12 November 2021: Articles 
Concurrent Breast Carcinoma and Follicular Lymphoma: A Case Series
Challenging differential diagnosis, Rare coexistence of disease or pathology
Tabinda Saleem1EF*, Kaihong Mi12EF, Rajan Pathak1F, Kolsoum Yari1EF, Kit Lu12ADEFDOI: 10.12659/AJCR.931772
Am J Case Rep 2021; 22:e931772






Abstract
BACKGROUND: The incidence of multiple primaries in cancer patients is 2-17%. However, the synchronous co-occurrence of adenocarcinoma of the breast and follicular lymphoma is rare.
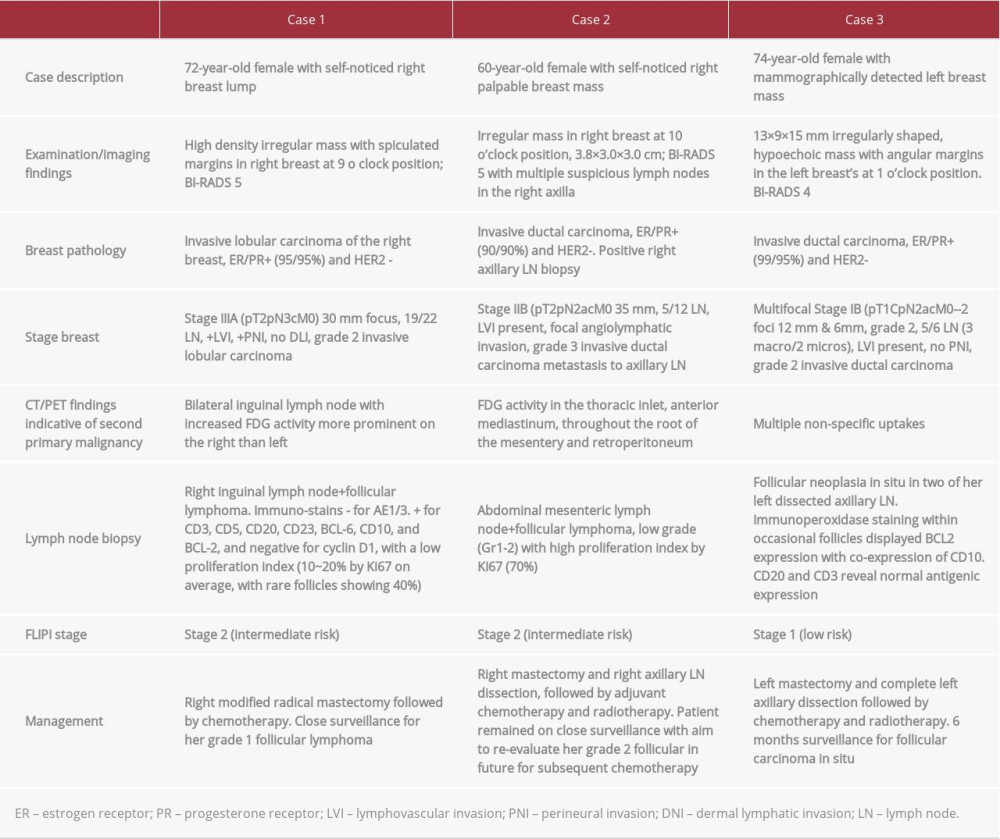
CASE REPORT: We describe a case series of 3 post-menopausal women who presented to our institute with a breast lump. On further investigations, 2 of them had invasive ductal carcinoma and 1 had invasive lobular carcinoma of the breast. All 3 cancers were estrogen/progesterone receptor (ER/PR)-positive and human epidermal growth factor receptor 2 (HER-2)-negative. During the staging PET scans, all 3 patients had increased FDG uptake in axillary, mesenteric, and inguinal lymph nodes, respectively, raising concerns for metastatic disease. However, subsequent biopsies revealed them as follicular lymphomas occurring as a second concurrent primary malignancy. All patients underwent radical mastectomies with sentinel lymph node dissection followed by chemotherapy and hormonal therapy. Most of the lymphomas were low grade, which the oncologist closely followed.
CONCLUSIONS: Very few cases of breast cancer and follicular lymphoma co-occur; this is not limited to the axillary lymph nodes and can occur in any part of the lymphatic chain. Regional lymph node enlargement detected on examination or imaging does not always indicate metastasis. A high index of suspicion is needed followed by lymph node biopsy to rule out any second primary malignancy.
