage II) from Ixodes scapularis and detection of antibody in vertebrate hosts sampled in the Hudson Valley, New York State: Parasites Vectors, 2013; 6; 185
3.. Cavanaugh CE, Muscat PL, Telford SR, Fatal deer tick virus infection in maine: Clin Infect Dis, 2017; 65(6); 1043-46
4.. Johnson TL, Graham CB, Maes SE, Prevalence and distribution of seven human pathogens in host-seeking Ixodes scapularis (Acari: Ixodidae) nymphs in Minnesota, USA: Ticks Tick Borne Dis, 2018; 9(6); 1499-507
5.. Frost HM, Schotthoefer AM, Thomm AM, Serologic evidence of powassan virus infection in patients with suspected Lyme disease: Emerg Infect Dis, 2017; 23(8); 1384-88
6.. Knox KK, Thomm AM, Harrington YA, Powassan/deer tick virus and Borrelia Burgdorferi infection in Wisconsin tick populations: Vector Borne Zoonotic Dis, 2017; 17(7); 463-66
7.. Piantadosi A, Rubin DB, McQuillen DP, Emerging cases of powassan virus encephalitis in New England: Clinical presentation, imaging, and review of the literature: Clin Infect Dis, 2016; 62(6); 707-13
8.. Halperin JJ, Nervous system Lyme disease: Handb Clin Neurol, 2014; 121; 1473-83
9.. El Khoury MY, Camargo JF, White JL, Potential role of deer tick virus in Powassan encephalitis cases in Lyme disease-endemic areas of New York, U.S.A: Emerg Infect Dis, 2013; 19(12); 1926-33
10.. Ellul M, Solomon T, Acute encephalitis – diagnosis and management: Clin Med (Lond), 2018; 18(2); 155-59
11.. van de Beek D, Brouwer M, Hasbun R, Community-acquired bacterial meningitis: Nat Rev Dis Primers, 2016; 2; 16074
12.. Tyler KL, Acute viral encephalitis: N Engl J Med, 2018; 379(6); 557-66
13.. Lindquist L, Vapalahti O, Tick-borne encephalitis: Lancet, 2008; 371(9627); 1861-71
14.. Kaiser R, The clinical and epidemiological profile of tick-borne encephalitis in southern Germany 1994–98: A prospective study of 656 patients: Brain, 1999; 122(Pt 11); 2067-78
15.. Choi EE, Taylor RA, A case of Powassan viral hemorrhagic encephalitis involving bilateral thalami: Clin Neurol Neurosurg, 2012; 114(2); 172-75
16.. Dumic I, Madrid C, Vitorovic D, Unusual cause at an unusual time-Powassan virus rhombencephalitis: Int J Infect Dis, 2020; 103; 88-90
17.. Khan AM, Shahzad SR, Ashraf MF, Naseer U, Powassan virus encephalitis, severe babesiosis and lyme carditis in a single patient: BMJ Case Rep, 2019; 12(11); e231645
18.. Dumic I, Severnini E, “Ticking bomb”: The impact of climate change on the incidence of Lyme disease: Can J Infect Dis Med Microbiol, 2018; 2018; 5719081
19.. Wormser GP, Dattwayler RJ, Shapiro ED, The clinical assessment, treatment and prevention of Lyme disease, human granulocytic anaplasmosisand babesiosis: Clinical practice guidelines by Infectious Disease Society of America: Clin Infect Dis November 9, 2006; 43; 1089-34