Keywords: Breast Neoplasms, Lymphoma, Follicular, Neoplasms, Second Primary, Axilla, Female, Humans, Sentinel Lymph Node Biopsy
Background
Multiple synchronous or metachronous malignant primaries are known entities that occur in 2–17% of cancer cases [1–4]. However, the synchronous breast cancer and lymphomas is rare and can pose a significant diagnostic and management challenge to the treating physicians.
Herein, we report a series of t3 patients with synchronous breast adenocarcinoma and follicular lymphoma, their management, and outcome.
Case Reports
CASE 1:
A 72-year-old post-menopausal woman with no family history of breast carcinoma initially presented with a self-noticed right breast lump. A bilateral diagnostic mammogram revealed a high-density, irregularly shaped mass with spiculated margins in the right breast’s outer region. Targeted bilateral ultrasound (US) confirmed the mass at 9 o’clock position, measuring 2.4×2.1×2.8 cm, BI-RADS 5.
Laboratory evaluation was unremarkable. Ultrasound-guided right breast biopsy and right axillary lymph node biopsy revealed invasive lobular carcinoma of the right breast, which was estrogen receptor (ER)- and progesterone receptor (PR)-positive (95/95%) and human epidermal growth factor receptor 2 (HER-2) receptor-negative.
The patient had enlarged bilateral superficial inguinal lymph nodes on staging computed tomography (CT) chest/abdomen/ pelvis scans. These nodes had increased radiotracer uptake on the positron emission tomography (PET)/CT scan (Figure 1).
Biopsy of the right inguinal lymph node confirmed follicular lymphoma (FL). Immuno-staining revealed that AE1/3 was negative and CD3, CD5, and CD20 were positive. These cells were also positive for CD23, BCL-6, CD10, and BCL-2 and negative for cyclin D1, with a low proliferation index (10~20% by Ki-67 on average, with rare follicles showing 40%). CD23 additionally highlighted a residual follicular dendritic meshwork.
Bone marrow aspiration and core bone biopsy did not show any malignant process (Figure 2).
Given her limited disease and asymptomatic nature, it was decided to treat her stage IIIA breast cancer first. She underwent right modified radical mastectomy followed by chemotherapy with Docetaxel and cyclophosphamide. She was closely followed for her grade 1 follicular lymphoma by the hematologist-oncologist.
CASE 2:
A 60-year-old post-menopausal woman presented with a self-noticed right palpable breast mass. She had a positive family history of breast, colon, lung, and esophageal cancers, all on the paternal side. A mammogram revealed a mass in the right breast’s upper outer quadrant, corresponding to palpable mass on the examination and suspicious lymph nodes in the right axilla. Breast US revealed an irregular mass in the 10 o’clock position of the right breast that measured 3.8×3.0×3.0 cm, BI-RADS 5. Several lymph nodes in the right axilla were also detected.
Biopsy of the right breast and right axillary LN revealed a grade 3 invasive ductal carcinoma that was ER/PR-positive (90/90%) and HER-2-negative (2+). Biopsy of the right axillary LN was positive for metastatic disease. On genetic testing, she was positive for a variant of uncertain significance in the MSH6 gene on BRCA ½ analysis.
Staging CT of the abdomen/pelvis showed no solid organ metastasis in the abdomen or pelvis. However, it revealed multiple enlarged abdominal mesenteric lymph nodes within the left mid-abdomen, left lower quadrant, and lower abdomen extending into the upper pelvis, and the mesenteric fat had a misty appearance. The size and distribution of the lymph nodes were greater than expected. There was also enlargement of the left para-aortic lymph node, with an increased number of smaller retroperitoneal lymph nodes and nonenlarged lymph nodes within the posterior mediastinum within the lower left chest. These findings were highly suspicious for a second primary malignancy in the abdomen, likely a lymphoma (Figure 3).
Biopsy of the abdominal mesenteric lymph node suggested a follicular lymphoma that was low grade (Gr 1-2) with high proliferation index by Ki-67 (70%), FLIPI score 2, low-risk category risk, radiographically stage 3, negative bone marrow biopsy, with normal flow cytometry (Figure 4).
In her case, although pathologically she was grade 1–2, the high proliferation index (>70%) was anticipated to behave more like grade 3 FL. It was recommended to treat her lymphoma. However, given low cure rates and asymptomatic nature, she initially proceeded with her stage IIB breast cancer management. She underwent a right mastectomy and right axillary lymph node dissection, followed by adjuvant chemo-therapy and radiotherapy. The patient remained on close surveillance to re-evaluate her grade 2 follicular lymphoma for subsequent chemotherapy in the future.
CASE 3:
A 74-year-old post-menopausal woman presented with a suspicious breast mass on an annual screening mammogram. Her family history was significant for breast cancer in her mother and ovarian cancer in her maternal grandmother.
Targeted ultrasound revealed a 13×9×15 mm irregularly shaped, hypoechoic mass with angular margins in the left breast at 1 o’clock position, BI-RADS 4. Laboratory evaluation was unre-markable. On genetic testing, the patient had a variant of unknown significance on ATM p.c755Y.
Left breast biopsy revealed ER/PR-positive (99/95%) and HER-2 negative, grade 2 invasive ductal carcinoma. A breast MRI was performed for other suspicious masses in the left breast, which showed additional areas of enhancement with visible nodes in the left axilla (Figure 5).
Additional left breast mass biopsy demonstrated new focuses of invasive ductal carcinoma, estrogen-positive and HER-2-negative, suggesting multifocal disease. A PET scan to evaluate the abnormal MRI and pathology did not show any other uptake focus.
She underwent left mastectomy with sentinel lymph node biopsy. She subsequently underwent complete axillary dissection and was incidentally found to have follicular neoplasia in situ in 2 of her left dissected axillary LNs. Immunoperoxidase staining within occasional follicles displayed BCL2 expression with co-expression of CD10. CD20 and CD3 revealed normal antigenic expression (Figure 6).
As the patient had follicular neoplasia in situ, which was more consistent with pre-cancerous findings vs overt lymphoma, no further workup or treatment was indicated. The patient underwent adjuvant chemotherapy and radiation therapy for her stage IIB breast cancer, followed by hormonal therapy. She remained under surveillance by the hematologist-oncologist for 6 months.
Discussion
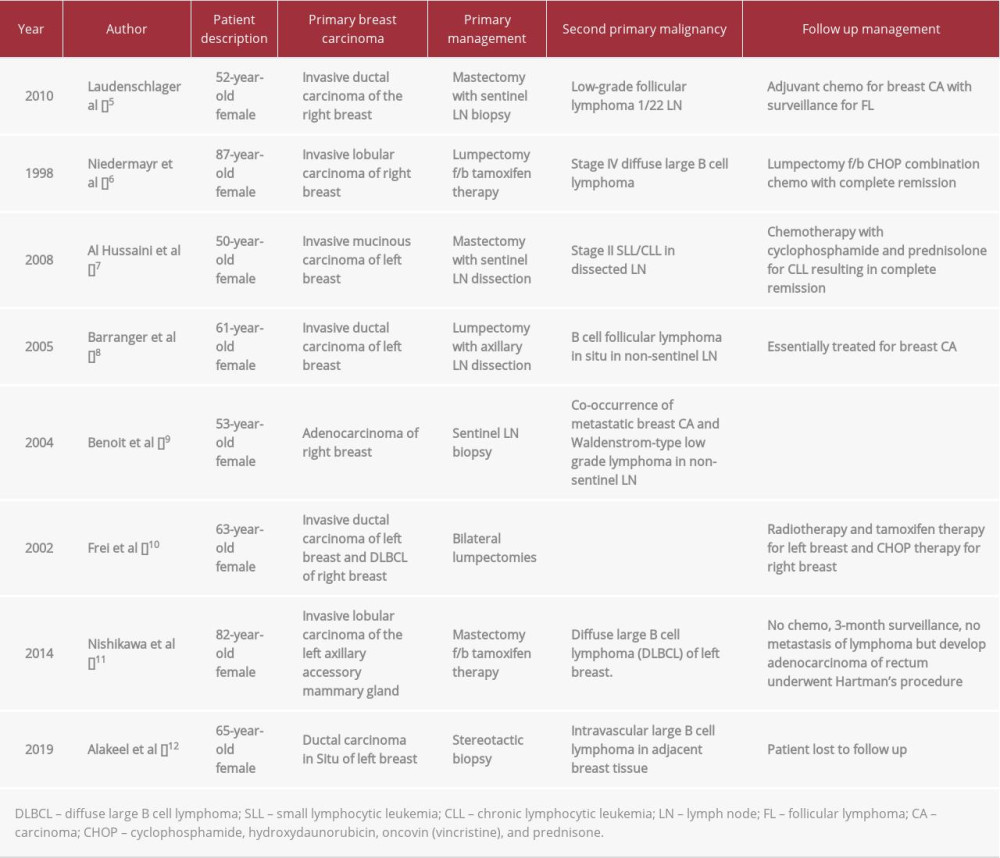
Breast cancer is the most common worldwide malignancy in females and the second most common cause of cancer-related deaths after lung cancer. The development of lymphoma following chemotherapy and radiotherapy for breast cancer is a recognized occurrence. However, the synchronous occur-rence of breast cancer and lymphoma is rare and can make the diagnostic and management approach very challenging. A summary of currently existing data on synchronous/meta-chronous occurrence of breast adenocarcinoma with lymphoma is listed in Table 2 [5–12].