20.. Dumic I, Vitorovic D, Spritzer S, Acute transverse myelitis – A rare clinical manifestation of Lyme neuroborreliosis: IDCases, 2018; 15; e00479
21.. Hermance ME, Thangamani S, Powassan Virus: An emerging arbovirus of public health concern in North America: Vector Borne Zoonotic Dis, 2017; 17(7); 453-62
22.. Rayamajhi A, Nightingale S, Bhatta NK, A preliminary randomized double-blind placebo-controlled trial of intravenous immunoglobulin for Japanese encephalitis in Nepal: PLoS One, 2015; 10(4); e0122608
23.. Hart J, Tillman G, Kraut MA, West Nile virus neuroinvasive disease: Neurological manifestations and prospective longitudinal outcomes: BMC Infect Dis, 2014; 14; 248
24.. Mailles A, De Broucker T, Costanzo P, Long-term outcome of patients presenting with acute infectious encephalitis of various causes in France: Clin Infect Dis, 2012; 54(10); 1455-64
Figures
Tables
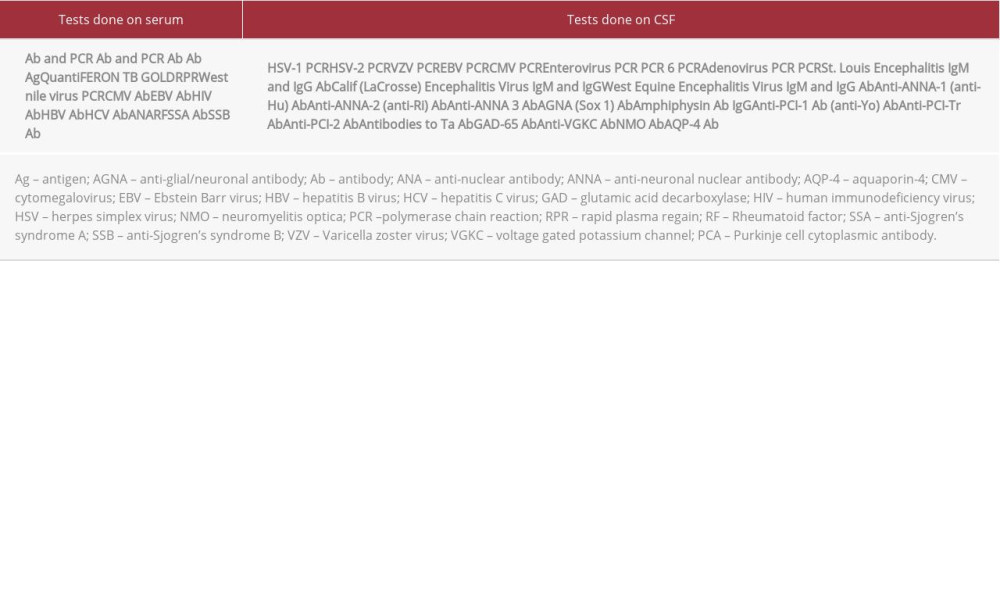 Table 1.. Summary of negative diagnostic tests that were done in our patient to rule out autoimmune, infectious, and paraneoplastic etiologies of encephalitis. Positive tests included: B. burgdorferi serum IgM and IgG, B. burgdorferi PCR in CSF (Mayo Medical Laboratories), and CSF IgM and plaque reduction neutralization test (PRNT) against POWV (CDC, Arboviral Disease Branch, Fort Collins, CO, USA).Table 1.. Summary of negative diagnostic tests that were done in our patient to rule out autoimmune, infectious, and paraneoplastic etiologies of encephalitis. Positive tests included: B. burgdorferi serum IgM and IgG, B. burgdorferi PCR in CSF (Mayo Medical Laboratories), and CSF IgM and plaque reduction neutralization test (PRNT) against POWV (CDC, Arboviral Disease Branch, Fort Collins, CO, USA).
Table 1.. Summary of negative diagnostic tests that were done in our patient to rule out autoimmune, infectious, and paraneoplastic etiologies of encephalitis. Positive tests included: B. burgdorferi serum IgM and IgG, B. burgdorferi PCR in CSF (Mayo Medical Laboratories), and CSF IgM and plaque reduction neutralization test (PRNT) against POWV (CDC, Arboviral Disease Branch, Fort Collins, CO, USA).Table 1.. Summary of negative diagnostic tests that were done in our patient to rule out autoimmune, infectious, and paraneoplastic etiologies of encephalitis. Positive tests included: B. burgdorferi serum IgM and IgG, B. burgdorferi PCR in CSF (Mayo Medical Laboratories), and CSF IgM and plaque reduction neutralization test (PRNT) against POWV (CDC, Arboviral Disease Branch, Fort Collins, CO, USA). In Press
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953173
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133