It is not clear if there is a direct relationship between lymphoma and breast carcinoma regarding our reported cases. It is theorized that, given that lymphomas can weaken the immune system and disable T cell-mediated antineoplastic pathways, successive carcinomas may occur. In a report regarding a rare presentation of diffuse large B cell lymphoma (DLBCL) and rectal carcinoma [11], it was thought that the coexisting lymphoma prepped the ground by defecting the cellular immune system that triggered the development of a second malignancy in the rectum, similar to the acquired reaction caused by the Helicobacter pylori causing MALT lymphoma of the stomach. However, given that we do not know which of the primary malignancy occurred first, further evidence is needed to elucidate specific cause-and-effect relationships.
Lymphoma is a diverse group of hematologic malignancies classified as Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL). NHL is more common in adults and is derived from B cell progenitors, T cells, and, rarely, natural killer cells. Breast cancer has been reported to co-occur with other rare forms of lymphoma like intravascular large B cell lymphoma [12]. However, the association between breast cancer and lymphoma is not specific to any pathological subtypes, as cases of synchronous breast cancer and DLBCL and HL have been reported [13,14].
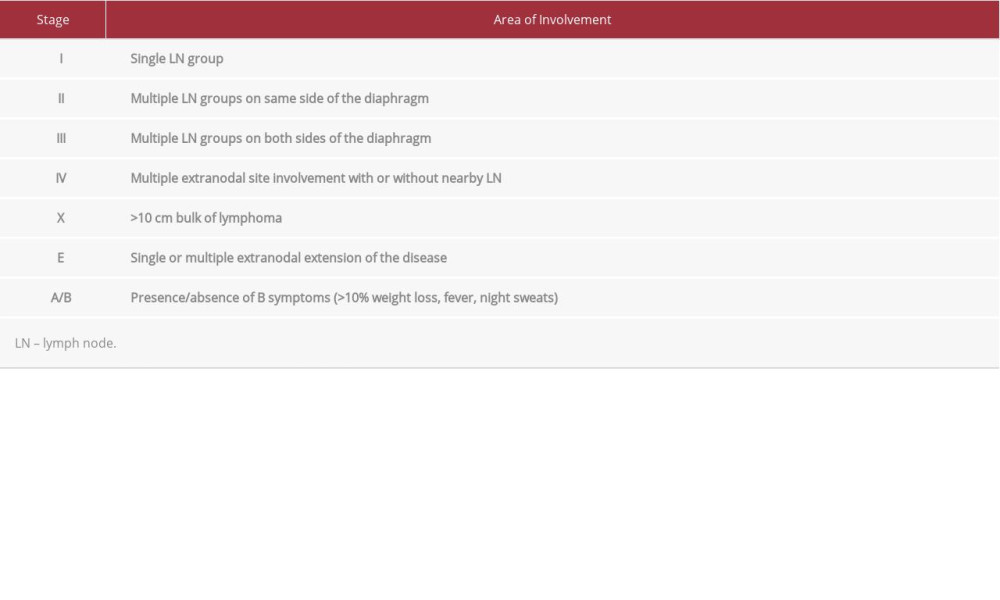
The diagnosis of lymphoma and breast cancer is especially challenging with indolent lymphomas such as follicular lymphomas (FL). Cotswold’s modified Ann Arbor staging for follicular lymphoma is described in Table 3 [15]. Patients with early-stage FL typically do not have any significant symptoms or laboratory abnormalities. Adenopathy is a common presentation of FL. However, patients with breast cancer may also present with axillary adenopathy in addition to the breast mass. Atypical presentations such as early-stage breast cancer and distant adenopathy findings may prompt the treating physicians to think of synchronous cancer rather than metastatic disease. However, if adenopathy is only presented in the axillary lymph nodes or there is locally advanced breast cancer, the diagnosis of synchronous pathology may be missed. Therefore, pathologists should consider performing a variety of immunohistochemical stainings to distinguish the different diagnoses. When there is a suspicion for lymphoma, physicians should consider performing an adequate immunohistochemistry panel including CD20, CD3, CD10, BCL6, CD21 or CD23 with or without cell surface marker analysis by flow cytometry.
The management of follicular lymphoma and breast cancer is also significantly different, which poses another challenge. There are currently no guidelines available for the concurrent management of breast carcinoma and lymphoma. Best practice statements recommend multidisciplinary team discussions and treatment decisions based on the initial presentation of each cancer type and the staging and prognosis of the concurrent malignancy/condition.
The current NCCN guidelines for follicular lymphoma recommend clinical observation for stage I and II follicular lymphomas vs involved site radiotherapy (ISRT) plus anti-CD 20 monoclonal antibody (rituximab, Obinutuzumab) therapy +/−chemotherapy if the clinical benefit outweighs the risk of toxicity, whereas for stages III or IV, treatment is only indicated if the patient is symptomatic or there is rapid progression of the disease or threatened end-organ damage. First-line systemic therapy includes bendamustine + Obinutuzumab or rituximab alone, CHOP (cyclophosphamide, vincristine, prednisone) + Obinutuzumab/rituximab, or Lenalidomide + rituximab. Surveillance is indicated with repeat histopathology and labs every 3–6 months for 5 years and then annually. Imaging, including CT scan chest/abdomen/pelvis with contrast, is recommended every 6 months for up to 2 years and then annually after 2 years [16].
Follicular lymphoma is non-curable. Initiation of systemic therapy can improve failure-free survival (FFS) but has not been shown to improve overall survival (OS). Patients with low to intermediate-risk Follicular Lymphoma International Prognostic Index (FLIPI) have a median progression-free survival (PFS) of 70–84 months (about 7 years) and 2-year overall survival (OS) of 94–98% [17]. In contrast, breast carcinoma is known to be curatable with currently available therapies. On average, breast cancer patients who have early-stage (I and II) breast cancer have over 90% PFS beyond 5 years [5].Current treatment guidelines for breast cancer are complex and vary for invasive vs non-invasive disease. Our focus here is on the management of hormone receptor-positive invasive breast cancer in post-menopausal women.
Treatment for invasive breast carcinoma according to the NCCN guideline is based on TNM staging. The mainstay of treatment remains surgery with modified radical mastectomy or lumpectomy with radiation therapy (breast-conserving therapy [BCT]). Recent studies have shown no survival difference between these 2 strategies, and BCT is the preferred treatment for early-stage breast cancer. Post-menopausal women with nodal involvement (pN1) who are candidates for chemotherapy should be assessed with a recurrence score based on the 21 gene RT PCR assay. A patient with a score of 26 or above should be started on adjuvant chemotherapy followed by endocrine therapy. However, nodal involvement (pN2 or pN3) already indicates a high recurrence risk. Therefore, the patient can be started on chemotherapy followed by endocrine therapy and does not need gene assay. Chemotherapy regimens in hormone receptor (HR)-positive and HER 2-negative invasive breast cancer include:dose-dense AC (doxorubicin+cyclophosphamide) followed by paclitaxelTC (docetaxel+cyclophosphamide).
Adjuvant endocrine therapy with aromatase inhibitors (anastrozole, exemestane, letrozole) or selective estrogen receptor modulators (SERM) like tamoxifen is recommended in all patients with HR-positive breast cancer. Data suggest that these agents decrease mortality by about 30% and the risk of recurrence by 50%. In post-menopausal women, aromatase inhibitors are preferred over SERM and are prescribed for a total of 5 years [18].
Therefore, the ideal approach is primarily to first treat the most biologically aggressive cancer, discussed by a multidisciplinary team including the surgeon, medical oncologist, pathologist, and radiation oncologist. All 3 of our patients presented with stage I-II follicular lymphomas with low to intermediate FLIPI and higher-risk breast cancer (stage II to III) requiring chemo-therapy and surgical interventions. They were all hormone receptor-positive and HER-2 receptor-negative, with a good expected prognosis. Hence, it was decided to proceed with breast cancer treatment first and observe the FL. To date, all 3 patients tolerated their systemic chemotherapy for breast cancer and did not have any FL imaging progression. We plan to continue surveillance and monitoring for both types of cancers.
Conclusions
The co-occurrence of breast cancer and lymphoma is rare and can pose a challenge to the treating oncologist, who should consider a second primary malignancy in cases of early breast cancer that presents with disseminated adenopathy. Choice of treatment should be based on the more aggressive disease and staging of the tumor, with close surveillance of the additional malignancy.
Figures
References:
1.. Coyte A, Morrison DS, McLoone P, Second primary cancer risk – the impact of applying different definitions of multiple primaries: Results from a retrospective population-based cancer registry study: BMC Cancer, 2014; 14; 272
2.. Buiatti E, Crocetti E, Acciai S, Incidence of second primary cancers in three Italian population-based cancer registries: Eur J Cancer, 1997; 33(11); 1829-34
3.. Rosso S, De Angelis R, Ciccolallo L, Multiple tumours in survival estimates: Eur J Cancer, 2009; 45(6); 1080-94
4.. Weir HK, Johnson CJ, Thompson TD, The effect of multiple primary rules on population-based cancer survival: Cancer Causes Control, 2013; 24(6); 1231-42
5.. Laudenschlager MD, Tyler KL, Geis MC, A rare case of synchronous invasive ductal carcinoma of the breast and follicular lymphoma: S D Med, 2010; 63(4); 123-25
6.. Niedermayr A, Gharehbaghi K, Pacher B, Coincidence of primary non-Hodgkin’s lymphoma and invasive lobular carcinoma of the breasts – clinical diagnosis and management: Acta Oncol, 1998; 37(3); 305-6
7.. Al-Hussaini MA, Al-Masad JK, Awidi AA, Carcinoma of breast co-existing with non-Hodgkin’s lymphoma of axillary lymph nodes: Saudi Med J, 2008; 29(1); 138-41
8.. Barranger E, Marpeau O, Uzan S, Antoine M, Axillary sentinel node involvement by breast cancer coexisting with B-cell follicular lymphoma in non-sentinel nodes: Breast J, 2005; 11(3); 227-28
9.. Benoit L, Arnould L, Collin F, Concurrent lymphoma and metastatic breast carcinoma in the axillary, confounding sentinel lymph-node biopsy: Eur J Surg Oncol, 2004; 30(4); 462-63
10.. Frei KA, Bonel HM, Forrer P, Primary breast lymphoma, contralateral breast cancer, and bilateral Brenner tumors of the ovary: Obstet Gynecol, 2002; 100(5 Pt 2); 1079-82
11.. Nishikawa A, Kasai H, Koyama Y, Synchronous ipsilateral carcinoma of the accessory mammary gland and primary lymphoma of the breast with subsequent rectal carcinoma: Report of a case: World J Surg Oncol, 2014; 12; 286
12.. Alakeel F, Lee E, Baird-Howell M, Easley S, Synchronous ductal carcinoma in situ and intravascular large B-cell lymphoma of the breast: Appl Immunohistochem Mol Morphol, 2019; 27(9); e91-e92
13.. Cuff KE, Dettrick AJ, Chern B, Synchronous breast cancer and lymphoma: A case series and a review of the literature: J Clin Pathol, 2010; 63(6); 555-57
14.. Zhong J, Di L, Zheng W, Synchronous breast cancer and breast lymphoma: Two case reports and literature review: Chin J Cancer Res, 2014; 26(3); 355-59
15.. Lister TA, Crowther D, Sutcliffe SB, Report of a committee convened to discuss the evaluation and staging of patients with Hodgkin’s disease: Cotswolds meeting: J Clin Oncol, 1989; 7(11); 1630-36
16.. , NCCN guidelines B-cell lymphoma May 5, 2021 Available from: https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf
17.. Kalli S, Semine A, Cohen S, American Joint Committee on Cancer’s Staging System for Breast Cancer, Eighth edition: What the radiologist needs to know: Radiographics, 2018; 38(7); 1921-33
18.. , NCCN guidelines breast cancer August 16, 2021 Available from: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf
Figures
In Press
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.953192
Case report 
Am J Case Rep In Press; DOI: 10.12659/AJCR.952818
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953608
Case report
Am J Case Rep In Press; DOI: 10.12659/AJCR.953068
Most Viewed Current Articles
07 Dec 2021 : Case report
22,364,578
DOI :10.12659/AJCR.934347
Am J Case Rep 2021; 22:e934347
06 Dec 2021 : Case report  174,245
174,245
DOI :10.12659/AJCR.934406
Am J Case Rep 2021; 22:e934406
21 Jun 2024 : Case report
119,744
DOI :10.12659/AJCR.944371
Am J Case Rep 2024; 25:e944371
07 Mar 2024 : Case report
64,648
DOI :10.12659/AJCR.943133
Am J Case Rep 2024; 25:e943133